Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
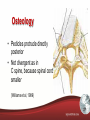
Brian Schlattmann, PT, DPT, OCS, CSMT, CSCS 1 2 The “New” Model Stabilization Directional Preference Manipulation Traction Red Flags Yellow Flags 3 Prevalence of C-spine disorders Neck pain in Hong Kong: a telephone survey on prevalence, consequences, and risk groups. The lifetime prevalence of neck pain was 65.4% The 12-month prevalence was 53.6% About 15.0% of these patients had moderate to severe pain. 65.4% The Saskatchewan Health and Back Pain Survey. The prevalence of neck pain and related disability in Saskatchewan adults. In Europe, the lifetime and point prevalence of neck pain is almost as high as the prevalence of low back pain. The age-standardized lifetime prevalence of neck pain is 66.7% The age-standardized 6-month prevalence of low-intensity and low-disability neck pain is 39.7% (95% confidence interval, 36.7-42.7), whereas it is 10.1% (95% confidence interval, 8.2-11.9) for high-intensity and low-disability neck pain and 4.6% (95% confidence interval, 3.3-5.8) for significantly disabling neck pain. 66.7% 4 C-Spine: At least a start… Neck Pain Idiopathic Whiplash 5 What about the Jurassic Spine? 6 Incidence of Thoracic Pain • 1-year prevalence for thoracic spine pain = 27% (Briggs et al, 2009) • Lifetime prevalence for thoracic spine pain = 31% (Briggs et al, 2009) Evidence Based Medicine • “The conscientious, explicit and judicious use of current best evidence in making decisions about the care of the individual patients.” – Sackett (1996) 8 Evidence Based Medicine Quantitative Research Qualitative Research Randomized Controlled Trials Human Experience Procedure/ Education/ Intervention Interaction Stolen from Mark Jones, IFOMT, 2004 9 What do patients want? • • • • • What is wrong with me? How long will it take? What can I (the patient) do? What can you (the PT) do? How much will it cost? Bud Light 2013 10 Clinical reasoning is the application of relevant knowledge (information, procedures, concepts) and clinical skills to patient management on an individual level. - Mark Jones, 1992 11 12 13 Permeable Brick wall Anatomy Physiology Biomechanics Pain Science Psychology From: Maitland 1992 History Signs Symptoms 14 The Role of the Physician 15 Collecting data: Questioning and Examining the Patient Maitland GD. Vertebral Manipulation. 6th ed. London: Butterworths; 1986. Interpret the Data Reach a Decision based on the Interpretation Treatment Assess the treatment and it’s effect Precautions Boissonnault WG, ed Examination in Physical Therapy Diagnosis. 2nd ed. New York: Churchill Livingstone; 1995. Clinical Anatomy of the Thoracic Spine Thoracic Spine • Challenging to treat, most neglected • Disorders thought to be less common • Less than 15% of all spinal disorders Thoracic Spine • Transitional zone between C and L spines • Second least mobile of the spinal regions (pelvic girdle) • Ribcage and low ratio of IVD height to vertebral body height (1:5) said to account for mobility (DiGiovanna and Schiowitz, 1991) Osteology T6 Vertebra • AP and transverse dimensions almost equal • Height of body is slightly higher posteriorly – contributes to normal kyphosis • Each body has paired costal demi-facets posterolaterally (↑↓) except T10, 11 & 12 Osteology • Pedicles protrude directly posterior • Not divergent as in C spine, because spinal cord smaller (Williams et al, 1989) Osteology • Laminae are higher than wide and overlap ‘like tiles on a roof’ • Limits extension Osteology T12 Vertebra • Superior facet slightly convex and posteriorly oriented 60º from horizontal plane and 20º from frontal plane • Inferior facet slightly concave and face anteriorly, slightly inferiorly and medially to match superior facets of vertebra below Osteology • Transverse processes project laterally and slightly posteriorly • Spread laterally diminishes from T1 to T12 – where they resemble those of L1 Osteology • Spinous processes project posteriorly and inferiorly to varying degrees (“rules of threes”) Rule of ‘threes’ Vertebra Spinous Process Level* T1 – T3 Same level T4 – T6 Half a level below T7 – T9 One whole level below T10 One whole level below T11 Half a level below T12 Same level Sternum Ribs Ribs Lateral costotransverse ligament Ribs • True/False Ribs – 1-7 True ribs, i.e. attach directly to the sternum – 8-12 False ribs, no direct sternal attachment • 11-12 are ‘floating ribs” • Typical/Atypical Ribs – 3-9 are Typical • Head attaches costovertebral demifacets on the body • Two Articular facets, one above and one below • Crest on head of rib that attaches to the disc Typical/Atypical Cont’d • Typical Cont’d – Distal to head and neck is a tubercle with articular and non-articular portions • Articular portion is more medial, attaches to for the costotransverse