Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
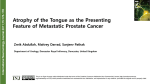
The Journal of Emergency Medicine, Vol. 35, No. 3, pp. 239 –246, 2008 Copyright © 2008 Elsevier Inc. Printed in the USA. All rights reserved 0736-4679/08 $–see front matter doi:10.1016/j.jemermed.2007.04.020 Original Contributions EVALUATION OF THIRD NERVE PALSY IN THE EMERGENCY DEPARTMENT Michael M. Woodruff, MD and Jonathan A. Edlow, MD Department of Emergency Medicine, Beth Israel Deaconess Medical Center, Boston, Massachusetts Reprint Address: Michael M. Woodruff, MD, Department of Emergency Medicine, Beth Israel Deaconess Medical Center, One Deaconess Rd., Boston, MA 02215 e Abstract—Third nerve palsy is an uncommon condition that carries significant risk of serious disease due to both the variability of its presentation and its association with intracranial aneurysms. In this article, we review the existing literature on the pathophysiology, diagnosis, and management of third nerve palsy presenting to the Emergency Department. © 2008 Elsevier Inc. CASE PRESENTATION A 59-year-old man with a history of migraines presented to the Emergency Department (ED) complaining of approximately 5 weeks of progressive double vision and a mild headache that began gradually 2–3 days prior. On the day of presentation, the patient had noted left facial and eye pain that was described as “sharper” in nature, and unusual. The patient had vomited once before arrival. In the ED, the patient appeared comfortable and had normal vital signs. There was ptosis of the left eyelid, with a sluggishly reactive pupil and partial inability to adduct the left eye. In its resting position, the left eye was deviated laterally and inferiorly. On further examination, there was no chemosis or proptosis of the affected eye, and visual acuity was normal. The contralateral eye was completely normal. Cranial nerves II and IV–XII were normal. Strength, sensation, reflexes, and cerebellar function were normal. The neurology team was consulted, and they agreed that this was a case of isolated partial CN III palsy. A magnetic resonance imaging (MRI) scan of the brain was normal, and magnetic resonance angiography (MRA) showed no evidence of an aneurysm causing the CN III dysfunction. The emergency physician and the neurologist agreed that the patient had a high pre-test probability of an aneurysm causing this type of CN III palsy; therefore, the neurosurgeon was consulted, and a traditional catheter angiogram was performed. A 5-mm saccular aneurysm was discovered originating from the posterior e Keywords—third nerve palsy; emergency medicine; cranial neuropathy; dilatated pupil INTRODUCTION Of all the cranial nerve palsies, isolated dysfunction of the third nerve (CN III) is a particularly thorny issue for the emergency physician. Although rare, it is a condition that demands thorough and appropriate evaluation due to its frequent association with intracranial aneurysms (1,2). Furthermore, the clinical presentation of third nerve dysfunction is remarkably varied— the nerve supplies seven different muscles, and almost any combination of these can be affected to varying degrees. Over the past 50 years, a good deal of work has been done to define the anatomic and pathologic features of third nerve palsies to enable clinicians to determine when an aneurysm might be the cause of the palsy. In this article we review the existing literature on CN III palsy and offer a straightforward approach to the problem that is useful to the practicing emergency physician. RECEIVED: 18 October 2005; FINAL ACCEPTED: 12 November 2006 SUBMISSION RECEIVED: 27 June 2006; 239 240 M. M. Woodruff and J. A. Edlow communicating artery. After lengthy discussions, the patient opted for endovascular coiling of the aneurysm, because the risk of rupture of symptomatic aneurysms is likely to be higher than that of asymptomatic aneurysms. QUESTION 1: IS THIS A THIRD NERVE PALSY? The presentation of third nerve palsy is extremely varied, so the clinician must think of this possibility with complaints relating to the eye. A CN III