Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
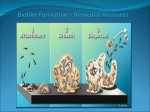
Original Investigation Microbiologic Trends and Biofilm Growth on Explanted Periorbital Biomaterials: A 30-Year Review David B. Samimi, M.D.*†, Brett P. Bielory, M.D.*, Darlene Miller, D.H.SC. M.P.H.*, and Thomas E. Johnson, M.D.* *Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, Florida; and †Eyesthetica, Oculofacial and Cosmetic Surgery Associates, Los Angeles, California, U.S.A. Purpose: To investigate microbiologic trends and role of biofilm on periorbital biomaterials surgically explanted for recalcitrant infection. Methods: A search of the Bascom Palmer Eye Institute, University of Miami Miller School of Medicine microbiology laboratory electronic database was conducted from 1980 to 2010. Culture results were analyzed from submitted periorbital biomaterials explanted for nonresolving infections or exposure. Random select samples cultured during the study were sent for electron microscopy. Results: Twenty-one explanted biomaterials were identified from 18 patients. Five orbital plate implants included 2 made of nylon, 1 of porous polyethylene, 1 of silicone, and 1 metallic. Of 4 anophthalmic socket sphere implants, 2 were silicone, 1 was porous polyethylene, and 1 was poly-2-hydroxyethyl methacrylate. Lacrimal intubation devices included 10 silicone stents and 2 pyrex glass Jones tubes. All biomaterials were culture positive with 40 total isolates identified. The most common organisms overall were Mycobacterium chelonae (N = 9), Staphylococcus aureus (N = 8), and Pseudomonas aeruginosa (N = 3). One hundred percent of orbital spheres had Gram-positive organisms, 90% of lacrimal silicone stents grew atypical mycobacterium, and 60% of orbital plates were culture positive for yeast species. Mixed organism growth was documented on 58% of the specimens. Ten of 12 implants (83%) examined with electron microscopy exhibited organisms encased in glycocalyx, suggestive of biofilm. Conclusions: A diverse array of microorganisms can colonize biomaterials implanted within the orbit and lacrimal drainage system. The authors’ study showed that the majority of infected periocular and orbital alloplastic implants display biofilm when studied with electron microscopy (83%). The cultured organism type depended on the implant location and composition. Most infected silicone lacrimal stents grew atypical mycobacterium, whereas infected orbital fracture repair plates demonstrated yeast species. Biofilms are known to be antibiotic resistant, explaining the need to explant most infected alloplastic implants. Further research concerning treatment of biofilms may prevent explantation and improve surgical outcomes. (Ophthal Plast Reconstr Surg 2013;29:376–381) Accepted for publication April 24, 2013. Presented at the American Society of Ophthalmic Plastic and Reconstructive Surgery (ASOPRS) 40th Annual Fall Scientific Symposium on October 21–22, 2009, in San Francisco, CA. The authors have no financial or conflicts of interest to disclose. Address correspondence and reprint requests to David B. Samimi, M.D., Eyesthetica, 1513 South Grand Avenue, Suite 200, Los Angeles, CA 90015. E-mail: [email protected] DOI: 10.1097/IOP.0b013e31829a7313 376 T he expanding availability of implantable biomaterials has increased the use of synthetic material in oculofacial surgery. Biomaterials, such as acrylic, nylon, glass, silicone, hydroxyapatite, and porous polyethylene, provide the surgeon with an expanding armamentarium of surgical tools for treating orbital and periocular disease. They also may provide microorganisms with an immune-privileged, abiotic surface for growth. Recalcitrant infections associated with implants have been described in almost every part of the body where they have been used. The presence of biofilms on implants in ophthalmology has been documented on corneal sutures, punctal plugs, lacrimal intubation devices, scleral buckles, and intraocular lenses.1–7 The purpose of this study was to characterize the microbiology of clinically significant periorbital biomaterial infection and document the presence of biofilm by direct visualization with electron microscopy. METHODS A retrospective review of the electronic Bascom Palmer Eye Institute Microbiology Laboratory database was conducted between 1980 and 