Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Herpes simplex virus wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Neonatal infection wikipedia , lookup
Oesophagostomum wikipedia , lookup
Onchocerciasis wikipedia , lookup
Chagas disease wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Marburg virus disease wikipedia , lookup
Meningococcal disease wikipedia , lookup
Hepatitis C wikipedia , lookup
Leishmaniasis wikipedia , lookup
Schistosomiasis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Hepatitis B wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
Leptospirosis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
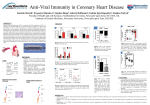
How I Manage CMV in the PostTransplant Patient Camille Nelson Kotton M.D. Clinical Director, Transplant and Immunocompromised Host Infectious Diseases Group Massachusetts General Hospital, Associate Prof.,Harvard Medical School Chair, Infectious Disease Community of Practice, American Society of Transplantation Past-President, The Transplant Infectious Disease Section, The Transplantation Society Disclosures Camille Nelson Kotton MD, FIDSA, FAST • Consultant: – Merck, Genentech (CMV therapeutics) – Astellas, AstraZeneca (CMV Vaccines) – Roche Molecular Systems, Cellestis-QIAGEN & Oxford Immunotec (transplant infectious disease diagnostics) • Adjudication committees: Merck, Astellas • Research projects with Oxford Immunotec and Cellestis-QIAGEN • Spouse has no significant financial disclosures • May discuss off-label use of diagnostics, medications, and vaccines How I Manage CMV after Transplant • Prevention • Diagnostics – Molecular – Immunologic • Therapeutics • Vaccines • Genetic risk stratification • Focus on what’s new in 2015 3 4 Direct Effects of CMV Infection Direct Effects CMV Viral Syndrome • • Tissue-Invasive Disease Flu-like syndrome: fever, malaise, myalgias • Leukopenia, thrombocytopenia • • • • • • • Colitis Hepatitis Pneumonitis Myocarditis Nephritis Encephalitis Retinitis Pancreatitis Adapted from Torres-Madriz G, Boucher HW. Clin Infect Dis. 2008;47:702-11. 5 Indirect Effects of CMV General indirect effects–elevated risks Transplant-specific indirect effects •Bacterial, fungal, viral infections • Chronic allograft nephropathy and/or allograft loss after renal transplant • Accelerated hepatitis C recurrence after liver transplant • Hepatic artery thrombosis after liver transplant • Allograft vasculopathy after cardiac transplant • Bronchiolitis obliterans after lung transplant •Post-transplant lymphoma (PTLD) •Cardiovascular events •New-onset diabetes mellitus after transplantation •Immunosenescence •Acute rejection •Mortality from Kotton, CMV: Prevention, Diagnosis and Therapy, AJT 2013 Transplantation 2015 D+R- D+R- prophylaxis prophylaxis 61,927 adult recipients of deceased donor kidney transplant 1990 to 2012 in the Collaborative Transplant Study 7 PREVENTION: Prophylaxis versus Preemptive Therapy Prophylaxis period (typically 3–6 months) after transplantation More common after SOT Antiviral prophylaxis Preemptive monitoring period (once weekly for 12-16 weeks); If CMV is detected (PCR or pp65 Ag), treat until CMV is cleared 0 4 8 12 16 Weeks Humar A, Snydman D. Am J Transplant. 2009;9 (suppl 4):S78-86. 20 24 More common after HSCT 28 8 Comparison of Known Benefits and Limitations of Prophylaxis vs Preemptive Therapy Prophylaxis Preemptive Therapy Rare Common Good efficacy Good efficacy* (*less optimal in high risk populations) Common Rare Uncommon Uncommon Relatively easy More difficult Prevents HSV, VZV Does not prevent May prevent Unknown Drug costs Monitoring costs Drug side effects Less drug toxicity Prevention of rejection May prevent Unknown Graft survival May improve May improve Early CMV DNAemia Prevention of CMV disease Late CMV (infection/disease) Resistance Ease of implementation Other herpesviruses Other Opportunistic infections Cost Safety Kotton CN et al. Updated International Consensus Guidelines on the Management of Cytomegalovirus in Solid-Organ Transplantation. Transplantation. 2013;96(4):333-360. 