Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Sarcocystis wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Toxoplasmosis wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Marburg virus disease wikipedia , lookup
Herpes simplex virus wikipedia , lookup
Schistosomiasis wikipedia , lookup
Henipavirus wikipedia , lookup
West Nile fever wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Hepatitis C wikipedia , lookup
Oesophagostomum wikipedia , lookup
Neonatal infection wikipedia , lookup
Lymphocytic choriomeningitis wikipedia , lookup
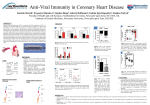
Long-term effects of CMV in the elderly By Adriaensen Wim Department of Public Health and Primary Care, KU Leuven & UCL, Belgium falling in for Prof. Catharina Matheï Cytomegalovirus Human Herpes Virus 5 (HHV-5) Double stranded DNA enveloped herpesvirus BELFRAIL serology BELFRAIL – BFc80+ prospective, observational, population-based cohort study of community-dwelling subjects total of 567 subjects (63% women) with a mean age of 85 years (range 80 - 102) were included between November 2, 2008 and September 15, 2009 29 GP centres recorded background variables and medical history and performed a detailed anamnesis and clinical examination The CRA performed an extensive examination including questionnaires and technical examinations BELFRAIL – BFc80+ High burden of comorbidity Low number of institutionalized CMV prevalence and determinants Routinely diagnosed by the detection of anti-CMV IgG & IgM antibodies. Worldwide high prevalence rates between 40-100% BELFRAIL: 74% Omsk region: 90-95% “Cytomegalovirus infection in Omsk region. Dolgikh et al. 2008 Zh Mikrobiol Epidemiol Immunobiol.” Depending on socio-economic status, gender and age. Generally lower in developed countries, due to improved hygiene in these countries. Natural History CMV is transmitted from person to person via close contact with an individual who is excreting the virus. It can be spread through the placenta, blood transfusions, organ transplantation, and breast milk. It can also be spread through sexual transmission. Natural History Persistent infections: those in which the virus is not cleared but remains in specific cells of infected individuals. Latent in the body Mainly in myeloid lineage and monocytes, epithelial cells. Involve stages of both silent and productive infection without rapidly killing or even producing excessive damage of the host cells. Might reactivate after an superinfection, periods of stress, immunodeficiency, etc. Virions appear in saliva, urine? IgM? No real chronic infection, as a chronic infection is characterized by the continued presence of infectious virus following the primary infection and may include chronic or recurrent disease. Known consequences of Cytomegalovirus Usually asymptomatic in healthy people Dangerous in: Pregnant mothers and newborns Immunocompromised situations HIV patients Transplantation CMV really innocent in healthy persons? Likewise many other infectious agents, in recent years CMV has emerged as an important long-term determinant in the development of many chronic diseases in immunocompetent hosts. Increased Risks CMV is implicated in the etiology of various chronic conditions such as atherosclerosis and cardiovascular or all-cause mortality. CMV has been identified as a risk factor for CHD A recent meta-analysis of 55 studies involving 9000 cases and 8608 controls. Ji et al. 2012 Mol Biol Rep tion to an outcome that is established at the start of the study. Most sources of error due to confounding and bias are more common in retrospective studies than in prospective studies. To investigate whether there was the heterogeneity of different study design, we stratified the group by the study design, and found that there was significant heterogeneity among retrospective studies (P = 0.000), but not among prospective studies, which showed that the heterogeneity among all the 55 studies may arise from the difference in study design. In 6 prospective studies, no significant heterogeneity (P = 0.054) was observed and the ORs (1.31, 95% CI = 1.13–1.52) was lower than the overall ORs (1.673) and the ORs (1.79) of the 49 retrospective studies. In our meta-analysis, all 6 nested case–control studies from non-Asian populations (4 USA studies, 1 Netherlands study, 1 UK study), resulting in the lower risks of CMV than Asian population (OR, 2.69) and retrospective studies. Thus, it is necessary to conduct more prospective studies using standardized unbiased methods and well matched controls among Asian population. and CHD risk Among 42 included studies, detection of antibodies for CMV IgG was performed using a commercially available enzyme-linked immunosorbent assay (ELISA) kit, other seven studies used a more sensitive test, PCR assay. The various detection methods of CMV infection can bring out the different prevalence of CMV positive radio in the included studies. In our present study, the increased risks (OR, 8.12) in PCR studies was significant higher than the risks among ELISA studies (OR, 1.561,). These findings