Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
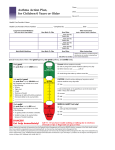
Talking to Parents about their Children’s Asthma Sally E. Findley Professor of Clinical Population and Family Health (in Pediatrics) Mailman School of Public Health Columbia University Asthma Basics for Children, Mailman School of Public Health, Columbia University Asthma Prevalence Increased 1980-99 • Annual prevalence of asthma has increased steadily between 1980-1996, from 31.4 to 38.4 (per 1000). • Asthma rates are 1.14 times higher among communities of color. • Highest prevalence is among young children, 5-14 years of age (56.4 per 1000). • Source: MMWR Surveillance Summaries, March 29, 2002/51 (SS01), 1-13. Asthma Basics for Children, Mailman School of Public Health, Columbia University Self-reported asthma (per 1000) US Annual Prevalence of Selfreported Asthma Episodes by Age, 1980-1999 80 70 60 50 40 30 20 10 0 0-4 5 -14 15-34 35-64 65+ Age in Years 1980 1990 1996 1999 Source: MMWR Surveillance Summaries, March 29,2002, 51(SS01); 1-13. Asthma Basics for Children, Mailman School of Public Health, Columbia University Self-reported asthma (per 10,000) US Asthma-Related Emergency Department Visits, Hospitalizations, and Office Visits by Age, 1999 160 140 120 100 80 60 40 20 0 0-4 5 -14 15-34 35-64 65+ Age in Years Hospitalizations Office Visits ED Visits Source: MMWR Surveillance Summaries, March 29,2002, 51(SS01); 1-13. Asthma Basics for Children, Mailman School of Public Health, Columbia University The youngest children bear a disproportionate share of the asthma burden • Children 0-4 years have the highest ED visit and hospitalization rates • Asthma management programs need to expand down to the younger age groups Asthma Basics for Children, Mailman School of Public Health, Columbia University Cities such as NYC have much higher asthma hospitalization rates Rate per 1,000 Population Asthma Hospitalization Rates 1995 12 10 8 6 4 2 0 US NYS (not including NYC) NYC Source: New York City Childhood Asthma Initiative, NYC DOH Asthma also keeps children from school • 14 million school-days are lost per year for children, 1996-99 • Each year a child with asthma can expect to be absent 4 days per year due to asthma. • 24% of school-age children also suffer activity limitation due to their asthma Asthma Basics for Children, Mailman School of Public Health, Columbia University Asthma episodes can be prevented • We do not know yet how to prevent or cure asthma, but asthma can be managed to reduce the severity and frequency of asthma episodes. • Current high rates of asthma-related hospitalizations, ED visits and school absences can be reduced through providing access to appropriate management of asthma. Asthma Basics for Children, Mailman School of Public Health, Columbia University Background to Our Approach • In 1999, through the Northern Manhattan Community Voices project we began working with a group of NYC early childhood centers and Head Starts to help them manage asthma. • We have developed a program to train the staff, identify children with asthma, and assist the parents in developing a strong partnership with their doctors and the staff to manage their children’s asthma. • Presentation today grows out of this work. Asthma Basics for Children, Mailman School of Public Health, Columbia University What did Educators want? • A systematic way of knowing if children had asthma (not just a cold or flu). • Know what to do when children had exacerbations • Help parents overcome fears and better manage asthma so children would not have to stay home when having asthma symptoms Asthma Basics for Children, Mailman School of Public Health, Columbia University What did Parents Want? • Prompt diagnosis of asthma to avoid the “dark time” of ER trips without knowing what is going on. • More explanations about medications: how they work, any side effects, limits to their effectiveness • More advice on what to do besides medications, including combining with traditional treatments • Assistance in dealing with indoor environmental triggers Asthma Basics for Children, Mailman School of Public Health, Columbia University Shared Desire for Confidence in Asthma Management • Know who has asthma • Have confidence that the management program is helping the child • Feel good about how they are handling asthma exacerbations at home or school Asthma Basics for Children, Mailman School of Public Health, Columbia University The Bottom Line for Parents and Educators: Make asthma less scary for the children Asthma Basics for Children, Mailman School of Public Health, Columbia University Gaps in the Application of Asthma Treatment Guidelines • NHLBI guidelines released in 1997 outline both diagnostic and treatment guidelines, yet surveys of physicians repeatedly show that many patients do not receive the recommended management. • The guidelines are not followed because of: – Lack of awareness or familiarity w. details – Lack of agreement with guidelines – Lack of self-efficacy to carry it out properly – Lack of confidence in outcomes – Inertia of previous practice • Source: Cabana and Lewis. Improving Physician Adherence to Asthma Guidelines. JCOM. 8(3), March 2001. Asthma Basics for Children, Mailman School of Public Health, Columbia University