Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
African trypanosomiasis wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Marburg virus disease wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Gastroenteritis wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Schistosomiasis wikipedia , lookup
Anaerobic infection wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Sarcocystis wikipedia , lookup
Neonatal infection wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
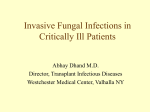
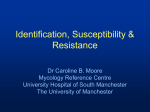
Can Probiotics Reduce Candida Infections? Peter Cartwright MSc MA Human Microbiota Specialist, Probiotics International Ltd. Candida in the Microflora At least one-third of healthy individuals carry the Candida fungus; in the mouth, the intestine or the vagina1,2,3,4. This prevalence, without symptoms, means that Candida can be considered a member of the normal microflora of human beings5. The microflora are communities of microscopic organisms that live with us for the whole of our lives, and are beneficial to our health. Under certain circumstances, however, Candida fungus can cause infectious disease, which occasionally can take a very serious form. How can a microorganism be a member of our microflora and also cause disease? Why is Candida such a Troublesome Opportunistic Pathogen? As a fungus, Candida is unlike the vast majority of microbes in the human flora, which are bacteria. A bacterium is a prokaryote (containing no nucleus or other organelles), while a fungus is a eukaryote, which is a more complex type of cell, closer in evolutionary terms to a human cell. Such greater complexity makes Candida a troublesome microbe when it switches into pathogenic mode. Candida albicans is the species responsible for the majority of infections, but other species such as Candida glabrata, Candida parapsilosis and Candida tropicalis are also pathogenic in humans8. The answer to this question is not yet known for certain, but it could be that Candida provides benefits to the host and is therefore accepted. Alternatively, Candida could be a pathogen that is very tricky to eradicate, but is controlled by the normal microflora. As no benefits from Candida have yet been identified, the second explanation seems more likely. In most people, the risk from Candida is low, because the fungus constitutes a very small proportion of the overall microfloral population. Several studies have found that only about 3-4,000 Candida cells are present in 1 gram of content of the large intestine. This is a tiny number compared with the billions of bacteria found in the same amount of colonic content2,3,4,6. Despite the relatively low risk from Candida in the microflora, and the development of new anti-fungal drugs, the incidence of Candida infections continues to rise, especially among hospital patients7. For example, over a 13-year period (19801992) there was a 5-fold increase in bloodstream infections caused by Candida in US hospitals. To understand why this is happening, it is necessary to look at Candida fungus in greater detail. Protexin Health Care Graphics by Doig Simmonds after C.C.Odds 1988 Candida in its yeast form is considered a normal gut inhabitant when present in low numbers. One of the reasons why C. albicans is such a persistent pathogen is that it can take two forms. Most of the time it exists as a single-celled yeast, but sometimes it converts to a mycelium (a network of fine filaments). The yeast-form can flow more easily in fluid and the mycelium-form can move more easily between the cells of human tissues by the insertion of growing tubes (hyphae). There is also a third and The Clinical Use of Probiotics PAGE 21 intermediate form, known as pseudohyphae, which are strings of elongated yeast cells, and these structures also appear to have invasive ability9. These different forms of the fungus may all coexist together. The ability to change form, which can occur quickly10, makes it easier for C. albicans to resist the body’s various defence mechanisms. appropriate microbial stimulation at an early age. The latest version of the hygiene hypothesis proposes that the gut microflora is missing certain microbes, such as helminthic worms, that are important in an evolutionary context to the proper development of our immune systems. If infants do not have their gut lymphoid tissues suitably provoked by the gut flora, their immune system may not function efficiently in later life. Given these potential factors behind Candida infection, it is no surprise that a number of experts have concluded that the most important aspect of avoiding Candida infection is having a balanced microbial flora and a healthy immune system2,13. This has led people to consider the use of probiotics, because these beneficial microbes are good at restoring