dysfunction can present with diplopia, ptosis, eye pain, headache, pupillary dilatation, monocular blurry vision, or any combination thereof (3). Unfortunately, the differential diagnosis for these complaints is broad and includes myasthenia gravis, botulism, orbital infections, orbital trauma, lens pathology, retinal pathology, migraine, and dysfunction of cranial nerves III, IV, and VI. A careful history will quickly narrow the differential. For example, it must be established whether the diplopia is monocular (does not resolve with closing one eye) or binocular (resolves on closing one eye), because the differential diagnosis for monocular diplopia is generally limited to refractive or ocular problems. The physician must search for any associated symptoms, such as facial or extremity weakness, fevers, or changes in speech, gait, or coordination that might suggest the presence of intracranial infection, hemorrhage, ischemia, or mass. If any historical or clinical features suggest spontaneous subarachnoid hemorrhage (e.g., sudden onset of severe headache, meningismus, photophobia) a non-contrast head computed tomography (CT) scan should be performed; if CT is non-diagnostic, lumbar puncture should be performed. Although opthalmoplegic migraine can cause CN III palsy, the diagnosis of migraine headache in a patient without a history of such should not be made without neurologic workup. To confirm the diagnosis of CN III palsy, the physician must perform a detailed physical examination of the eye. CN III has a number of motor functions (Table 1). To examine the pupil, a light is shined directly into the eye, and note is made of the degree of constriction of the iris muscle. Bright ambient light may interfere with this examination by constricting the pupil too much, so ideally the room lights should be dimmed. The process is repeated in the opposite eye, and the two responses are compared. The consensual reflex (constriction of the contralateral pupil with illumination of the ipsilateral pupil) is also noted. If CN III is affected, the ipsilateral pupil will react sluggishly to both direct and consensual light. If the pupil involvement is “complete,” the pupil will not react at all. To examine the levator palpebrae muscle, note is made of the portion of the iris that is covered by the upper lid, and compared with the opposite side. Ptosis can be exaggerated by having the patient look up. If ptosis is present, the patient should be tested for lid fatigue: the ptosis may worsen when the patient refrains from blinking for a time or attempts to maintain upgaze. Ptosis from myasthenia gravis is often asymmetric, fatigable, and improves with short periods of rest (4). Other conditions causing ptosis include Horner’s syndrome, botulism (or injection of botulinum toxin), palpebral trauma, and cluster headache; ptosis also may be congenital (5). “Pseudoptosis” is caused by enopthalmos (e.g., from an orbital blowout fracture), which makes the lid seem to be relatively lower on the side with the sunken globe. Examination of the extraocular muscles should begin with inspection of the resting position of the pupils when the gaze is directed straight ahead. Subtle differences in the orientation of the pupils can be detected by noting the position of the reflection of the examiner’s light in the pupil and comparing it to the opposite pupil. The patient is then asked to perform ductions, or movement of the eyes through all the cardinal directions. Any or all of the motor divisions of CN III may be affected, and palsy may be complete or partial; if there is complete palsy of the oculomotor functions of CN III, the patient will be unable to elevate or adduct the corresponding eye and the eye will assume the classic “down and out” resting position (Figure 1). This is due to the remaining input of Table 1. Individual Functions of CN III Muscle Action How to Test Pupillary Constrictor Ciliary muscles Miosis (pupillary constriction) Accommodation (thickening of the lens) Levator palpebrae superioris Superior rectus Inferior rectus Inferior oblique Medial rectus Opening