2010. Culture results from periorbital biomaterial submitted to the microbiology laboratory for culture at the time of explantation were recorded. Clinical charts were reviewed and information regarding demographics, clinical course, and antibiotic usage were collected. The study was approved by the University of Miami Institutional Review Board. The culture protocol consisted of vortexing implant material in thioglycollate broth and inoculating aliquots onto solid (chocolate, 5% sheep blood, sabouraud, Lowenstein-jensen) and liquid (thioglycollate broth and SeptiChek AFB [Becton Dickinson, Franklin Lakes, NJ, U.S.A.]) culture media. Preliminary identification was confirmed using Gram stains, acid-fast stains, growth rate, and biochemical profiles. Definitive identification of Mycobacteria was performed by either MAYO Medical Labs (Rochester, MN, U.S.A.) or Focus Diagnostic Labs (Cypress, CA, U.S.A.) using polymerase chain reaction or highperformance liquid chromatography. Biomaterials and aliquots of the microbiology specimen that were available while conducting this review were placed in formalin and sent to the Center for Biofilm Engineering in Bozeman Montana or the University of Miami Center for Advanced Microscopy for scanning electron microscopy for detection of biofilm. Specimens sent to Miami Center for Advanced Microscopy were processed by fixing in 10% formalin for at least 1 hour, then post fixed in 1% Osmium Tetroxide in phosphate-buffered saline buffer for 30 minutes. After 3 progressive rinses in phosphate-buffered saline for 10 minutes each, the samples were dehydrated in an ethanol series. The specimens were critically dried with hexamethyldisilazane, allowed to outgas overnight, and sputter coated with Palladium before imaging. Scanning electron microscopy at Miami Center for Advanced Microscopy used a Phillips XL-30 Ophthal Plast Reconstr Surg, Vol. 29, No. 5, 2013 Ophthal Plast Reconstr Surg, Vol. 29, No. 5, 2013 Periorbital Implant Infection TABLE 1. Clinical data Age, mean (range) Immunosuppression Diabetes mellitus Dialysis or HIV Autoimmune disorder Age >65 years Total weeks implanted Median (range) Weeks symptomatic before explantation Median (range) Postexplant weeks to symptom resolution Median (range) Pre-explantation antibiotic treatment attempted Organisms that should have been sensitive based on culture Overall (N = 21) Plate (n = 5) Spheres (n = 4) Jones tube (n = 2) Stent (n = 10) 57 (5–81) 58 (38–73) 41 (5–64) 79 (77–81) 58 (32–79) 2 (10%) 0 2 (10%) 10 (48%) 1 (20%) 0 1 (20%) 3 (60%) 0 0 0 0 0 0 0 2 (100%) 1 (10%) 0 1 (10%) 5 (50%) 13 (2–1,924) 60 (24–1,924) 5 (4–208) 36 (12–60) 11 (2–128) 19 (2–105) 63 (8–156) 2 (2–105) 33 (10–55) 4 (1–8) 1 (1–62) 76% 44% 1 (1–4) 100% 40% 1 (1–1) 50% 0 9 (1–16) 100% 50% 9 (1–62) 70% 57% HIV, human immunodeficiency virus. ESEM FEG (Phillips, Amsterdam, the Netherlands) at varying kilovolts. Scanning technique and equipment at Center for Biofilm Engineering was similar and has been described previously.8 Images were examined in a masked fashion by one of the authors, the director of the microbiology laboratory (D.M.), for evidence of organisms growing in biofilm. overall had pre-explantation antibiotic treatment. Of those treated, 44% of infections should have been sensitive to the given antibiotic based on postexplantation culture results. All biomaterials were culture positive with 40 total isolates identified (Table 2). The most common organisms overall were Mycobacterium chelonae, Staphylococcus aureus, and Pseudomonas aeruginosa. One hundred percent of orbital spheres had culture-confirmed Gram-positive organisms, 90% of lacrimal silicone stents grew atypical mycobacterium, and 60% of orbital plates were culture positive for yeast species (Fig. 1). Multiple organisms were growing on 58% of the implants. Twelve implants were imaged with electron microscopy: 4 orbital spheres, 4 plates, and 4 lacrimal stents. Organisms encased in matrix on the surface of the implants suggestive of biofilm was seen on 10 (83%) of the implants imaged (Figs. 2–4). RESULTS Twenty-one explanted biomaterials were identified from 18 patients. (Table 1) Five orbital plates included 2 nylon, 1 porous polyethylene, 1 silicone, and 1 metallic. Of 4 anophthalmic socket sphere implants, 2 were silicone, 1 was porous polyethylene, and 1 was poly2-hydroxyethyl