What makes application of the guidelines so hard for physicians? • Hard to Track: People with asthma usually are asymptomatic for most of the time, and asthma can be overlooked during office visits. • Continuity of Care problematic: Many episodes occur at night, when physician offices are closed, leaving treatment to on-call and ED services. • Medication Tailoring: Medications need to be tailored to individual asthma severity. • Medications only part of the solution: Part of the management is in trigger management at home and school. Asthma Basics for Children, Mailman School of Public Health, Columbia University What makes asthma management so hard for parents/patients? • Here today, gone tomorrow: Periods of symptoms interspersed with symptom-free periods • Daily medications, even when feeling fine • Unpredictability: Don’t know exactly what triggers the episode • Complicated medication plan, varies with symptom intensity and disease severity • Need to monitor asthma symptoms, the signals for medication changes • Fears about medication side-effects • Medications only part of plan: Trigger reduction also needed. Helping parents and providers move beyond the difficulties • Promote early diagnosis • Develop tools to clarify and simplify the complicated medication management steps • Find ways to build asthma management into a regular routine, both for providers and patients. • Promote the reduction of environmental and behavioral triggers to asthma in the child’s daily life Asthma Basics for Children, Mailman School of Public Health, Columbia University Physician Asthma Care Education Program • PACE Program to help physicians talk about asthma with parents/patients, proven effective in studies conducted by Columbia University researchers in work with NYC practices • Outlines clear steps for incorporating NHLBI recommendations into daily practice • Promotes communication strategies for promoting family and self-management of asthma. Source: Clark, NM et al. “Impact of education for physicians on patient outcomes.” Pediatrics 1998; 101: 831-36. Asthma Basics for Children, Mailman School of Public Health, Columbia University PACE Suggestions for Talking with Parents about Asthma • Be attentive: Make eye contact, sit same level, no desk or barriers between you, lean into the conversation • Ask open-ended questions: What about asthma is hard for you or your child? • Get fears out on the table and deal with fears and concerns right away • Be reassuring • Share information interactively • Tailor the regimen to the family’s daily routines • Plan how the family and you will make decisions together • Set goals for asthma treatment: Find out what the family wants to achieve Explaining Asthma • Provider message: Explain what happens during an asthma attack – Inflammation: Airway lining swells and produces too much mucus – Bronchospasm: Airway muscles squeeze too much • Asthma episodes are reversible • Parent/Patient message: • Wants an explanation that takes away the mystery about asthma, so can “see” what is going on in the lungs • Wants to be reassured that asthma is manageable and can get better Asthma Basics for Children, Mailman School of Public Health, Columbia University Communication Tips for Explaining Asthma • Make it simple and use pictures of airways • Use the “fist” example, asking parent/patient to do it with you. • Convey the dynamic of open/shut airways Asthma Basics for Children, Mailman School of Public Health, Columbia University Asthma Can Be Managed: Key Message • With proper therapy, the child can be symptom free • Goal is to use as little medicine as possible, increasing on an as-needed basis. • Long-term goal of reducing or even stopping regular medication • Emphasis on as little as possible addresses parents’ fears of overmedication and “dependence” Asthma Basics for Children, Mailman School of Public Health, Columbia University Explain About Quick-Relief Medications • Provider message: – Quick- relief medications act fast, so that breathing is easy again within minutes – Quick-relief medications relax the muscles after they have tightened during an attack – Parents are in charge of helping their children breathe through the quick-relief medications • Parent Message: • Know that medicines will open up lungs and child won’t suffocate • Know that reaction is not instant; may take a few minutes • Quick relief medicines are parents’ ticket to helping child breathe Asthma Basics for Children, Mailman School of Public Health, Columbia University Communication Tip for QuickRelief Medications • Use a physical example: Unclamp fist to show how medicines work • Ask parent about fears about child during an asthma episode • Discuss concerns parents may have about medications – Jitteriness; anxiety – Other side effects parents may fear (“dependence”) • Be accurate about risks but reinforce message that medicines work! Asthma Basics for Children, Mailman School of Public Health, Columbia University Explaining about Controller Medications • Provider Message: • Anti-inflammatory medicines don’t relieve symptoms • Do reduce inflammation and prevent frequent or severe episodes • Needed if asthma symptoms more than every 2 months • Effective only if taken regularly • Parent Message: • Anti-inflammatory meds