of eyelid Supero-lateral gaze Infero-lateral gaze Supero-medial gaze Adduction Shine light in each eye, compare response Watch pupillary response as light is brought close to patient’s nose Examine resting position of lid relative to pupil Test lateral/supero-lateral gaze Test lateral/infero-lateral gaze Test medial/supero-medial gaze Test medial gaze Third Nerve Palsy in the ED Figure 1. Complete CN III palsy. The affected eye assumes a “down and out” resting position due to unopposed input from CN VI and CN IV. The pupil is dilatated and ptosis is present. the abducens nerve (CN VI—abduction of the eye) and the trochlear nerve (CN IV—abduction and depression of the eye). In addition to examination of the cranial nerves, the physical examination for diplopia or eye pain should include inspection for chemosis or conjunctival injection, proptosis, or evidence of trauma to the eye. If any physical examination findings are not consistent with CN III palsy, other diagnoses should be considered. Differentiating Third Nerve Palsy from Other Causes of the Isolated Dilatated Pupil Although there are very few data in the literature regarding CN III palsy presenting as an isolated dilatated pupil with normal oculomotor function and without ptosis, it is generally agreed to be extremely rare; an aneurysmal cause is even rarer (6). The more common causes of the isolated dilatated pupil include exposure to pharmacologic agents, trauma to the iris or ciliary ganglion, glaucoma, and Adie’s tonic pupil. These can be determined using simple tests that can be performed in the ED. A number of authors have suggested a stepwise approach to determining the etiology of a dilatated pupil (7,8). First, determine whether the pupil reacts normally. If it constricts briskly to direct light, then the problem may be a lack of sympathetic tone in the contralateral eye, making the “normal” ipsilateral eye appear dilatated. This can be caused by disruption of the sympathetic pupillary fibers (such as in Horner’s syndrome) or by pharmacologic agents such as pilocarpine. Additionally, up to 20% of the population may have a slight physiologic anisocoria, usually 1 mm or less (9). In general, the pupil that reacts slowly to light is the abnormal one. Visual acuity and visual fields should be carefully tested; ipsilateral optic nerve injury may result in a relative afferent pupillary defect and vision loss. Relative afferent pupillary defect is elicited with the swinging flashlight test; the pupil will show decreased constriction 241 to direct illumination, but will constrict normally when the contralateral eye is illuminated. Next, test the extraocular movements. Normal extraocular movements make a third nerve palsy very unlikely. If extraocular movements are affected, the third nerve palsy should be further investigated, as described later in this article. With normal eye movements, the next step is to exclude a pharmacologic cause. A careful history directed at any inadvertent exposures to mydriatics is essential. Some authors recommend instilling topical 1% pilocarpine into the affected eye; in the case of pharmacologic blockade by parasympatholytics (scopolamine, atropine), the pupil will not constrict; in the case of third nerve palsy, the pupil will constrict briskly. In the case of mydriasis caused by sympathomimetics, the pupil will also constrict, but these patients also should have blanched conjunctivae and a retracted upper eyelid (10). Next, perform a careful slit-lamp examination. Structural abnormalities of the iris and anterior chamber can cause acute sphincter dysfunction, and usually present with a history of ocular trauma, visual loss, or eye pain. Slit lamp examination may reveal sphincter tears. Intraocular pressure should be measured to exclude angleclosure glaucoma. If the preceding diagnostic steps have been performed and no definite etiology has been determined, the patient may have a tonic pupil. Adie’s tonic pupil syndrome is believed to be a defect affecting parasympathetic pupil fibers after they leave the ciliary ganglion. The condition occurs more