virtually confirmed the major relationship between CMV infection and CHD risk in various detection methods of CMV infection. Some limitations of this meta-analysi s should be acknowledged. Firstly, heterogeneity is a potential problem when interpreting all the results of meta-analyses. Although we minimized the likelihood by performing a careful search for published studies, using the explicit criteria for study inclusion, performing data extraction and data analysis strictly, the significant between-study heterogeneity still Table 2 Main results of pooled odds ratios (OR) with confidence interval (CI) in the meta-analysis Number of the included studies Heterogeneity Test (Q test) OR (95% CI) P (Pooled OR test) 55 Q = 258.47; P = 0.000 1.673 (1.562–1.792) 0.000 Asian 25 Q = 87.04; P = 0.000 2.691(2.304–3.144) 0.000 Non-Asian 30 Q = 139.11; P = 0.000 1.481(1.371–1.600) 0.000 Total Ethnicity (all) Increased Risks CMV is implicated in the etiology of various chronic conditions such as atheroslecorsis and cardiovascular or all-cause mortality. The NHANES III study demonstrated that a positive CMV serostatus produces an increased risk for all-cause mortality, largely explained by an increase in cardiovascular deaths (CVD). High levels of CRP strengthened this association. Simanek et al. 2011 PLoS ONE All-cause mortality, NHANES III, n=14011 >25 years old Increased risks Evenmore, CMV has been implied in the development of cancer, inflammatory bowel diseases, frailty, physical and cognitive impairment in elderly. But this association seems to disappear in VERY elderly… CMV’s main impact was seen in individuals aged 55–75 at while CMV imposed little increased risk of mortality in the most elderly (aged 75– 90) – SIMANEK et al. BELFRAIL results: VERY elderly CMV infection was not associated with functional or cognitive impairment. Moreover, positive CMV serology was found to be negatively associated with frailty. These apparently contradictory results may reflect a survival effect because the current study population was considerably older than the populations of older adults in previous studies. This would cause individuals susceptible to the long-term deleterious effects of CMV exposure to be underrepresented in the cohort because they would have died at an earlier age. The survival analysis will give us more insight into the phenotype of the octogenarians (reverse epidemiology) Matheï C, Vaes B, Wallemacq P, Degryse J.Associations Between Cytomegalovirus Infection and Functional Impairment and Frailty in the BELFRAIL Cohort. J Am Geriatr Soc. 2011 Nov 7. doi: 10.1111/j.15325415.2011.03719.x. [Epub ahead of print] BELFRAIL Results CMV serostatus was not associated with mortality In contrast to younger populations anti-CMV IgG titer in the highest tertile or > 250 IU/ml was associated with mortality even after adjustment for age, gender, level of education, smoking status, BMI, co-morbidity and hCRP serum level. These findings suggest that CMV reactivation -apparent from increased anti-CMV IgG titers- in the oldest old may be frequently present in this age-category. Matheï et al. CMV, inflammation and mortality in the oldest old: results from the Belfrail study. Submitted BELFRAIL – Survival Curve Control of CMV reactivation We hypothesize that many among the oldest old represent a phenotype that is less susceptible for the detrimental effects of CMV because of their capacity to strongly control the infection and thereby preventing reactivation and exerting harm. However, some will eventually fail to contain the virus because of exhaustion of the immune system causing the infection to reactivate and anti-CMV IgG titers to increase. From this perspective, high anti-CMV IgG titers in the oldest old should be interpreted as a measure of general deterioration. Rather than that it plays an important role in the etiology of mortality. Through what mechanism exerts CMV its effect? The mechanisms behind these associations are not fully understood but it is believed that CMV may contribute to the chronic inflammatory state underlying most chronic diseases as a result of periodic re-activations. Chronic CMV hypothesis Immunosenescence !!! What is immunosenescence? Immunosenescence = deleterious age-associated changes to both innate and adaptive immunity Hallmarks: Inflammageing T-cell senescence (primarly CD8+) Late-stage effector-memory CD8+ T-cell accumulation In CMV-seropositive elderly, up to 50% of the overall CD8+ T-cell pool will be specific for CMV. It remains unclear why CMV alone as such a profound impact, and not other herpesviruses. It might be due to its abundant presence in the body and efficient interaction with immune cells. Take-home messages CMV also appears to have long-term effects in immunocompetent hosts (CHD, CVD, cancer, frailty,…) Possibly trough an effect on immunosenescence Effect disappears in the oldest old Possibly through survivors effect Reverse epidemiology Thank you for your attention! Acknowledgements: - Jean-Marie Degryse - Cathy Matheï - Gijs Van Pottelbergh - Bert Vaes - Pierre Wallemacq