Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
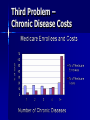
CMS Innovation Advisor Project Representing Group 4 Richard Young, MD Director of Research John Peter Smith Hospital FMRP Fort Worth, Texas [email protected] Group 4 – The Island of Misfit Toys My Project - Background People from the middle of the country, especially medium and small communities quickly understood my project. People from large cities, particularly the Washington DC to Boston corridor did not understand my project. Three Problems National shortage of primary care physicians Onerous primary care documentation, coding, and billing rules Patients with the most chronic diseases cost the most to care for Why Worry? – Primary Care Texas Ologist Supply - Quality Ologist Supply - Cost Family Physicians - Quality Family Physicians - Cost Another Model: WeCare • Example from a manufacturing facility in Indiana • 1,100 employees 2,300 lives • One-year savings: $4 million • Net clinic costs Summary – Better Quality and Lower Costs It’s an issue of physician supply But little interest in adult ambulatory primary care among U.S. medical students – 8% family medicine – 2% general internal medicine (if that) Why the Lack of Student Interest? Second Problem Onerous Evaluation and Management (E/M) documentation, coding, and billing rules. HCFA created these rules in 1995 then 1997 Reason? -- Fraud and Abuse No vetting, validating, piloting E/M Rules In 2002, an Advisory Committee on Regulatory Reform of the U.S. Health and Human Services Department reviewed these guidelines An advisor for HHS Secretary Tommy Thompson concluded, “documentation guidelines are the poster child for regulatory burden.” Voted 20-1 to eliminate the payment rules. CMS E/M Rules – Example From the Risk Table: The CMS Document 89 pages!! And There’s More Another 100 Pages Third Problem – Chronic Disease Costs My Project - Assumptions Interest in primary care among medical students will not increase until the income disparity is fixed. Existing CMS documentation, coding, and billing rules are the primary cause of the income disparity. My Project -- Assumptions Better U.S. primary care supply to take care of everyone, especially patients with multiple chronic diseases, leads to: – Better health – Better patient experience – Lower costs What is My Project? To throw away the existing CMS E/M documentation, coding, and billing guidelines and start all over. Driver Diagram Medical Students Ologies $ Adult Primary Care More Assumptions The solution is NOT to pay family physicians $200 for a sore throat. The solution is to pay family physicians for all the work they do that currently isn’t paid for. – Literature: 20%-50% of work NOT paid Align incentives to achieve better efficiencies and outcomes. My Previous Research Family physician cost-effectiveness – Article to be published in Family Medicine this spring. Family physician opinions of current system – Manuscripts in progress Project Development Formed advisory/feedback team – 23 family physicians Survey - Listed 28 units of work not currently explicitly paid under current system Vote for: – Paid as a separate fee – Paid as a global fee – Just part of our job More Supporting Work Surveyed doctors in other countries about their documentation, coding, and billing rules. – U.S. is the only country that ties documentation to payment Solution - Principles If the physician can’t tell a computer what he or she did, then he or she won’t get credit for the work. New system – Clinic work is additive – One issue = small bill – Many issues = big bill Incentivize primary care to provide as comprehensive care as possible. Solution - Principles Incentives – No incentive to order tests – No incentive to order treatments Both of these incentives exist in the current system. My System Innovations – Documentation Chronic diseases – – – – – – – Effect on Quality of Life Effect on Functionality Adherence and Tolerance to Medications Pertinent Physical Examination Pertinent Lab/X-ray results Maximal Medical State (Treatment Goal) Treatment Plan New System – Coding Issues Addressed code -- IA.x Becomes primary code – Replaces existing CPT codes (99213, etc.) 3 Levels – 3, 2, 1 – Level billed is a function of Thoroughness and primary care Responsibility New System – New Codes and Fees (a few examples) Work Requiring Extra Time – Example: Advance Directive Discussions Global Fees (care coordination) – Different approach Non-Face-to-Face Work – Emails, phone calls, text messages Discourage Excessive Utilization - Professionalism Few Examples: – Clear statement that one of the goals of primary care is to be a good steward of medical resources – Use generic medications whenever possible – Spread out visits for patients with stable chronic diseases Validation of This System I observed family physicians in private practices I recorded – Times – Number of Issues Addressed – Which issues addressed – Procedures, referrals, expensive tests ordered, labs, X-rays, etc. Typical Practice Avg. visit length Avg. # issues/visit Issues Addressed – Thorough – Moderate – Brief Avg. # Tests and RXs Avg. Fee Collected Avg. New System Fee 17.5 min. 3.5 0.8 1.8 0.9 1.6 1.0 $99 $117 Typical Practice Declined patient requests for services – $3 declined services for each $1 of revenue Some unnecessary services – About $1 unnecessary services for $1 revenue – My system includes incentives to lower this amount Validity - # Issues Good agreement between me and observed physician for number of issues addressed in each visit # Issues Addressed Count Complete Agreement 7 6 5 Observed 4 Physician's 3 Count 2 1 0 0 1 2 3 4 My Count R2 = 0.66, P< .001 5 6 7 8 Validity – New Fee vs. # of Issues Addressed Number of Issues vs. New Fee 8 7 6 5 # of Issues 4 3 2 1 0 $0 $50 $100 $150 New Fee R2 = 0.77, P<.001 $200 $250 Examples – Quick Visit Example: Longer Visit * Existing CMS fees Comparison to MultiDoctor Approach Issue Doctor Migraines Neurologist $103 Hypertension Cardiologist $69 High Cholesterol Lipid-ologist $69 Foot Pain Podiatrist X-Ray Radiologist $52 Low Back Pain Orthopedist $69 Preventive Care Family Physician $131 Post-Menopausal Bleeding Gynecologist $267 TOTAL 8 $918 * Assumes no facility fees CMS Current Fee* $158 Modeling of New Approach: Effect on Physician Income Income under existing rules/fees – $169,000 Income under my new approach, no change in practice style – $245,000 Income assuming FP is a little more thorough – $283,000 Effect on Physician Income Income assuming more thorough plus capture more non-face-to-face fees (emails, phone calls, etc.) – $326,000 Income assuming above plus other incentives to provide full basket of services and not overtest or overtreat. – $417,000 Run Chart Finally Lessons Learned – Colleagues for life: Others looking for answers with passion and commitment – I know more about change management and process improvement Barriers Total Cost Data – CMS: ResDAC data help – My local intermediary disappearing (Trailblazer) Funding for experiment – Myself – JPS Health Network Still might happen – CMS No luck with regional office so far Next Steps Another cycle of observations to further validate payment model. Present model to AAFP CMS – Could start using this system now!! Finally Thank you Fran Thank you mentors Thank you fellow Innovation Advisors Goodbye from the Island of Misfit Toys