frequently (70%) in women, and the patient will often present with blurred near vision, with relative sparing of distance vision. Examination shows poor response to accommodation, and a slit-lamp examination will reveal sector palsies of the iris. Because the iris is functionally denervated, the pupil will show super-sensitivity to low-dose (0.063– 0.125%) pilocarpine (11). A weaker concentration of pilocarpine is preferred, as stronger concentrations may cause a normal pupil to constrict and yield false-positive results. Adie’s pupil requires non-emergent referral to an ophthalmologist. Approximately 50% will recover within 2 years. QUESTION 2: IS THIS AN ISOLATED CN III PALSY? CN III is most often affected in combination with other cranial nerves, particularly II, IV, V, and VI. An understanding of the anatomy of the third nerve can help identify neurological deficits that frequently accompany CN III palsy. A careful cranial nerve examination, in conjunction with a general neurological examination (in- 242 cluding observing the patient’s gait), will differentiate an isolated CN III palsy from the more common situation where multiple neurological deficits are present. Midbrain/Brainstem The nerve begins with a cluster of nuclei near the center of the midbrain, at the level of the superior colliculus; nerve fascicles exit ventrally through the brainstem into the interpeduncular cistern (12,13). Isolated CN III palsy has been reported from brainstem lesions, but lesions in this region usually affect surrounding cerebellar or brainstem structures, and cause a number of syndromes: Weber’s syndrome (CN III palsy with contralateral limb weakness), Benedikt’s syndrome (CN III palsy with contralateral cerebellar tremor), Nothnagel’s syndrome (CN III palsy with cerebellar ataxia), or internuclear ophthalmoplegia (adduction weakness with contralateral nystagmus upon abduction) (14 –17). Infarction, arteriovenous malformation, cavernous hemangioma, neoplasm, multiple sclerosis, and traumatic injury have been implicated in this type of lesion (18,19). Subarachnoid Space In the subarachnoid space of the interpeduncular cistern, the nerve passes the basilar artery, superior cerebellar artery, and travels in close proximity to the posterior communicating artery (Figure 2). Because there are few other neural structures in this area, aneurysms of the posterior communicating artery, basilar artery, and superior cerebellar artery tend to cause an isolated CN III palsy. Figure 2. Superior view of the Circle of Willis. An aneurysm arising from the posterior communicating artery is shown compressing papillary motor fibers in the supero-medial aspect of CN III. M. M. Woodruff and J. A. Edlow Cavernous Sinus The nerve then enters the cavernous sinus, where it is in close proximity to nerves IV, V, VI, and the carotid artery (20). Lesions in this region (cavernous sinus thrombosis, carotid artery aneurysms) typically involve some combination of III, IV, V, or VI palsy, along with evidence of impaired venous drainage from the eye (chemosis or proptosis). Orbital Apex In the cavernous sinus, the nerve divides into superior and inferior divisions, then enters the orbital apex through the superior orbital fissure, where it travels with the optic nerve, ophthalmic artery, nerve VI, and the nasociliary branch of V1 (21). Lesions affecting CN III in the orbital apex are usually accompanied by facial numbness (superior division of CN V) and visual loss (CN II) (22). QUESTION 3: WHAT IS THE RISK OF INTRACRANIAL ANEURYSM WITH ISOLATED CN III PALSY? The key issue to address for a patient presenting with CN III palsy is whether or not the palsy is caused by an intracranial aneurysm. Several recent studies have clarified the natural history of unruptured intracranial aneurysms: the 5-year risk of rupture is highly variable (between 0% and 50% per year), and depends on size and location of the aneurysm. The aneurysms with the highest rates of rupture (posterior communicating and basilar tip aneurysms) are also the aneurysms most likely to cause an isolated CN III palsy; these posterior