9 Massachusetts General Hospital Protocol: CMV/Herpes/Varicella Prophylaxis after Renal, Liver, Heart, or Pancreas Transplant Induction Donor agent CMV Antibody Recipient CMV Antibody Prophylaxis Thymoglobulin + + (polyclononal antithymocyte globulin) - + + - Valganciclovir x 6 months - - acyclovir/famvir/valacyclovir x 3 mos + + - + + - - - + + - + + - - - Basiliximab (IL-2 antagonist) None Monitoring with CMV viral load while on prophylaxis valganciclovir x 3 mos plus monthly monitoring afterwards x 3 months valganciclovir x 3 mos acyclovir/famvir/valacyclovir x 3 mos valganciclovir x 3 mos acyclovir/famvir/valacyclovir x 3 mos 10 Not needed - only if clinically indicated by symptoms HYBRID Strategy: Preemptive Therapy After Prophylaxis • High Risk (D+R-) may be highest yield population (for late disease) • Other high risk groups (potent immunosuppression) • Guidelines experts use approach, not strongly evidence-based CMV disease CMV viral load assay: 0 Prophylaxis + + + + 4 + 8 + + - - 12 months Could have initiated preemptive therapy before disease developed 11 Stringent adherence to a CMV-prevention protocol is associated with reduced overall costs in the first 6 months after kidney transplantation, Matter-Walstra et al, TID 2015 • Standard prevention cost Swiss francs [CHF] 104,548 (mean) versus CHF 76,983 for stringent prevention (P = 0.0005) (1 CHF = US$1.03) – Largely due to less disease in stringent group • Overall difference in CMV disease episodes did not occur in the high-risk group, rather in intermediate group with CMV seropositive recipients (R+) • Incidence of CMV disease was significantly reduced from 14 (15%) to 4 (5%) – 11% down to 1% in pre-emptive therapy group Conclusions: “The use of secondary prophylaxis was not significantly associated with fewer episodes of CMV relapse, graft loss, or death.” “Time to clearance of CMV viremia during treatment was significantly longer in those who relapsed (mean, 30 days vs. 20 days; P = 0.037).” 13 Transplant ID 2015 • 45 patients on low dose prophylaxis were evaluated: – 6 developed CMV infection while on prophylaxis (P = 0.11) – 1 developed ganciclovir (GCV)-resistant infection • Late-onset CMV infection/disease: same – 11 patients (24%) in the standard dose group – 12 patients (27%) in the low dose group (P = 0.86) • More patients in the standard dose group developed leukopenia (75% vs. 44%, P < 0.01). 14 Low dose: -6/45 developed CMV infection while receiving prophylaxis (P = 0.11). 1/45 w/ confirmed GCV-resistant infection -same rates of late CMV standard dose PPx lower dose PPx 180 days of prophylaxis 15 Stevens et al, TID 2015 Diagnostics: Molecular & Immunology Crough and Khanna, CMR, 2009 16 CMV Viral Load & International Standard • Inter-laboratory comparison: Variation observed in viral load results for individual samples ranged from 2.0 log(10) to 4.3 log(10), Pang et al, AJT 2009 • Assays at 5 transplant centers in US and Europe were compared, using international units, Hirsch et al, CID 2013 – COBAS AmpliPrep/COBAS TaqMan CMV Test superior to local assays – Results generally comparable w/ international units • Must compare same specimen type – Plasma < whole blood 17 “We predict that the era when CMV-specific T-cell immune assays are part of the standard of care for CMV at-risk SOT populations is very near”. Potential Clinical Scenarios for the Use of Cellular Immune-based Assays Clinical Scenarios Assays studied Potential clinical management* CMV D+/R- and R+ at the end of prophylaxis QFT, ELISpot, ICS For negative assay, prolong prophylaxis; For positive assay, no further prophylaxis CMV D+/R- and R+ during preemptive strategy QFT, ELISpot, ICS Result may help guide frequency of viral load monitoring and thresholds for initiating antiviral therapy Post-therapy for acute rejection ICS (small number, not predictive) For negative assay, restart prophylaxis or viral load monitoring; For positive assay, no further intervention Recent completion of therapy for CMV disease or viremia (Prediction of relapse) No studies For negative assay, secondary prophylaxis; For positive assay, no further therapy Risk stratification in patients pretransplant ICS, QFT For positive assay, assume true positive CMV status Kotton CN et al. Updated International Consensus Guidelines on the Management of Cytomegalovirus in Solid-Organ Transplantation. Transplantation. 2013;96(4):333-360. 19 Ex vivo monitoring of CMV-specific T-cell responses Modified from Crough & Khanna, CMR, 2009 T-SPOT®.CMV 20 Assessment of CMV-Specific Cell-Mediated Immunity for the Prediction of CMV Disease in High-Risk SOT Transplant Recipients: A Multicenter Cohort Study • D+R- on antiviral prophylaxis; Quantiferon CMV assay • Test done at end of PPX, then at 1, 2 months • 22% developed CMV disease • 124 patients: • 31 (25%) positive • 81 (65.3%) negative • 12 (9.7%) indeterminate result (negative mitogen) Manuel O, et al. CID 2013 Mar;56(6)817-824. 