methacrylate. Lacrimal intubation devices included 10 silicone stents and 2 pyrex glass Jones tubes. Fourteen implants (67%) were from female patients. Nine (43%) patients were Hispanic, 7 (33%) Caucasian, 0 African American, and 5 (24%) others. Twelve (57%) specimens were from the OD. Average follow-up period was 65 weeks (range 0–350 weeks). Median symptomatic weeks before explantation was longest among the orbital plate (63) and Jones tube group (33). Postexplantation time to symptom resolution was greatest in the Jones tube and lacrimal silicone stent groups, both 9 weeks. Seventy-six percent of patients DISCUSSION The authors’ study characterized microbiologic trends from a variety of infected periorbital alloplastic implants needing surgical removal after recalcitrant infection in South Florida. We discovered the predominance of Gram-positive isolates on TABLE 2. Microbiology of explanted biomaterials from periorbital infections Isolates Gram positive Staphylococcus aureus S. epidermidis Gram negative Achromobacter xylosoxidans Pantoea agglomerans Pseudomonas aeruginosa Serratia marcescens Stenotrophomonas maltophilia Mycobacteria Mycobacterium chelonae Fungi Candida species Trichosporon species Total isolates Orbital plates (N = 5) Orbital spheres (N = 4) Lacrimal stents (N = 10) Jones tubes (N = 2) Total 1 1 4 — 2 1 1 — 8 2 2 — 2 — — — 1 — — — — — — 1 3 — — 1 1 — 2 1 3 2 3 1 1 8 — 10 2 1 10 — — 6 — — 15 — — 3 2 1 34* *Forty total isolates, 6 individually occurring isolates excluded from table: Acinetobacter baumannii, Achromobacter xylosoxidans, Streptococcus intermedius, Corynebacterium diphtheriae, Corynebacterium amycolatum, Enterobacter. © 2013 The American Society of Ophthalmic Plastic and Reconstructive Surgery, Inc. 377 Ophthal Plast Reconstr Surg, Vol. 29, No. 5, 2013 D. B. Samimi et al. FIG. 1. Organism by biomaterial type. Sums equal greater than 100% due to multiple isolates on the majority of implants. orbital sphere implants, yeast on the majority of orbital plates, and a high prevalence of atypical mycobacterium on clinically infected lacrimal silicone stents. The longest time period between implant removal and resolution of infection-related symptoms occurred with lacrimal implants. This study also found that the period between implantation and removal was longest in orbital plate group. Electron microscopic imaging was suggestive for biofilm in the majority of implants studied. Many factors predispose certain organisms to colonize a given class of implants. These include the implant material, native flora in the region of the implant, and organism compatibility with growth in a biofilm. All infected orbital spheres exhibited Gram-positive isolate culture results. This likely relates to the predominance of Gram-positive organisms routinely found on the conjunctival surface.9,10 Staphylococcus isolates from the conjunctiva have also been shown to exhibit increased biofilm formation ability in comparison to isolates from the rest of the face.11 Yeast species were found on 3 of 5 orbital plates and not on any other class of implants. A positive medical history for immunosuppression or high-risk setting for infection was evident in all 3 patients: 1 with Wegener granulomatosis on immunosuppressant agents, 1 with diabetes mellitus, and a third with a history of prison incarceration at the time of infection. Immunosuppression correlates with yeast growth in the paranasal sinuses adjacent to where orbital plates are placed.12 Chronic or later onset rhinosinusitis may partially explain the longer period between implantation and removal noted with orbital plates. Studies of sinus mucosa have shown the presence of biofilm that may provide a reservoir for native flora to infect an implant.13 One of the patients had a silicone orbital plate that grew S. aureus and a history of chronic rhinosinusitis. He had undergone multiple sinus surgeries after implant placement and had suffered 5 episodes of orbital cellulitis treated with intravenous antibiotics before explantation of the plate. Lacrimal silicone stent infection with atypical mycobacterium was first described by Rootman et al.14 in 1989. The authors’ study found atypical mycobacterium on 90% of FIG. 2. Infected porous polyethylene orbital floor implant culture positive with Mycobacterium chelonae, Pseudomonas aeruginosa, and Trichosporon species in a patient with Wegener granulomatosis. A, Gross image. B, Electron microscopy of porous surface. C, High power image showing sheets of rod-shaped organisms (blue arrow) and overlying hyphae (yellow arrow) consistent in size and morphology with culture results. 