circulation aneurysms have a rate of rupture between 2.5% and 50%, depending upon the size of the aneurysm (23). In addition, cranial nerve palsy from an aneurysm likely reflects an acute change (hemorrhage or expansion) in the aneurysm; these aneurysms may have a higher risk of rupture. When intracranial aneurysms rupture, the subsequent mortality and morbidity are extremely high. A large percentage of patients die from the initial rupture, and the rest (up to 70% in some series) experience significant morbidity from rebleeding or subsequent vasospasm and stroke (24 –27). Although some debate exists about the best strategy for management of unruptured but symptomatic intracranial aneurysms, it is a diagnosis that carries significant risk, and should be established or excluded with urgency (28). Isolated CN III palsy is a relatively rare phenomenon: the exact incidence has not been established in the liter- Third Nerve Palsy in the ED ature, but roughly 1300 cases were reported at the Mayo Clinic between 1958 and 1992 (29). A significant number (18 –29% in the larger series) of isolated CN III palsies, however, are caused by cerebral aneurysms (1,30). Over the years, a number of authors have attempted to define clinical and historical factors that identify patients at risk of having an aneurysmal cause of CN III palsy. This approach is supported by anatomical data and case series, but due to the low incidence of the disease, not by large prospective studies. CN III dysfunction can be classified according to whether the pupil is involved (pupil-involving or pupilsparing) and the degree of extraocular muscle dysfunction (partial or complete). This distinction is important because it has long been held that when an aneurysm (or other compressive lesion) is the cause of third nerve palsy, the pupil will almost always (95–97% of the time) be involved; this has become known as “the rule of the pupil” (1,31). The anatomic basis of the rule of the pupil is the arrangement of the pupillary constrictor fibers within the subarachnoid portion of the nerve. Fibers that supply the pupillary constrictors are located superficially in the dorsomedial aspect of the nerve (Figure 2), and are readily compressed by an aneurysm arising from the posterior communicating artery (32). In early retrospective case series, there seems to be a subset of third nerve palsies that do not involve the pupil at all, and occur mainly in people with diabetes, hypertension, or with other vasculopathic risk factors (33,34). These cases of CN III palsy tend to resolve over time, and are attributed to pathologic changes in the vasa nervorum and ischemic injury to the axons located deeper within the nerve bundle. Thus, the rule of the pupil came to mean that patients with pupil-sparing CN III palsy, particularly those over age 50 years with vasculopathic risk factors, could safely be managed with outpatient observation, and without cerebral angiography. This type of pupil-sparing CN III palsy has become known as “diabetic third nerve palsy.” The mechanism of this type of CN III palsy is not well delineated, but pathological studies have revealed arteriolar thickening and demyelinating lesions consistent with microvascular ischemia of the nerve (35,36). Although there has been one case report of a pupilsparing complete oculomotor palsy caused by a basilar apex aneurysm, it is generally accepted that patients over the age of 50 years with vasculopathic risk factors and complete pupil-sparing CN III palsy can be observed as outpatients without neuroimaging (6,33,37). This should be done in consultation with a neurologist or a neuroophthalmologist. Younger patients without strong risk factors should undergo neuroimaging before the diagnosis of microinfarctive or “diabetic” palsy is made. 243 The “rule of the pupil” has an important caveat: there have been numerous cases of incomplete CN III palsies caused by aneurysms that do not involve the pupil (2,38 – 41). These partial extraocular palsies are likely due to the fact that initially an aneurysm (in particular a basilar apex aneurysm) may not