Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
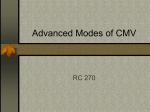
HOME NON INVASIVE POSITIVE PRESSURE VENTILATION BY AHMAD YOUNES PROFESSOR OF THORACIC MEDICINE Mansoura Faculty of Medicine Non-invasive ventilation • Non invasive ventilation refers to techniques that provide alveolar ventilation without an invasive artificial airway in place i.e. endotracheal or tracheostomy tube is not needed. • This can be accomplished by either negative or positive pressure. Home Ventilation • Non Invasive Ventilaion A) Negative pressure ventilation B) Positive pressure ventilation (Pressure preset ventilation or volume preset ventilation or dual modes). • Invasive Ventilaion (Pressure preset ventilation or volume preset ventilation or dual modes).. Modes of Ventilation • Almost any ventilator mode that can be applied with an endotracheal tube in place can be administered noninvasively. • Pressure cycled ventilators have been applied utilizing : - BIPAP. - CPAP. • Volume cycled ventilators have been used successfully utilizing: - control. - Assist-control. Non-invasive ventilation • In the vast majority of cases therapy will be delivered with positive pressure devices, although a few individuals still use negative pressure devices . • Negative pressure devices present a number of difficulties with regard to home ventilation including bulkiness, fit and comfort , they can induce significant upper airway obstruction , rendering therapy ineffective . External Negative Pressure Ventilation • ENPV is provided by a variety of devices applied externally to the chest wall and abdomen. • These devices generate intermittent subatmospheric pressure and thus inspiratory airflow. • Exhalation is usually passive, resulting from the inward elastic recoil of the lung and chest wall. Devices of External Negative Pressure Ventilation • Tank ventilator “iron lung”: the most effective one. • Cuirass. • Jacket ventilator. • Hayek oscillator: the most recent variation of cuirass negative pressure ventilator Iron-lung Cuirrass Non-invasive ventilation • Prior to the introduction of NIV in the mid 1980’s, home ventilation was restricted to a) negative pressure devices used primarily in patients with poliomyelitis, and b) tracheostomy ventilation used for patients with severe respiratory muscle weakness or total paralysis. • Both forms of ventilatory support were associated with significant practical difficulties, which meant that home ventilation was restricted to a small number of individuals usually with complex chronic health care needs. Non Invasive Positive Pressure Ventilation • The simplicity, cost and acceptability of NIV has led to this approach being widely adopted by the respiratory community and accepted by patients to the extent that NIPPV is now considered first line therapy in the management of chronic respiratory failure. • Importantly, it is now recognized clinically that ventilatory support during sleep is all that is required to achieve sustained daytime improvements for most patients. Non Invasive Positive Pressure Ventilation • European survey of home ventilation identified almost 22,000 users in 16 countries, 87% of whom used non-invasive ventilation . • NIPPV is acceptable to patients on a long-term basis and can alleviate symptoms related to chronic hypoventilation , improving survival and quality of life. Non Invasive Positive Pressure Ventilation • Volume preset ventilation delivers a stable tidal volume irrespective of the patient’s pulmonary system mechanics (compliance, resistance and active inspiration) . In contrast, pressure preset ventilation delivers a set pressure during inspiration and expiration, and changes in the patient’s pulmonary mechanics directly influence the flow and the delivered tidal volume . • Most studies evaluating these two modes in patients with chronic respiratory failure have shown equivalent effects with respect to maintaining nocturnal gas exchange and improving daytime blood gases . Non Invasive Positive Pressure Ventilation • Due to lower cost and greater patient comfort , most patients in the majority of centres are now prescribed pressure preset devices, mostly commonly, bilevel machines. • volume ventilators are