joint • Non-articular portion is more lateral, costotranverse ligament attachment – Rib angle Typical/Atypical Cont’d • Atypical – 1st rib • Most curved of all ribs • No angle • Only one joint surface for costovertebral facet at T1 – 2nd rib • Atypical due to attachment at junction of munibrium and body of sternum – 10th rib • Single costal facet attachment to T10 – 11th and 12th ribs • No direct sternal attachment Arthrology Ratio disc: body height is 1:5 compared to 2:5 in C spine and 1:3 in L spine Some report annulus is stronger and this helps T Spine resist rotational stress Thoracic Disc • Wood et al (1993) conducted T Spine MRI evaluations on 90 asymptomatic subjects • 68% had abnormalities • 24% had frank disc herniation FRANK • 42% had bulging discs • 46% had annular tears Facet Joint Structure Costovertebral Joint Structure Costotransverse Joint Structure • Upper joints are convex/ concave • Lower joints are planar • Said to account for ‘spin’ (rotation) of ribs within upper T spine, and ‘slide’ (elevation/ depression) of ribs within lower T spine Costochondral Junction • Costal cartilage fits into depression in distal end of each rib • Secured by enveloping periosteum which is continuous with perichondrium Costochondral Junction • Can be site of primary sprains or irritations (costochondritis) or secondary pain caused by rib cage dysfunction Ligaments of the T Spine • “Continuous ligamentous stocking” in which the vertebrae and ribs are positioned (Willard, 1997) Neural Arch Ligaments • • • • Ligamentum flavum Interspinous ligament Supraspinous ligament Intertransverse ligament Grade together at their boundaries to unite and function as a single unit Capsular Ligaments • Represents a bridge between neural arch ligaments and those of the vertebral body • Capsule reinforced dorsally by multifidus and ventrally by ligamentum flavum Ventral (Vertebral Body) Ligaments • ALL • PLL Myology • In the patient with T spine pain we should consider the large muscles of the spine and shoulder girdle as possible sources • We often resort to palpation for muscle spasm and check for imbalances • Don’t forget the many small muscles intimately associated with landmarks such as the rib angles, transverse processes and costovertebral joints Myology Deep ↓ Superficial Myology Intertransversarii Levatores costarum Myology Rotatores Thoracis Myology Myology Myology Myology Biomechanics of the Thoracic Spine The biomechanics of the Thorax is complex. We will slow it down for you… Biomechanics • • • Studies have concentrated on specimens without an intact rib cage Andriacchi et al (1974) studied effect of rib cage on T spine and found that the rib cage (with sternum) increased stiffness 2.64 times in E and 2.14 in F (No sternum = no ribs) Load bearing capacity of T spine was up to 3 to 4 times greater with addition of rib cage Biomechanics • • R-handed orthogonal (90º angle) coordinate system Motion in 3 translations and 3 rotations about the X, Y and Z axes Flexion Flexion Rib Kinematics Forward motion through superior demifacet of costovertebral joint. Facilitates anterior rotation of rib. Superior glide of costotransverse joint. Extension Extension Rib Kinematics Backward motion through superior demifacet of costovertebral joint. Facilitates posterior rotation of rib. Inferior glide of costotransverse joint. Lateral Flexion Lateral Flexion Lateral Flexion • Ribs on ipsilateral side approximate before joint motion is completed • As transverse process ipsilateral to the side bending attempts further motion in an inferior direction, the rib facet is forced superiorly • Creates an anterior rotation moment at the rib and forces superior vertebrae forward at the costovertebral joint • The ribs distract on contralateral side • Reach their passive restraints, are forced inferiorly at costotranverse joint as transverse process continues superior • Posterior rotation moment created and posterior rotating rib head forces the superior vertebrae back at the costovertebral joint Lateral Flexion Rotation Coupling of rotation with contralateral translation (X) and ipsilateral lateral flexion (Z) – clinical findings Rotation • Thus in R rotation the L translation of the vertebrae above pulls the R rib with it and push the L away • This causes costovertebral and costotransverse ligaments to become taught anterior on the R and posterior on the L • The segment is therefore forced into same side lateral bending Rotation Clinical Considerations 3 distinct regions 1. Upper T Spine (T1 – T2) – functions as part of lower C Spine 2. Lower T Spine (T10 – T12) – functions as part of upper L Spine 3. Functional T Spine (T3 – T9) – ‘true’ T Spine Need some coffee? Biomechanics • Dividing the T Spine into functional regions consistent with patterns of clinical presentation of mechanical disorders. 