21 CMV-Specific Cell-Mediated Immunity for the Prediction of CMV Disease in High-Risk SOT Freedom from CMV Disease positive negative indeterminate Manuel O, et al. CID 2013 Mar;56(6)817-824. At 12 months, patients with a positive result had a subsequent lower incidence of CMV disease (6.4%) than patients with a negative (22.2%) and an indeterminate result (58.3%, respectively; P < .001). 22 Pre-transplant CMV–specific interferon (IFN) γ–producing T-cell responses were significantly lower among CMV IgG–seropositive (R+) kidney transplant recipients with CMV disease and viremia Disease Yes No Yes No Viremia Yes Non-commercial assay Lúcia et al, Clin Infect Dis. 2014 Jul No Yes No Factors Related to the Development of CMV-Specific CD8+ T cell Response in CMV-Seropositive SOT Transplant Candidates, Cantisán et al, AJT 2015 • CMV seropositive but lacking CMV-specific CD8+ T cell response=higher incidence of CMV replication/disease • Used QuantiFERON-CMV assay • n=141: 90 (64%) QF-CMV reactive/51 (36%) nonreactive. “Therefore, although the assessment of CMV-specific CD8+ response is recommended in all R+ candidates, it is essential in those with a lower probability of being reactive, such as nonrenal candidates, candidates under 50 or those with non-HLAA1/non-HLA-A2 alleles.” 25 Treatment of CMV • Treat with ganciclovir or valganciclovir, test viral load/antigenemia weekly, until 1-2 assays are negative (or low results (<1,000 IU)), often 2-3 weeks of treatment • VICTOR trial showed valganciclovir PO similar to ganciclovir IV for mild-moderate disease in SOT (Asberg, AJT 2009) • Foscarnet used when bone marrow suppression an issue • Concern for resistance: worsening disease or increasing viral load – Consider sending genotypic resistance testing – Consider switching to foscarnet or using high dose ganciclovir Suggested Algorithm for Managing Suspected CMV Drug Resistance Kotton CN et al. Updated International Consensus Guidelines on the Management of Cytomegalovirus in Solid-Organ Transplantation. Transplantation. 2013;96(4):333-360. 27 Optimal Dosing of GCV/VGCV Kotton CN et al. Updated International Consensus Guidelines on the Management of Cytomegalovirus in Solid-Organ Transplantation. Transplantation. 2013;96(4):333-360. 28 Novel/Emerging Therapeutics • Maribavir (Viropharma) • Letermovir (AIC246) (Merck) • Brincidofovir (CMX001) (Chimerix) • HSCT data, limited SOT • Compassionate use - challenging 29 Vaccines under Development • Astellas vaccine (ASP0113, TransVax™) w/ Vical – Plasmids encoding cytomegalovirus glycoprotein B and phosphoprotein 65 formulated with poloxamer CRL1005 and benzalkonium chloride – multinational Phase 3 trial in HSCT recipients, Phase 2 in SOT recipients • Sanofi vaccine (enveloped virus-like particles, glycoprotein B/MF59 adjuvant) w/ VBI – Kirchmeier et al, Clin Vaccine Immuno 2014, increased efficacy in animals • GSK vaccine (glycoprotein B/AS01 adjuvant) – HCMV gB (hgB) antigen, a recombinant fusion protein consisting of the extracellular domain of the native gB (AD169 strain) and peptide sequences from glycoprotein gD of Herpes Simplex virus 2 (HSV2) • Novartis (AVX601) w/ AlphaVax – single-cycle particle RNA vaccine encoding three antigens-- phosphoprotein 65, immediate early protein I, and glycoprotein B *CMV-specific T cells from a donor bank 31 Genetics & CMV: Influences of Recipients and Donors • Polymorphisms in the IFNL3/4 region influence susceptibility to CMV replication in solid-organ transplant recipients (Manuel et al, JID 2015) • Killer immunoglobulin-like receptors (KIR) (genetically polymorphic natural killer (NK) cell receptors) important in antiviral response KIR genotype impacts primary control of CMV infection after transplantation (Van Duin et al) • Toll-like receptors(TLR)-2/-4 polymorphisms influence CMV risk (Cervera et al 2007, Ducloux et al 2005, Kijpittayarit et al, 2007) • Mannan-binding lectin deficiency increases risk of CMV infection (Manuel et al 2007, numerous others) 32 Summary • Prevention is key, in both high and moderate risk groups • Novel diagnostics, therapeutics, and vaccines under active development • A better appreciation of the contribution of donor and recipient genetics may be revealing • Personalized medicine may be in the near future, via immunodiagnostics and genetics 33 Questions? [email protected] Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts, USA