recommended for patients with the most severe respiratory failure including those with tracheostomy and when continuous or near continuous ventilator support is needed. • A switch from pressure to volume preset ventilation may also be required in patients who are adherent to pressure preset ventilation but who fail to respond to treatment . • No difference in blood gas improvement, lung function or compliance with therapy was seen between the two modes. Non Invasive Positive Pressure Ventilation • Volume preset ventilators are usually set in an assist / control or control mode of support. • Pressure preset devices may be set in an assist (“spontaneous”) mode where each breath is patient triggered; an assist / control (“spontaneous/ timed”) mode where breaths may be patient or machine triggered; and a control (“timed”) mode where all breaths are machine triggered only . • The pressure settings used in bilevel devices include the inspiratory positive airway pressure (IPAP) and expiratory positive airway pressure (EPAP), with the difference between the two determining the level of pressure support . Non Invasive Positive Pressure Ventilation • A recent innovation in this area is that of autotitrating bilevel devices. • The algorithms of these machines are designed to automatically titrate pressure support levels, and in some devices EPAP, based on minute ventilation or flow targets. • There is mounting evidence for the use of these devices in managing sleep disordered breathing in patients with central sleep apnoea/Cheyne– Stokes respiration . Goals of non-invasive ventilation • For those with stable or slowly progressive disorders, the purpose of providing ongoing therapy is to increase survival while maintaining or improving the quality of life . • In rapidly progressive disorders, the primary goal is to palliate symptoms . • In a small group of individuals, such as those with cystic fibrosis, home NIPPV may provide a temporizing measure until transplantation is possible . • The non-invasive approach also permits earlier intervention in the course of the disease than is possible with invasive techniques , reduces acute care costs by decreasing hospital length of stay and readmissions , and simplifies the burden of care related to managing chronic respiratory failure in the home . Types of Home Ventilation • Nocturnal Ventilatory Support ( sleep disordered breathing) Usually Pressure preset ventilators . • Nearly Continuous (>18 hours) Ventilatory Support (Nocturnal Ventilatory support + most daytime ventilatory support ) Usually Volume Preset Ventilators . • Continuous ventilatory support (Ventilator dependent individuals ) Life Support Ventilators ( BACK UP RATE , POWER FAILURE ALARMS ,MASK OFF ALARMS , LOW PREASSURE ALARMS ) Patient Selection • Criteria for selecting patients for NIPPV: 1. Alert & cooperative. 2. Hemodynamic stability. 3. No need for endotracheal intubation: to protect airways or to remove excessive secretions. 4. No acute facial trauma. 5. Properly fitted mask. 6. No multiorgan dysfunction. Exclusion criteria: 1. Respiratory arrest. 2. Cardiovascular instability (hypo tension, arrhythmias, myocardial infarction). 3. Somnolence impaired mental status, uncooperative patient. 4. High aspiration risk; Viscous or copious secretions. 5. Recent facial or gastro-esophageal surgery. 6. Crainio-facial trauma, fixed naso-pharyngeal abnormalities. 7. Burns. 8. Extreme obesity (>200% of ideal body wt). Advantages of NIPPV • Better tolerance. • No need for sedation. • Patient can talk, eat, … Drawbacks of NIPPV • Air leaks. • Facial skin necrosis • Gastric distension • Eye irritation. • Claustrophobia. Treatment modalities for Positive Airway Pressure Therapy • Continuous positive airway pressure Provides a constant pressure throughout the respiratory cycle • Bi-level positive airway pressure Provides two pressure levels during the respiratory cycle: a higher level during inspiration and a lower pressure during expiration • Autotitrating positive airway pressure Provides variable pressures using device-specific diagnostic and therapeutic algorithms • Nocturnal noninvasive positive pressure ventilation Provides two pressure levels at a set rate to assist ventilation