are like a flu shot, to help keep away the “bad” asthma episodes • Anti-inflammatory medicines are like vitamins; they need to be taken all the time, even if not sick Asthma Basics for Children, Mailman School of Public Health, Columbia University Communication Tips about Controller Medicines • Explain the different types of controllers (parents want to know the names), and why more than one may be used • Convey clearly information about any risks or side effects • Discuss fears about medication “dependence” – Low Doses of Inhaled Corticosteroids do not cause side effects – Not the same as the body-building steroids • Emphasize safety of the medications when used as prescribed on the plan. Asthma Basics for Children, Mailman School of Public Health, Columbia University Talking about Alternative Asthma Treatments • Provider Message: • Asthma medications work and are safe when used as prescribed. • Traditional teas and herbal remedies can also be used, but not instead of medications. • Work out how the two can be paired, if parents wish. • Parent Message: • Needs to hear that it is OK to use traditional remedies with medications • Sense of respect for own traditions when provider brings up alternative therapies Asthma Basics for Children, Mailman School of Public Health, Columbia University Asthma Action Plan as a Tool • Asthma Action Plan is a problem solving tool. • Plan is based on information from both parent and provider – Parent/patient: Symptoms in each zone; triggers – Provider: Medications and “action steps” • Parent/patient involvement in developing the plan will increase chance that is used appropriately. – Makes sure “fits” for the family – “What if” helps the family see how it can help solve asthma management problems Asthma Basics for Children, Mailman School of Public Health, Columbia University Developing the Asthma Action Plan • Begin filling out the asthma action plan as you talk about each medication, so that you build the plan as you go. (simpler, easier for parents to stay with you) • Give the daily dose level for the child • Outline how to change the quick relief doses if the child becomes symptomatic – Use the stop light image to categorize normal (green), caution (yellow), and danger (red) • Give the limits for quick relief medications – maximum sets of 4 puffs per day Asthma Basics for Children, Mailman School of Public Health, Columbia University Example of An Asthma Action Plan Asthma Zone Symptoms Medications How much? What else? GO Good breathing Sleep at night Peakflow>80% Quick Relief 2 puffs X 2 /day Controller 2 puffs X2 / day Child can play & go to school Caution Cough Wheeze Peak flow <80% Quick Relief 4 puffs now & 4Xday Controller 4 puffs 2X/day Call doctor; watch child See doctor to change meds Danger Asthma worse fast; Meds don’t work Peakflow<50% Quick Relief 4 puffs right now Controller 4 puffs bid Urgent call to doctor; go to ED if can’t reach doctor Communication Tips for the Asthma Action Plan • Color Code the Explanation • Show what the different colors mean in terms of the child’s symptoms • Explain how to use the plan to adjust medications • Give parent confidence to read child’s symptoms • Make sure parent knows you can be called if parent has questions, and must be called if danger zone. Asthma Basics for Children, Mailman School of Public Health, Columbia University Review Plan with Parents/Patients • The plan is only a piece of paper if you don’t help the parent use it. • Underscore that the plan is tailored especially for their child • Give example of how to use the plan if child gets a cold or flu – Shift preventively into Yellow Zone medications • Reassure parent that you are always there if not sure what to do. • Make sure parent knows how to reach you 24 hours a day. Asthma Basics for Children, Mailman School of Public Health, Columbia University Practice Using the Plan • Make sure parent understands how to “read” child’s breathing in each zone • Encourage parent to talk often to child about their breathing • Go over what to do if breathing changes • Ask parent to identify when/how meds will be given in daily routine • Ask the parent to do a “mock” trial with a nurse on changing symptoms Asthma Basics for Children, Mailman School of Public Health, Columbia University Asthma Action Plans Need to be Updated • Follow-up call to parents w/in 1 month • Ask parents to come in to review plan regularly to make sure it is still right • Ask parents to come in for a medication change if symptoms persist or worsen. – Stays in “yellow” zone too long – Doesn’t sleep through night – Asthma triggered by play Asthma Basics for Children, Mailman School of Public Health, Columbia University Explaining How to Take Medicines • Provider Message: • Demonstrate how to use inhaler and spacer • Show how to use peak flow meter • Give step-by-step instructions • Parents Message: • Need to feel comfortable with the “technology” • Need to know how/where to get spacers, etc. • What to do if run out of medicine Asthma Basics for Children, Mailman School of Public Health, Columbia University Communication Tips on Medication Use • Ask parent to demonstrate technique in the office • Reassure parent and child that spacer is meant to allow slow, easy intake of medication • Reassure parent