378 © 2013 The American Society of Ophthalmic Plastic and Reconstructive Surgery, Inc. Ophthal Plast Reconstr Surg, Vol. 29, No. 5, 2013 Periorbital Implant Infection FIG. 3. Electron microscopy images. A and B, Metal screws from metal-coated porous polyethylene orbital plate implant removed 6 months after placement, culture positive with Pseudomonas aeruginosa and Candida parapsilosis. Organisms and surrounding deposits consistent in size and morphology with yeast seen on high power images of surface. C and D, Cocci-shaped organisms encased in biofilm matrix on the surface of methicillin-resistant Staphylococcus aureus–infected poly-2-hydroxyethyl methacrylate material AlphaSphere implant surgically explanted 1 month after placement. infected stents. The organism may be subclinically present in many patients with history of nasolacrimal duct obstruction necessitating dacryocystorhinostomy surgery or may develop externally during or after implantation. The majority of dacryocystitis cases are caused by Gram-positive flora.15,16 A study of microbial growth on lacrimal silicone stents by Kim et al.17 found mostly Gram-positive organisms, but a correlation of P. aeruginosa with postoperative membranous ostia obstruction. A high prevalence of underlying mycobacterial infection has not been documented. Atypical mycobacteria are ubiquitous throughout the environment and commonly found in municipal water supplies.18–20 A study by Feazel et al.21 involved swabbing the interior surface of showerheads from 9 regions across the country and used rRNA analysis to identify microbial species. Nontuberculous mycobacterium were the most common class of organisms found. Theoretically, daily exposure to aerosolized FIG. 4. Progressively closer images of infected lacrimal silicone stent that caused chronic mucopurulent dacryoconjunctivitis. Culture isolates included Mycobacterium chelonae, Serratia, and Corynebacteria. A, Sectioned lumen with biofilm plaques. B and C, Depth of 1 plaque (white arrow). D, Tubular-shaped organisms encased within protective matrix seen on surface of plaque (black arrow). © 2013 The American Society of Ophthalmic Plastic and Reconstructive Surgery, Inc. 379 Ophthal Plast Reconstr Surg, Vol. 29, No. 5, 2013 D. B. Samimi et al. mycobacteria, while showering in the presence of a silicone foreign body, may predispose these patients to clinically significant infection. Other possible explanations include contaminated tubes or silk sutures at the time of implantation, contaminated make up, preexisting mycobacterial dacryocystitis, or nasal colonization with atypical mycobacterium. Patients with infected lacrimal silicone stents and Jones tubes both had a median of 9 weeks of residual symptoms after implant removal. Common symptoms were discharge, erythema, and pain. These symptoms may be related to bacterial reservoirs from lacrimal or nasal biofilm residua or from scarring of the lacrimal system with recurrent nasolacrimal duct obstruction and dacryocystitis. The longer duration of symptoms may also be related to the extraorbital location of the lacrimal system making residual or resolving infection more evident to the patient and clinician. The majority of bodily infections involve biofilm, a heterogeneous collection of microorganisms encased within a protective extracellular polymeric substance matrix derived from host and bacterial materials.7 Within biofilm exist complex communities exhibiting cell-to-cell communication, varying degrees of gene expression, and commonly multiple species acting synergistically to survive harsh environmental conditions.22 Cells near the biofilm surface have the most exposure to nutrients and are the most metabolically active, whereas those deeper in the biofilm have access to nutrients through intricate channel networks but are relatively dormant.7 The heterogeneous degree of metabolic activity and physical extracellular polymeric substance matrix fortification confer microorganism protection against adverse conditions. Bacteria in biofilm are up to 1,000 times more