Determining Optimal Continuous Positive Airway Pressure 1. In-laboratory attended polysomnographically guided CPAP titration – Full-night studies. – Split-night studies (consists of an initial diagnostic portion and a subsequent CPAP titration on the same night) 2. Unattended laboratory or home titration 3. Use of autotitrating devices 4. Formula-derived pressures from clinical, PSG, and/or anthropometric variables The current standard of practice • The current standard of practice involves an attended pressure titration during a laboratory PSG, during which sleep stages and respiratory variables are monitored. • The goal is to determine a single fixed pressure that eliminates apneas, hypopneas, snoring, and respiratory effort–related arousals (RERAs); maintains adequate oxygen saturation; and improves sleep architecture and quality in all sleep positions and in all sleep stages. • It is generally accepted that higher pressures are required to reverse airway occlusion during REM sleep and during sleep in a supine position. • Split-night studies can potentially underestimate the severity of OSA Criteria for split-night (CPAP) titration • At least 2 hours of recorded sleep time during the initial diagnostic portion of the study • Apnea-hypopnea indices during the diagnostic portion of the study: AHI 40 OR • AHI 20–40 (accompanied by significant oxygen desaturation) • At least 3 hours are available for CPAP titration with the presence of REM sleep during a supine sleep position AASM recommendations for CPAP and BPAP therapy for adult patients with sleep related breathing disorders • The presence of OSA based on an acceptable diagnostic method should be established prior to CPAP therapy (standard). Indications for CPAP therapy include: a. Moderate to severe OSA (standard) b. Mild OSA (option) c. Improvement of subjective sleepiness in patients with OSA (standard) d. Improvement of quality of life in patients with OSA (option) e. As an adjunctive therapy to lower blood pressure in patients with OSA (option) AASM recommendations for CPAP and BPAP therapy for adult patients with sleep related breathing disorders 3. The preferred CPAP titration method to determine optimal positive airway pressure is an in-laboratory, fullnight, attended polysomnography, but split-night studies are usually adequate (guideline). 4. Objective monitoring of CPAP use is recommended to ensure optimal utilization (standard). 5. Close monitoring of CPAP utilization and any problems that might develop, especially during the first few weeks of use, is important, as is the correction of problems if needed (standard). 6. Addition of heated humidification and a systematic educational program enhance adherence to CPAP use (standard). AASM recommendations for CPAP and BPAP therapy for adult patients with sleep related breathing disorders 7. Patients with OSA treated with CPAP therapy should be followed up yearly or more frequently as needed to correct problems related to its use (option). 8. CPAP and bilevel positive airway pressure (BPAP) therapy are generally safe with minor adverse effects (standard). 9. BPAP can be considered as an optional therapy to CPAP in selected patients who require high pressures, who report difficulty exhaling against a fixed CPAP pressure, or who have coexisting central hypoventilation (guideline). 10. BPAP may also be beneficial in patients with some forms of restrictive lung disease or hypoventilation syndromes with daytime hypercapnia (option). AASM recommendations for CPAP and BPAP therapy for adult patients with sleep related breathing disorders • The extent to which asymptomatic patients with mild OSA and no associated medical or psychiatric disorders benefit from CPAP is less certain. • Intermittent use of CPAP should be avoided, because virtually all of the gains in sleep quality and daytime alertness derived from sleeping with CPAP are rapidly reversed with CPAP discontinuation. Starting PAP treatment based on a prediction equation with subsequent adjustment based on symptoms, machine readings, and nocturnal oximetry. • Predicted CPAP =0.16XBMI +0.13 X NC + 0.04 XAHI – 5.12 where BMI = body mass index and NC = neck circumference in centimeters AHI =apnea hypopnea