disturbed microflora and improving immune function. Graphics by Doig Simmonds after C.C.Odds 1988 The multicelluar form of Candida albicans can make it easier to resist the body’s defence mechanisms. Candida infection (candidiasis) causes two main types of disease: superficial and systemic. Superficial infection, known as ‘thrush’, may occur in the mouth or vagina, with the production of a white itchy surface layer, and also discharge from the vagina5. Superficial candidiasis may also occur on the skin, especially at moist folds and creases. Systemic candidiasis involves the passage of Candida cells into the bloodstream, where they may form colonies in almost any part of the body. Such entry through the skin or mucosal surfaces usually only occurs if there is damage to these surfaces. Systemic candidiasis can be life-threatening and is especially difficult to treat. The increase in incidence of candidiasis infections is probably due, in part, to the greater use of broad-spectrum antibiotics that disturb the microflora. In vitro studies have shown that colonic microflora reduces Candida spp. numbers11, and in vivo studies have shown that the use of broad-spectrum antibiotics increases the risk of candidal infection4,6,12. Antibiotics kill or inhibit bacteria, but leave fungi unaffected. With the bacteria of the gut microflora disturbed, there is opportunity for Candida numbers to increase substantially. Another factor in the increased incidence of Candida infection, is the greater use of corticosteroids and other immunosuppressive agents that alter the functioning of the immune system13. The relevance of a weakened immune system is reflected in the fact that leukaemia patients carry higher levels of Candida spp.14 and patients with HIV virus are much more likely to develop candidiasis. The increase in Candida infections may also be due to the ‘hygiene’ effect. The hygiene hypothesis blames the increase in diseases of the malfunctioning immune system (e.g. asthma, eczema, autoimmune diseases) on the absence of Protexin Health Care Evidence of Probiotic Benefits There have been a number of clinical studies examining the effects of probiotics on vaginal candidiasis. A group of women with recurrent vaginal candidiasis consumed yoghurt containing Lactobacillus acidophilus for six months, and there was a three-fold lower level of infections compared to the control group15. In a more recent randomised controlled trial (RCT), an oral probiotic consisting of two Lactobacillus species (a Lactobacillus rhamnosus and a Lactobacillus reuteri) significantly improved the effectiveness of an anti-fungal drug. Vaginal discharge was reduced, as were Candida cell numbers16. There have also been two studies in which the probiotics were administered vaginally. One used a L. rhamnosus and the other used a L. acidophilus. Both showed benefit, including a halving of the risk of developing candidiasis in the latter study17. A RCT has also been undertaken with 80 premature infants, with a view to preventing candidiasis. Candida can be a major threat to the lives of such infants with their underdeveloped immune systems. The group of infants receiving L. rhamnosus for six weeks were significantly less likely to have their intestine colonised by Candida (23% compared with 49% in the control group)18. Different Species A number of different probiotic species were used in the above studies, so how important is the type of species used in a probiotic product? By definition, species of bacteria have different characteristics. In fact, even within a species, some strains behave slightly differently. Therefore it can be expected that some probiotic bacteria will be more effective against Candida than others. The Clinical Use of Probiotics PAGE 22 Furthermore, the mechanisms of benefit from probiotic bacteria are wide-ranging. This should not be surprising, because we are dealing with a living organism (the bacterium) interacting with cells of another organism (human being). Their complicated metabolisms and surface structures are bound to offer a range of potential influences. The importance of species used was demonstrated in one study of mice using four different probiotic species. Two of the species (Bifidobacterium animalis and L. acidophilus) were superior to the other two (L. reuteri and Lactobacillus casei) in controlling Candida19. Conclusion Unfortunately, good quality studies on the use of probiotics against candidiasis are still relatively uncommon, and a clear picture of the most desirable characteristics of a probiotic species has not yet been obtained. Pending more research, it may be that a good quality, multi-species probiotic is currently the best choice. Candida infections can occur in men as well as women. References 1. Ruhnke M. 2002. Skin and Mucous Membrane Infections. In Candida and Candidiasis 12. Krause R, Schwab E, Bachhiesl D, et al. 2001. Role of Candida in Antibiotic-associated (Calderone, R.A., ed.) ASM Press, Washington, D.C., U.S.A.: 307-325. Diarrhea. The Journal of Infectious Diseases 184: 1065-1069. 