about using alternative treatments with medications (teas, herbal remedies) Asthma Basics for Children, Mailman School of Public Health, Columbia University Explaining Peak Flow Meters • Provider Message: • Peak flow meter helps identify breathing changes before an episode occurs • Useful only if breathing is monitored regularly • Not used in children under age 6 • Parent Message: • Peak flow meter signals what’s going on inside the lungs before it gets bad • Peak flow meter use needs to be a habit Asthma Basics for Children, Mailman School of Public Health, Columbia University Communication Tips for Peak Flow Meters • Use a small, easy to use meter • Give steps to establish child’s personal best – Best of three puffs every morning for 2-3 weeks when asthma is under control • Show how to mark gauge with child’s zones (personal best, caution, danger) • Help parent establish a routine for peak flow measurements each morning • Remind the parent to adjust medications if peak flow reading is <80% of normal/personal best. Asthma Basics for Children, Mailman School of Public Health, Columbia University What about Triggers? • Provider Message: • Some children’s asthma is “triggered” by allergies, irritants, or exercise • If there are triggers, steps can be done to reduce the child’s exposure to them • Parent Message: • Asthma management is not just medicines. Need to control triggers. • Many triggers are very common in our homes, and having a “trigger” like dust in the home doesn’t mean parent is bad housekeeper. • Can do something about some but not all triggers. Communication Tips about Triggers • Ask parents about what triggers asthma • Give a “trigger checklist” parents can use to identify possible triggers in their home • Recommend skin testing to determine specific allergens (dust, cockroach, pet dander, mold…), and follow with de-sensitization as needed • Make recommendations for steps parents can take to control triggers – Use of quick-relief medicines before exposure or exercise – Cleaning/control tips – Smoking cessation if there is a smoker in home – Who to contact for help with triggers Reaching out for Support: Early Childhood Centers and Schools • Goal: Reduce asthma-related absences to only if very bad or fever/sore throat • Steps towards a partnership with schools: – Inform center/school about child’s asthma – Center/school should have a plan for what to do if child has asthma episode – Agreements/plans for medications as needed at school – Trigger identification and removal Asthma Basics for Children, Mailman School of Public Health, Columbia University An Example: The ABC Asthma Solutions Program with Early Childhood Educators • Complementary “Asthma Solutions Handbooks” for early childhood educators and parents • 3 part training series for early childhood educators • Asthma screening program through the early childhood centers • 2 part training program for parents • Follow-up by the center’s staff • Integration of asthma units and improved management into the child care program • It Takes a Village approach to environmental triggers The Experience of 14 Centers: One in Five had Asthma Status of Children Screened (N=479) 20% 39% Children with asthma symptoms but no diagnosis Children with symptoms and diagnosis 41% Children with no symptoms, no diagnosis Asthma Basics for Children, Mailman School of Public Health, Columbia University Need for Enhanced Screening of Preschoolers • Clear need for early screening programs: 20% of the children in the day care centers already had a diagnosis, and another 39% had asthma symptoms. • Screen children whose parents have/had asthma: Children with asthma symptoms were over 2 times more likely to have a parent with asthma. • State-of-the-art now includes recommendations on diagnosis and management of asthma among pre-schoolers. • Source: Special Supplement on Asthma among Preschoolers, Pediatrics, Oct. 2001. Diagnosed Children with Asthma Action Plans Asthma Diagnosis and Action Plans (N=96) Children with asthma diagnosis with an action plan 43% 57% Children with asthma diagnosis with no action plan Asthma Basics for Children, Mailman School of Public Health, Columbia University The Need to Improve Asthma Management • One-fourth (26%) of symptomatic children had been to the ER for asthma in the past year • Only 13% of diagnosed symptomatic diagnosed children had been to a doctor about asthma in the past year. • One-third (37%) of the symptomatic, undiagnosed children had seen a doctor but not been diagnosed. • Asthma symptoms are keeping children from school, at a cost to themselves and their parents, with 2-3 times more absences than among non-symptomatic children. • Most (57%) parents of diagnosed children do not have an asthma action plan. Asthma Basics for Children, Mailman School of Public Health, Columbia University Need for Better Links to Providers • Providers need to be proactive about diagnosing asthma, even among young children • Early Childhood Centers and parents seek providers who will be partners in asthma management • Proactive providers can help ensure regular asthma check-ups, appropriate medications guided by an asthma action plan, and reduced school absences. Asthma Basics for Children, Mailman School of Public Health, Columbia University