index. Auto-adjusting (auto-titrating) CPAP, devices Auto-CPAP devices provide a useful alternative for providing positive airway pressure (PAP) treatment for patients with OSA . • One can separate the uses of these devices into two large categories These include: (1) Auto-titration PAP to determine an effective fixed level of CPAP) 2- Auto-adjusting CPAP for chronic treatment with the advantage of delivering the lowest effective pressure in any circumstance. Chronic treatment with APAP would also eliminate the requirement for a CPAP titration Auto-CPAP devices • When used in the auto-titration mode, the devices are used by the patient for a period of time (one night to several weeks). Information stored in the device is transferred to a computer and can be used to select an optimal fixed level of CPAP for chronic treatment. • When APAP devices are used for chronic treatment they have the potential advantage of delivering the lowest effective pressure in any circumstance (body position, sleep stage). The mean pressure for the night may be lower than a single pressure that would be effective in all circumstances (the prescription pressure). For example, higher CPAP is usually needed in the supine posture and during rapid eye movement (REM) sleep. Auto-titrating CPAP mode • Attended auto-titration in CPAP naïve patient (technologist extender) • Unattended auto-titration in CPAP naïve patient • Check prescription pressure after weight gain/loss • Salvage a failed manual CPAP titration Auto-adjusting mode • Initial chronic treatment of OSA (no titration needed) • Chronic treatment in patients not tolerating CPAP • Chronic treatment in patients with difficult mask/mouth leak BiPAP Pro Bi-Flex • The BiPAP Pro Bi-Flex device delivers the following therapies: • Bi-level – Provides EPAP and IPAP. • Bi-level with Bi-Flex – Bi-level therapy with pressure relief upon exhalation to improve patient comfort based on patient needs. • CPAP. • CPAP with C-Flex – Delivers CPAP therapy with pressure relief upon exhalation to improve patient comfort based on patient needs. Pressure curve when BiPAP = 10/5 cm H2O; The pressure is higher on inspiration than on expiration, but both pressures are above ambient .In this example IPAP is set as 10 cm H2O and EPAP is set as 5 cm H2O. BiPAP S/T SPECIFICATIONS: • Modes : CPAP, S, ST • Timed inspiration 0.5 to 3.0 seconds • IPAP 4 to 25 cm H2O • EPAP 4 to 25 cm H2O • CPAP 4 to 20 cm H2O • Breath rate 0 to 30 BPM • Weight 1.36 kg Dimensions 18 cm x 14 cm x 10 cm • Alarms Patient Disconnect, Apnea, Low Minute Ventilation BiPAP Auto Autobilevel positive airway pressure with a minimum EPAP of 6 cm H2O and a maximum IPAP of 25 cm H2O. Automatic Positive Airway Pressure • In the older generation of APAP devices, the sensors were simplistic and measured only the pressure inflections (vibrations) of a certain frequency and amplitude that were caused by snoring. • The next generation of APAP devices became more sophisticated and were able to sense flowbased changes such as apnea, hypopnea, or inspiratory flow limitation based upon the inspiratory flow contour (i.e., flattening of the inspiratory flow waveform). Advanced methods of Autotitration • Newer generation devices can can increase the IPAP alone in order to ameliorate obstructive events (Auto Bilevel PAP),correct hypoventilation (averaged volume assured pressure support [AVAPS], Intelligent Volume Assured Pressure Support (iVAPS ) or combat central apneas in patients with complex sleep apnea (ServoVentilation). • Devices may also introduce a back-up rate to prevent central apneas and although in general they are not referred to as APAP devices, they function using similar principles and can be judged as the latest generation of APAP devices . BiPAP AVAPS • Clinicians no longer need to choose between pressure or volume ventilation in order to deliver optimum therapy to NIV patients. • Now, they can have both. The BiPAP AVAPS (Average Volume Assured Pressure Support) home ventilator enables clinicians to achieve the prescribed target volume pressure without compromising patient comfort. • Automatically adapts to patient’s changing needs • Designed for clinical ease of use and patient comfort • Powered by advanced