compress the supero-medial aspect of the nerve where the pupillary fibers travel. Many partial oculomotor palsies that initially seem to spare the pupil will eventually go on to involve the pupil (33). IMAGING DETECTION OF INTRACRANIAL ANEURYSMS Magnetic resonance imaging of the brain and cerebral vessels is generally the preferred method of imaging third nerve palsies, because it provides not only a means of identifying intracranial aneurysms, but also a means of identifying non-aneurysmal causes of CN III palsy such as tumor and inflammatory conditions. The sensitivity of MRA for aneurysms has increased in recent years as the technology improves. Sensitivities between 88% and 97% have been reported for larger (⬎ 5 mm) aneurysms, lower for smaller aneurysms (42,43). There is evidence, though, that some types of aneurysms (e.g., thrombosed and low-flow aneurysms) may be difficult to detect with MRI, regardless of size. In addition, some patients cannot undergo MRI scan due to implanted materials, claustrophobia, or inability to lie still for a relatively lengthy scan. Computed tomography angiography (CTA) has the advantages of being rapid, less invasive, and a lower contrast load than contrast angiography. It also provides a three-dimensional picture of the aneurysm and the relevant skull-base anatomy. Sensitivity varies with aneurysm size, ranging from 86 –97% (44,45). Catheter angiography, although traditionally the gold standard for diagnosing aneurysms, carries a small risk (approximately 1%) of neurologic morbidity and a small risk of mortality. The emergency physician is unlikely to be ordering this test without the involvement of a consultant, but should be aware that it is an option in the evaluation of CN III palsy. SUMMARY: DIAGNOSTIC APPROACH (FIGURE 3) Two subsets of CN III palsy seem to be at lower risk for intracranial aneurysm. The first is the isolated dilatated pupil. In the comatose patient, unilateral pupillary dilatation is often due to CN III compression by the medial temporal lobe in the setting of elevated intracranial pres- 244 M. M. Woodruff and J. A. Edlow Figure 3. Schema for evaluation of third nerve palsy. sure: this is obviously an emergency. But in the awake, neurologically normal patient with a dilatated pupil and no other complaints, CN III palsy is exceedingly unlikely. Investigation in this situation should be aimed at identifying the cause of pupil palsy (see previous text). The second subset is the complete pupil-sparing CN III palsy or “diabetic” CN III palsy. The existing evidence suggests that if the patient fits the appropriate profile (diabetic or other risk factors for microvascular disease, age over 50 years), the patient may be safely discharged with outpatient neurological follow-up. All other types of isolated CN III palsy carry a higher risk of intracranial aneurysm, and should prompt neuroimaging and consultation with a neurologist. In particular, complete pupilinvolving and partial pupil-involving CN III palsies represent the highest risk for aneurysm—in one study, 36% of CN III palsies caused by aneurysm had complete pupil involvement and complete extraocular palsy (2). Although obviously a decision that should be made in consultation with a specialist, some authors recommend proceeding to conventional catheter angiography in these patients if MRA or CTA scan is negative. Some attempts have been made in the literature to define the risk of aneurysm by whether the oculomotor palsy is partial or complete; however, there is very little standardization in the neuro-ophthalmologic literature regarding the definition of a complete CN III palsy. Thus, this is probably a determination best made by a neurologist or neuroophthalmologist and not by the emergency physician. In general, it is our opinion that as neuroimaging modalities become more accessible, the approach to imaging of third nerve palsy is becoming (appropriately) Third Nerve Palsy in the ED more liberal. The existing literature on CN III palsy is largely from referral ophthalmology and neurology clinics, and probably does not represent the