resistant to antibiotics than those studied in the classic laboratory planktonic form.7,23 Biofilms have previously been described on a wide variety of periorbital implants including punctal plugs, lacrimal intubation devices, and scleral buckles.1,3–5,7 Electron microscopy examination of most implants in the authors’ study suggested presence of biofilm. The 3 most common organisms overall, M. chelonae, S. aureus, and P. aeruginosa, are all avid biofilm producers. Many implants included in the study were recalcitrant to antibiotic therapy to which the organism isolate was sensitive in laboratory culture. The widely held paradigm of treating infection based on laboratory sensitivities does not fit implant-related infection.24 The definitive treatment strategy for implant-related infection is implant removal and appropriate antibiotic therapy.23,24 Other intervention strategies include the prevention of initial device contamination, minimization of initial microbial cell attachment, and use of antibiotics with increased penetrance and efficacy against microbial biofilm.23,25 Strict aseptic technique should always be followed when implanting foreign biomaterial. Once implanted, all foreign bodies are quickly coated by host matrix molecules such as fibrinogen, fibronectin, and collagen.7,23 The fate of the available surface is then a contest between tissue cell integration and microbial adhesion and subsequent biofilm formation.26 Implant design modifications, such as alteration in surface polarity, surface texture, and antibiotic coating, have been shown to discourage bacterial biofilm growth.27–29 Design alterations to inhibit microbial growth are not without their problems. Sufficient antibiotic must be incorporated for the lifetime of the device, and long-term presence of antimicrobials may promote resistant organisms.25 Although antibiotic efficacy against biofilm-embedded organisms is limited, some antibiotics demonstrate more efficacy than others. Daptomycin, minocycline, and tigecycline show increased efficacy against biofilm-embedded methicillin-resistant S. aureus when compared with linezolid or vancomycin in vitro.30 380 The literature also suggests a synergistic effect when adding rifampin or N-acetylcysteine.30,31 Further studies regarding the effective prevention and treatment strategies are needed. The main weaknesses of the authors’ study relate to the retrospective nature of their data search. Relevant infections may have been missed in their microbiology electronic database review. Many removed implants are sent to pathology instead of the microbiology laboratory. It would have also have been useful to report the incidence of successfully treated implantrelated infections in their patient population during the same period. This data would be difficult to accurately ascertain over the 30-year interval. Given the relatively small sample size of the study and referral nature of the patient population at their institution, the study was also not ideally structured to extrapolate conclusions regarding incidence and risk factors for infection. Comparative controls would be useful to further clarify the pathogenicity of the organisms and biofilm in their study. Also, the findings from South Florida may not generalize to other patient populations. Biofilm growth likely plays a significant role in clinically significant periorbital implant infection. Further research in effective biofilm prevention and treatment strategies may improve surgical outcomes. REFERENCES 1.Yokoi N, Okada K, Sugita J, et al. Acute conjunctivitis associated with biofilm formation on a punctal plug. Jpn J Ophthalmol 2000;44:559–60. 2. Suzuki T, Iihara H, Uno T, et al. Suture-related keratitis caused by Corynebacterium macginleyi. J Clin Microbiol 2007;45:3833–6. 3. Sugita J, Yokoi N, Fullwood NJ, et al. The detection of bacteria and bacterial biofilms in punctal plug holes. Cornea 2001;20:362–5. 4. Parsa K, Schaudinn C, Gorur A, et al. Demonstration of bacterial biofilms in culture-negative silicone stent and jones tube. Ophthal Plast Reconstr Surg 2010;26:426–30. 5. Holland SP, Pulido JS, Miller D, et al. Biofilm and scleral buckleassociated infections. A mechanism for persistence. Ophthalmology 1991;98:933–8. 6.Kobayakawa S, Jett BD, Gilmore MS. Biofilm formation by Enterococcus faecalis on intraocular lens material. Curr Eye Res 2005;30:741–5. 