technologies SPECIFICATIONS: • • • • • • • • • • • • • Modes CPAP, S, ST, PC, T AVAPS available on S, ST, PC, and T modes Bi-Flex Available from S mode Target Tidal Volume from 200 to 1500 ml IPAPmin From EPAP to IPAPmax IPAPmax From IPAPmin to 25 cm H2O Timed inspiration 0.5 to 3.0 seconds IPAP 4 to 25 cm H2O EPAP 4 to 25 cm H2O CPAP 4 to 20 cm H2O Breath rate 0 to 30 BPM Weight 1.36 kg Dimensions 18 cm x 14 cm x 10 cm Alarms Patient Disconnect, Apnea, Low Minute Ventilation, Low Tidal Volume (AVAPS modes only) BiPAP AVAPS Ideal body weight • Estimated ideal body weight in (kg) Males: IBW = 50 + 2.3 for each inch over 5 feet. Females: IBW = 45.5 + 2.3 for each inch over 5 feet. • Estimated adjusted body weight (kg) If the actual body weight is greater than 30% of the calculated IBW, calculate the adjusted body weight (ABW): ABW = IBW + 0.4(actual weight - IBW) • The IBW and ABW are used to calculate medication dosages when the patient is obese. • This formula only applies to persons 60 inches (152 cm) or taller. BiPAP AVAPS and VPAP™ ST with iVAPS Anatomical Dead space • Inspired/expired air remaining in conducting airways • Not involved in gas exchange • Correlation between patient’s height and dead space (Vd) • Height is used to calculate anatomical dead space (Vd) for each breath of air (Tidal Volume) • Example dead space volume (Vd) : 120 ml for height 175 cm or 70 inches Anatomical dead space in relation to height of the patient As alveolar ventilation drops , iVAPS rapidly increase pressure support until target Va is reached, and as alveolar ventilation increase , iVAPS rapidly decrease pressure support . Intelligent back up rate (iBR) stays out of the way at 2/3 spontaneous rate whenever the patient spontaneously triggers above 2/3 of the target . once the patient rate reach minimum back up rate (2/3 of the target ) iBR increase towards patient spontaneous rate to maintain alveolar ventilation .Once spontaneous trigering returns, iBR drops back to 2/3 of the target / spontaneous rate. Auto-TriLevel • The auto-TriLevel principle by Weinmann combines two proven types of therapy – auto-CPAP and BiLevel – into a synthesis that offers the most therapy effectiveness. Your benefits with these products: • Therapeutically effective maximum and mean pressures that are lower than BiLevel with the same tidal volume for fewer side effects such as leakage. • It‘s like a new titration every day – adjusts to patient‘s high variability . • Effortless titration and monitoring . Auto-TriLevel • IPAP: inspiratory pneumatic splinting of the airways (ventilation) • EPAP: easier exhalation at a low expiratory pressure level for a pleasant breathing sensation • Additional end-expiratory pressure (EEPAP): required minimum pressure for adequate splinting of airways during phase when risk of collapse is highest • PDIFF (Δ IPAP-EPAP): needoriented ventilation support by means of changes between inspiratory (IPAP) and expiratory (EPAP) pressure levels Auto-TriLevel • Reduced mean and maximum therapy pressure under TriLevel: Results of a bench test comparison with BiLevel therapy. • SOMNOvent auto-ST is the world‘s first automatic BiLevel device that permits goal-oriented therapy settings(SCOPES). • With the combination of the autoTriLevel principle and the automatic trigger WMtrak, this device delivers the greatest effectiveness, reliability and breathing comfort – simply the fastest therapy results. • Particularly for cases of complicated SDB, SOMNOvent auto-S, convinces with its intelligent combination of automatic BiLevel S therapy and auto-CPAP. Auto-TriLevel • Auto-bilevel spontaneous (SOMNOvent auto-S ). • Auto-bilevel spontaneous/timed (SOMNOvent auto-ST ). • Anti-cyclic modulated ventilation (SOMNOvent auto-CR ). ASV is a variant of BPAP that was developed to treat Cheyne-Stokes central apnea. Both ASV and BPAP devices with a backup rate are approved for use with patients with central apnea and complex sleep apnea SomnoVent CR Respironics autoSV ResMed VPAP Adapt SV Advanced methods of titration • Servo-ventilation made by different manufacturers can successfully detect and treat central apneas . • During servo-ventilation, the expiratory positive airway pressure is set at a level