population seen in the ED. In addition, the physicians evaluating the patients in these case series are specialists with a great deal of experience with the evaluation of cranial nerve palsy. Much of the literature is also from the pre-MRA/ CTA era, and may reflect a different approach to imaging than is currently recommended. Therefore, we advocate a conservative approach to the workup of third nerve palsies, with liberal use of consultation and imaging. The decision of whether and how to image a CN III palsy is best made in consultation with a specialist. Specifically, the decision to follow an MRA or CTA scan with catheter angiography is based on the clinical likelihood of an intracranial aneurysm as determined from the patient’s symptoms, risk factors, and physical examination. The clinician must be aware of the limitations of the various imaging tests available, and recognize that if a high pre-test probability of aneurysm exists, the post-test probability may still be unacceptably high, even with a negative test result (46). Acknowledgment—The authors acknowledge the help of Jane Hayward and Jennifer McGrath in preparing the illustrations. REFERENCES 1. Green WR, Hackett ER, Schlezinger NS. Neuro-ophthalmologic evaluation of oculomotor nerve paralysis. Arch Ophthalmol 1964; 72:154 – 67. 2. Kissel JT, Burde RM, Klingele TG, Zeiger HE. Pupil-sparing oculomotor palsies with internal carotid-posterior communicating artery aneurysms. Ann Neurol 1983;13:149 –54. 3. Biousse V, Newman NJ. Third nerve palsies. Semin Neurol 2000; 20:55–74. 4. Scherer K, Bedlack RS, Simel DL. Does this patient have myasthenia gravis? JAMA 2005;293:1906 –14. 5. Finsterer J. Ptosis: causes, presentation, and management. Aesthetic Plast Surg 2003;27:193–204. 6. Lee AG, Hayman LA, Brazis PW. The evaluation of isolated third nerve palsy revisited: an update on the evolving role of magnetic resonance, computed tomography, and catheter angiography. Surv Ophthalmol 2002;47:137–57. 7. Lee AG, Taber KH, Hayman LA, Tang RA. A guide to the isolated dilated pupil. Arch Fam Med 1997;6:385– 8. 8. Thompson S, Pilley SF. Unequal pupils. A flow chart for sorting out the anisocorias. Surv Ophthalmol 1976;21:45– 8. 9. Lam BL, Thompson HS, Corbett JJ. The prevalence of simple anisocoria. Am J Ophthalmol 1987;104:69 –73. 10. Anastasi LM, Ogle KN, Kearns TP. Effect of pilocarpine in counteracting mydriasis. Arch Ophthalmol 1968;79:710 –5. 11. Bourgon P, Pilley FJ, Thompson HS. Cholinergic supersensitivity of the iris sphincter in Adie’s tonic pupil. Am J Ophthalmol 1978;85:373–7. 12. Miller MJ, Mark LP, Ho KC, Haughton VM. Anatomic relationship of the oculomotor nuclear complex and medial longitudinal fasciculus in the midbrain. AJNR Am J Neuroradiol 1997;18: 111–3. 245 13. Porter JD, Guthrie BL, Sparks DL. Innervation of monkey extraocular muscles: localization of sensory and motor neurons by retrograde transport of horseradish peroxidase. J Comp Neurol 1983; 218:208 –19. 14. Keane JR. Isolated brain-stem third nerve palsy. Arch Neurol 1988;45:813– 4. 15. Mark AS. Oculomotor motion disorders: current imaging of cranial nerves 3, 4, and 6. Semin Ultrasound CT MR 1998;19:240 –56. 16. Liu GT, Crenner CW, Logigian EL, Charness ME, Samuels MA. Midbrain syndromes of Benedikt, Claude, and Nothnagel: setting the record straight. Neurology 1992;42:1820 –2. 17. Biller J, Shapiro R, Evans LS, Haag JR, Fine M. Oculomotor nuclear complex infarction. Clinical and radiological correlation. Arch Neurol 1984;41:985–7. 18. Keane JR, Zaias B, Itabashi HH. Levator-sparing oculomotor nerve palsy caused by a solitary midbrain metastasis. Arch Neurol 1984;41:210 –2. 19. Stevenson GC, Hoyt WF. Metastasis to midbrain from mammary carcinoma. Cause of bilateral ptosis and ophthalmoplegia. JAMA 1963;186:514 – 6. 20. Harris FS, Rhoton AL. Anatomy of the cavernous sinus. A microsurgical study. J Neurosurg 1976;45:169 – 80. 21. Morard MV, Tcherekayev V, de Tribolet N. The superior orbital fissure: a microanatomical study. Neurosurgery 1994;35:1087–93. 22. Yeh S, Foroozan R. Orbital apex syndrome. Curr Opin Ophthalmol 2004;15:490 – 8. 