2. Bernhardt H. & Knoke M. 1997. Mycological Aspects of Gastrointestinal Microflora. 13. Mitchell TG. 2004. Medical Mycology. In Jawetz, Melnick & Adelberg’s Medical Scandinavian Journal of Gastroenterology 32 Suppl 222: 102-106. Microbiology (Brooks GF, Butel JS & Morse SA, eds.). Lange Medical Books/McGraw-Hill, New 3. Ott SJ, Kuhbacher T, Musfeldt M, Rosenstiel P, Hellmig S, Rehman A, Drews O, Weichert W, York, U.S.A.: 623-659. Timmis KN, Schreiber S. 2008. Fungi and inflammatory bowel diseases: alterations of 14. Tomoda T, Nakano Y & Kageyama T. 1988. Intestinal Candida Overgrowth and Candida composition & diversity. Scandinavian Journal of Gastroenterology 43: 831-841. Infection in Patients with Leukemia: Effect of Bifidobacterium Administration. Bifidobacteria 4. Samonis G, Gikas A, Anaissie EJ, Vrenzos G, Maraki S, Tselentis Y, Bodey GP. 1993 and Microflora 7: 71-74. Prospective Evaluation of Effects of Broad-Spectrum Antibiotics on Gastrointestinal Yeast 15. Hilton E, Isenberg HD, Alperstein P, France K, Borenstein MT. 1992. Ingestion of Yogurt Colonisation of Humans. Antimicrobial Agents and Chemotherapy 37: 51-53. Containing Lactobacillus acidophilus as Prophylaxis for Candidal Vaginitis. Annals of Internal 5. MacCallum D. 2007. Candida albicans: New Insights in Infection, Disease and Treatment. Medicine 116: 353-357. In New Insights in Medical Mycology (Kavanagh, K., ed.). Springer, Dordrecht, The 16. Martinez R, Franceschini S, Patta M, Quintana SM, Candido RC, Ferreira JC, De Martinis Netherlands: 99-129. EC, Reid G. 2009. Improved treatment of vulvovaginal candidiasis with fluconazole plus 6. Mavromanolakis E, Maraki S, Cranidis A, Tselentis Y, Kontoyiannis DP, Samonis G. 2001. probiotic Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14. Letters in Applied The Impact of Norfloxacin, Ciprofloxacin and Ofloxacin on Human Gut Colonisation by Microbiology 48: 269-274. Candida albicans. Scandinavian Journal of Infectious Diseases 33: 477-478. 17. Falagas ME, Betsi GI & Athanasiou S. 2006. Probiotics for prevention of recurrent 7. Lewis RE & Klepser ME. 1999. The changing face of nosocomial candidemia: vulvovaginal candidiasis: a review. Journal of Antimocrobial Chemotherapy 58: 266-272. Epidemiology, resistance, & drug therapy. American Journal of Health-system Pharmacy 56: 18. Manzoni P, Mastert M, Leonessa ML, Priolo C, Farina D, Monetti C, Latino MA, Gomirato 525-533. G. 2006. Supplementation with Lactobacillus casei Subspecies rhamnosus Prevents Enteric 8. Pfaller MA & Diekema DJ. 2007. Epidemiology of invasive candidiasis: a persistent public Colonisation by Candida Species in Pre-term Neonates: A Randomised Study. Clinical health problem. Clinical Microbiology Reviews 20: 133-163. Infectious Diseases 42: 1735-1742. 9. Gow NAR, Brown AJP & Odds FC. 2002. Fungal morphogenesis and host invasion. Current 19. Wagner RD, Pierson C, Warner T, Dohnalek M, Farmer J, Roberts L, Hilty M, Balish E. Opinion in Microbiology 5: 366-371. 1997. Biotherapeutic Effects of Probiotic Bacteria on Candidiasis in Immunodeficient Mice. 10. Dignani MC, Solomkin JS & Anaissie EJ. 2003. Candida. In Clinical Mycology (Anaissie EJ, Infection and Immunity 65: 4165-4172. McGinnis MR & Pfaller MA, eds.). Churchill Livingstone, Philadelphia, U.S.A: 195-239. 11. Matthews HL & Witek-Janusek L. 2002. Host Defense against Oral, Esophageal, and Gastrointestinal Candidiasis. In Candida and Candidiasis (Calderone, R.A., ed.). ASM Press, Washington, D.C., U.S.A.: 179-192. Protexin Health Care The Clinical Use of Probiotics PAGE 23 About the author Peter Cartwright MSc MA Peter Cartwright has 17 years experience of working for patient and self-help associations, as Assistant Director of the National Association for Colitis and Crohn’s Disease, Director of the British Stammering Association and National Development Officer of the Self-Help Alliance. Currently he is a Trustee of the Bladder & Bowel Foundation. Peter has an MSc in Microbiology and an MA in Sociology. He is the author of three books for the general public on intestinal health, including Probiotics for Crohn’s and Colitis and has given over 40 lectures on probiotics to doctors in 10 countries. Probiotics International Ltd is one of the largest manufacturers and suppliers of probiotic supplements for the healthcare, veterinary and animal health industry. Products are marketed under the brand name of Protexin. As published in: 2010. The Clinical Use of Probiotics. Ed Barlow J. Probiotics International Ltd, United Kingdom. ©Probiotics International Ltd. Protexin Health Care The Clinical Use of Probiotics PAGE 24