to treat obstructive apneas and obstructive hypopneas. • Combining APAP and servo-ventilation, with APAP determining the EPAP level automatically, whereas the servo-ventilation controlling periodic breathing and central apneas has been recently reported to be effective in ameliorating SRBD . BiPAP A30 Ventilator • For 24 Hours Use • BiPAP A30 ventilator has been designed to combine ease of use with technology advancement to deliver enhanced therapy that adapts to patient’s condition. • Being at home can work wonders so It delivers a smooth transition from hospital to home for chronic respiratory patients. • Compatible with PSG Systems • Optional Oximetry Module • Intuitive, User Friendly & Colored Interface • Integrated Heated Humidifier • Graphical & Statistical Data Management on Encore Pro & Direct View Soft wares SPECIFICATIONS: • • • • • • • • • • Modes CPAP, S, ST, PC, T , AVAPS AVAPS available on S, ST, PC, and T modes AVAPS Rate 0.5 to 5 cmH2O/min Target Tidal Volume from 200 to 1500 ml IPAP 4 – 30 cmH2O EPAP 4 – 25 cmH2O Breath Rate 0 – 40 BPM Inspiratory Time 0.5 – 3 sec Rise Time 1 (100 ms) – 6 (600 ms) Monitoring Pressure, Tidal Volume, Minute Ventilation, Respiratory Rate, I/E Ratio • Weight 2.1 kg (with Power Supply) Noise Level < 30 dBA at 10 cmH2O • Humidification System one Humidification & Dry Box technology • Alarms Patient Disconnect, Apnea, Low Minute Ventilation, Low Tidal Volume, High Respiratory Rate BiPAP A40 Ventilator • BiPAP A40 comes with well-known and clinically proven Philips Respironics technology such as Auto-Trak, AVAPS and a Dry Box humidifier design. • The device is capable of non invasive and invasive pressure ventilation, up to 40 cmH2O, providing treatment for your chronic respiratory insufficiency patients. • The device features AVAPS-AE, the first fully automatic ventilation mode, designed to help clinicians during titration process, while maintaining comfort and therapy optimization at the lowest pressures. BiPAP A40 Ventilator • This new innovative ventilation mode helps in providing long term therapy compliance regardless of changes to the body position, sleep stages and respiratory mechanics. • Detachable Battery with up to 5 Hours Backup • AVAPS-AE Automatically Adjust Ventilation to the Patients Need • Compatible with PSG Systems • Optional Oximetry Module • Intuitive, User Friendly & Colored Interface • Integrated Heated Humidifier • Graphical & Statistical Data Management on Encore Pro & Direct View Soft wares SPECIFICATIONS • Ventilation modes : CPAP, S, S/T, PC, T, AVAPS-AE • Hybrid ventilation AVAPS (Average Volume Assured Pressure Support) AVAPS-AE • IPAP 4 – 40 cm H2O • EPAP 4 – 25 cm H2O • Target tidal volume (when AVAPS enabled) 200 – 1500 ml • Breath rate 0 – 40 bpm (4 – 40 bpm in T mode) • Inspiratory time 0.5 – 3 sec. • Triggering and cycling Auto-Trak ,Sensitive Auto-Trak, Flow triggering. • Rise time 1 (100 ms) – 6 (600 ms) • Size 21.6 cm W x 19 cm L x 11.5 cm H • Weight 2.1 Kgs (with power supply) SPECIFICATIONS: • Humidification System One humidity control and ‘Dry Box’ technology • Alarms Patient disconnection Apnea ,Low minute ventilation ,Low tidal volume (with AVAPS/AVAPS-AE only) ,High RR • Monitoring Pressure, tidal volume, minute ventilation, respiratory rate, leak, I/E ratio • Battery back up Detachable battery module: 5 hours • DC power source 12 VDC, 5.0 A (external battery), 24 VDC, 4.2 A (power supply) • Data management Encore Pro 2 and Direct View software • Compatible with oximetry module • Advanced detection of residual respiratory events(Obstructed Airway Apnea, Clear Airway Apnea, Hypopnea, Periodic Breathing, RERA, Large Leak and Snore) Finger tip pulse oximeter with adapter Detachable Battery ,Detachable Battery Module and roll stand Carrying Case. The bag is designed to attach the ventilator to a wheelchair VENTImotion 2 Oxygen supply with VENTI-O2 / VENTI-O2 plus • For safety reasons (risk of fire), it is not permitted to supply oxygen directly to the tube system or to the breathing mask without a special safety device. • On this device, the supply of oxygen is permitted only using the VENTI-O2 and VENTIO2 plus oxygen supply valves. • It is possible to supply up to 4 l/min or 15 l/min of oxygen using VENTI-O2 or VENTI-O2 plus. In the event of a fault, the VENTI-O2 gives the oxygen off into the atmosphere, thus preventing it from accumulating in the device. VENTIpower • You can use VENTIpower to operate the device independently of the electricity supply. • You can connect VENTIpower to the device in parallel to the regular electricity supply (top socket). • If the regular electricity supply fails, VENTIpower undertakes the supply of power to the device after a delay of approx. 