7. Behlau I, Gilmore MS. Microbial biofilms in ophthalmology and infectious disease. Arch Ophthalmol 2008;126:1572–81. 8.James GA, Swogger E, Wolcott R, et al. Biofilms in chronic wounds. Wound Repair Regen 2008;16:37–44. 9. de Kaspar HM, Kreidl KO, Singh K, et al. Comparison of preoperative conjunctival bacterial flora in patients undergoing glaucoma or cataract surgery. J Glaucoma 2004;13:507–9. 10. Graham JE, Moore JE, Jiru X, et al. Ocular pathogen or commensal: a PCR-based study of surface bacterial flora in normal and dry eyes. Invest Ophthalmol Vis Sci 2007;48:5616–23. 11. Suzuki T, Kawamura Y, Uno T, et al. Prevalence of Staphylococcus epidermidis strains with biofilm-forming ability in isolates from conjunctiva and facial skin. Am J Ophthalmol 2005;140: 844–50. 12. Malani PN, Kauffman CA. Invasive and Allergic Fungal Sinusitis. Curr Infect Dis Rep 2002;4:225–32. 13. Post JC, Hiller NL, Nistico L, et al. The role of biofilms in otolaryngologic infections: update 2007. Curr Opin Otolaryngol Head Neck Surg 2007;15:347–51. 14.Rootman DS, Insler MS, Wolfley DE. Canaliculitis caused by Mycobacterium chelonae after lacrimal intubation with silicone tubes. Can J Ophthalmol 1989;24:221–2. 15.Coden DJ, Hornblass A, Haas BD. Clinical bacteriology of dacryocystitis in adults. Ophthal Plast Reconstr Surg 1993;9: 125–31. 16. Mills DM, Bodman MG, Meyer DR, et al.; ASOPRS Dacryocystitis Study Group. The microbiologic spectrum of dacryocystitis: a national study of acute versus chronic infection. Ophthal Plast Reconstr Surg 2007;23:302–6. © 2013 The American Society of Ophthalmic Plastic and Reconstructive Surgery, Inc. Ophthal Plast Reconstr Surg, Vol. 29, No. 5, 2013 17.Kim SE, Lee SJ, Lee SY, Yoon JS. Clinical significance of microbial growth on the surfaces of silicone tubes removed from dacryocystorhinostomy patients. Am J Ophthalmol 2012:153: 253–7.e1. 18. Vaerewijck MJ, Huys G, Palomino JC, et al. Mycobacteria in drinking water distribution systems: ecology and significance for human health. FEMS Microbiol Rev 2005;29:911–34. 19. Le Dantec C, Duguet JP, Montiel A, et al. Occurrence of mycobacteria in water treatment lines and in water distribution systems. Appl Environ Microbiol 2002;68:5318–25. 20. Hilborn ED, Covert TC, Yakrus MA, et al. Persistence of nontuberculous mycobacteria in a drinking water system after addition of filtration treatment. Appl Environ Microbiol 2006;72:5864–9. 21.Feazel LM, Baumgartner LK, Peterson KL, et al. Opportunistic pathogens enriched in showerhead biofilms. Proc Natl Acad Sci U S A 2009;106:16393–9. 22. Stoodley P, Sauer K, Davies DG, et al. Biofilms as complex differentiated communities. Annu Rev Microbiol 2002;56:187–209. 23. Aslam S. Effect of antibacterials on biofilms. Am J Infect Control 2008;36:S175.e9–11. 24. Darouiche RO. Treatment of infections associated with surgical implants. N Engl J Med 2004;350:1422–9. Periorbital Implant Infection 25. Smith AW. Biofilms and antibiotic therapy: is there a role for combating bacterial resistance by the use of novel drug delivery systems? Adv Drug Deliv Rev 2005;57:1539–50. 26.Gristina AG. Biomaterial-centered infection: microbial adhesion versus tissue integration. Science 1987;237:1588–95. 27. Jang CH, Park H, Cho YB, et al. The use of piperacillin-tazobactam coated tympanostomy tubes against ciprofloxacin-resistant Pseudomonas biofilm formation: an in vitro study. Int J Pediatr Otorhinolaryngol 2009;73:295–9. 28. Berry JA, Biedlingmaier JF, Whelan PJ. In vitro resistance to bacterial biofilm formation on coated fluoroplastic tympanostomy tubes. Otolaryngol Head Neck Surg 2000;123:246–51. 29. Karlan MS, Mufson RA, Grizzard MB, et al. Potentiation of infections by biomaterials: a comparison of three materials. Otolaryngol Head Neck Surg 1981;89:528–34. 30. Raad I, Hanna H, Jiang Y, et al. Comparative activities of daptomycin, linezolid, and tigecycline against catheter-related methicillinresistant Staphylococcus bacteremic isolates embedded in biofilm. Antimicrob Agents Chemother 2007;51:1656–60. 31. Aslam S, Trautner BW, Ramanathan V, et al. Combination of tigecycline and N-acetylcysteine reduces biofilm-embedded bacteria on vascular catheters. Antimicrob Agents Chemother 2007;51:1556–8. © 2013 The American Society of Ophthalmic Plastic and Reconstructive Surgery, Inc. 381