23. Wiebers DO, Whisnant JP, Huston J 3rd, et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 2003;362:103–10. 24. Kassell NF, Torner JC, Haley EC Jr, Jane JA, Adams HP, Kongable GL. The International Cooperative Study on the Timing of Aneurysm Surgery. Part 1: overall management results. J Neurosurg 1990;73:18 –36. 25. Kassell NF, Torner JC, Jane JA, Haley EC Jr, Adams HP. The International Cooperative Study on the Timing of Aneurysm Surgery. Part 2: surgical results. J Neurosurg 1990;73:37– 47. 26. Rabinstein AA, Weigand S, Atkinson JL, Wijdicks EF. Patterns of cerebral infarction in aneurysmal subarachnoid hemorrhage. Stroke 2005;36:992–7. 27. Parra A, Kreiter KT, Williams S, et al. Effect of prior statin use on functional outcome and delayed vasospasm after acute aneurysmal subarachnoid hemorrhage: a matched controlled cohort study. Neurosurgery 2005;56:476 – 84. 28. Wardlaw JM, White PM. The detection and management of unruptured intracranial aneurysms. Brain 2000;123:205–21. 29. Richards BW, Jones FR Jr, Younge BR. Causes and prognosis in 4,278 cases of paralysis of the oculomotor, trochlear, and abducens cranial nerves. Am J Ophthalmol 1992;113:489 –96. 30. Rucker CW. The causes of paralysis of the third, fourth and sixth cranial nerves. Am J Ophthalmol 1966;61:1293– 8. 31. Rucker CW. Paralysis of the third, fourth and sixth cranial nerves. Am J Ophthalmol 1958;46:787–94. 32. Kerr WL, Hollowell OW. Location of pupillomotor and accommodation fibres in the oculomotor nerve: experimental observations on paralytic mydriasis. J Neurol Neurosurg Psychiatry 1964; 27:473– 81. 33. Trobe JD. Third nerve palsy and the pupil. Footnotes to the rule. Arch Ophthalmol 1988;106:601–2. 34. Goldstein JE, Cogan DG. Diabetic ophthalmoplegia with special reference to the pupil. Arch Ophthalmol 1960;64:592– 600. 35. Asbury AK, Aldredge H, Hershberg R, Fisher CM. Oculomotor palsy in diabetes mellitus: a clinico-pathological study. Brain 1970;93:555– 66. 36. Said G, Goulon-Goeau C, Lacroix C, Moulonguet A. Nerve biopsy findings in different patterns of proximal diabetic neuropathy. Ann Neurol 1994;35:559 – 69. 37. Lustbader JM, Miller NR. Painless, pupil-sparing but otherwise complete oculomotor nerve paresis caused by basilar artery aneurysm. Case report. Arch Ophthalmol 1988;106:583– 4. 246 38. Ajtai B, Fine EJ, Lincoff N. Pupil-sparing, painless compression of the oculomotor nerve by expanding basilar artery aneurysm: a case of ocular pseudomyasthenia. Arch Neurol 2004;61:1448 –50. 39. Bartleson JD, Trautmann JC, Sundt TM Jr. Minimal oculomotor nerve paresis secondary to unruptured intracranial aneurysm. Arch Neurol 1986;43:1015–20. 40. Kasoff I, Kelly DL Jr. Pupillary sparing in oculomotor palsy from internal carotid aneurysm. Case report. J Neurosurg 1975;42: 713–7. 41. Guy J, Savino PJ, Schatz NJ, Cobbs WH, Day AL. Superior division paresis of the oculomotor nerve. Ophthalmology 1985;92: 777– 84. 42. Huston J 3rd, Nichols DA, Luetmer PH, et al. Blinded prospective evaluation of sensitivity of MR angiography to known intracranial aneurysms: importance of aneurysm size. AJNR Am J Neuroradiol 1994;15:1607–14. M. M. Woodruff and J. A. Edlow 43. Chung TS, Joo JY, Lee SK, Chien D, Laub G. Evaluation of cerebral aneurysms with high-resolution MR angiography using a section-interpolation technique: correlation with digital subtraction angiography. AJNR Am J Neuroradiol 1999;20:229 –35. 44. Villablanca JP, Jahan R, Hooshi P, et al. Detection and characterization of very small cerebral aneurysms by using 2D and 3D helical CT angiography. AJNR Am J Neuroradiol 2002;23:1187–98. 45. Anderson GB, Steinke DE, Petruk KC, Ashforth R, Findlay JM. Computed tomographic angiography versus digital subtraction angiography for the diagnosis and early treatment of ruptured intracranial aneurysms. Neurosurgery 1999;45:1315–20; discussion 1320 –2. 46. Johnson MR, Good CD, Penny WD, Barnes PR, Scadding JW. Lesson of the week: playing the odds in clinical decision making: lessons from berry aneurysms undetected by magnetic resonance angiography. BMJ 2001;322:1347–9.