4 seconds. • VENTIpower must be switched on for this. VENTIlogic LS Intended use • VENTIlogic LS is used for invasive and noninvasive life-support ventilation. • The device can be used in both static or mobile operation, both at home and in appropriate hospital departments. Note :VENTIlogic LS is not a ventilator for intensive care purposes. The device can be used for weaning off invasive ventilation and converting to mask ventilation. It is used on patients with medium to severe acute and chronic global respiratory insufficiency with a tidal volume of at least 50 ml and a body weight of at least 5 kg. Intended use • VENTIlogic plus is used for invasive and noninvasive life-support ventilation. The device can be used in both static or mobile operation, both at home and in appropriate hospital departments. Note :VENTIlogic plus is not a ventilator for intensive care purposes . The device can be used for weaning off invasive ventilation and converting to mask ventilation. It is used on patients with medium to severe acute and chronic global respiratory insufficiency with a tidal volume of at least 50 ml and a body weight of at least 5 kg. Intended use • Obstructive respiratory disorders, such as COPD • • Restrictive respiratory disorders such as scolioses, deformities of the thorax , • Neurological, muscular and neuromuscular disorders, such as muscular dystrophies, pareses of the diaphragm etc. • Central respiratory regulation disorders • Hypoventilation syndrome associated with obesity Pathologic defaults offer a choice of disease-specific preset setting values to facilitate a quick and sensible starting point to therapy. Stellar 150 • The Stellar 150 is intended to provide ventilation for non-dependent, spontaneously breathing adult and pediatric patients (30 lb/13 kg and above) with respiratory insufficiency, or respiratory failure, with or without obstructive sleep apnea. • The device is for noninvasive use, or invasive use (with the use of the ResMed Leak Valve). • Operation of the device includes both stationary , such as in hospital or home, or mobile, such as wheelchair usage. Stellar provides the following modes • CPAP mode—a fixed pressure is delivered. • S (Spontaneous) mode—the device senses the patient breath and triggers IPAP in response to an increase in flow, and cycles into EPAP at the end of inspiration. The breath rate and the respiratory pattern will be determined by the patient. • ST (Spontaneous/Timed) or PS (Pressure Support) mode—the device augments any breath initiated by the patient, but will also supply additional breaths should the patient breath rate fall below the clinician's set ’backup’ breath rate. • T (Timed) mode—the fixed breath rate and the fixed inspiration time set by the clinician are supplied regardless of patient effort. Stellar provides the following modes • PAC (Pressure Assist Control)—the inspiration time is preset in the PAC mode. There is no spontaneous/flow cycling. The inspiration can be triggered by the patient when respiratory rate is above a preset value, or time triggered breaths will be delivered at the backup breath rate. • iVAPS (intelligent Volume Assured Pressure Support)— designed to maintain a preset target alveolar ventilation by monitoring delivered ventilation, adjusting the pressure support and providing an intelligent backup breath automatically. The iVAPS therapy mode is indicated for patients 66 lb (30 kg) and above. Pathology Defaults • The Pathology Defaults offer a choice of disease-specific preset setting values to facilitate efficient commencement of therapy. • You can select from four sets of respiratory system mechanics. • Before use you will need to review the set parameters on the Clinical Settings screen.