2 common patterns of clinical presentation: 1. Pain from loading – load attenuation 2. Symptoms related to movement/ motion restrictions Loading/ Load Attenuation • Compressive loads on T spine increase caudally from 9% body weight at T1 to 47% body weight at T12 (White, 1989) T6 Vertebra • Design to handle increasing load demand by progressive increase in: – Vertebral body height – End plate cross sectional area – Bone content (esp. last 6 segments) T12 Vertebra Load/ Load Attenuation • Upper T spine – 76% compressive load transferred through vertebral body/ disc complex. • Lower T spine – greater load transferred through posterior column via interlocking lamina and facet joints. (Pal and Routal, 1987) Load/ Load Attenuation IVD • Thinner than C spine and L spine discs • Some reports that annulus fibrosis is stronger – greater ability to resist rotational stress • Evidence that disc lesions more evident – MRI studies – 73% of asymptomatic population had some form of disc lesion Load/ Load Attenuation • Upper and mid-thoracic discs undergo greater deformation and creep • More viscous mechanical behavior not because of water content • Due to morphology, biochemistry and structural arrangement of annular lamellae Load/ Load Attenuation • In L Spine – compressive loading evenly distributed across surface of end plate independent of position of motion segment • In T Spine – load distribution across the end plate becomes asymmetric when loaded outside the neutral position – May explain common clinical finding of mid-thoracic pain associated with sustained loading postures, e.g. computers, driving Movement/ Motion Restrictions • Upper T spine mobility contributes to normal C spine function and to functional movements of the thorax. • Restricted mobility in upper T spine can affect C spine motion, as well as overall motion of thorax. Clinical Considerations of Motion Restriction • Normal mechanics/ motion of C spine and shoulder dependent upon normal mobility of upper T spine • Habitually flexed upper T spine may reduce capacity of muscles to provide cervicothoracic retraction to work in the functional range Clinical Considerations of Motion Restriction Clinical Considerations of Motion Restriction • Palpation for intersegmental accessory joint motion – mainstay of Maitland Approach • Changes in through-range resistance to movement (stiffness) with PA can help identify symptomatic segment • Pain response to PA shown to be more reliable in detecting symptomatic segments than stiffness alone – don’t underestimate palpation skills • Edmondston et al (1999) found that PA stiffness of T spine segments ↑ from 9.1 N/mm at T4 to 11.4 N/mm at T10 • Departure from this segmental increase in PA stiffness could indicate abnormal motion segment function if assoc w/ relevant symptom response PA to the T Spine • When applying a PA to the T spine, care should be taken with orientation of applied force • PA to spinous process induces anterior translation and posterior rotation (extension) of the related vertebral segment PA to the T Spine • Lee (1989) – movement force (PA) of 200 N applied perpendicular to spinal curvature causes anterior translation of equivalent force at vertebral segment but it is also accompanied by extension moment of up to 5.5 Nm • In contrast, equivalent force directed towards vertebral body eliminates extension moment but induces a longitudinal force of up to half the applied load PA to the T Spine Applied anteriorly PA to the T Spine Applied to spinal curvature PA to the T Spine Applied towards center of vertebral body Dinner last night… 88 Thoracic Spine Pathology 89 Thoracic Injury 90 Injury to T Spine classified as: • • • • • Gradual arthritic disorders Postural Acute, traumatic Referral from C spine Visceral in origin 91 Pathology • Greatest % of pts presenting w/ T Spine symptoms will have been involved in a trivial accident – fall, bump or accident • T Spine well supported with ribcage but it doesn’t need strong force applied to strain ZPJ or costochondral joint 92 Pathology • Musculoskeletal disorders common with pain referral in/ around chest wall • Differential diagnosis of visceral disorders essential • Study – 25% of ‘cardiac’ pts in ER had T Spine disorder (other studies 11 – 16%) • Confusion when breathing, coughing or posture alteration aggravates pain 93 T Disc Lesions • Much more common that previously thought but still less than in L Spine • Attachment of ribs to annulus fibers may be one reason for higher incidence - blow to rib may affect/ disrupt the IVD • Other reasons: - higher viscosity of IVD in T Spine - asymmetrical loading associated with segmental motion 94 T Disc Lesions • Most affected – lower T Spine; most often – T/L junction • Disc lesions common on convex side of a scoliosis or kyphosis 95 T-Spine Disc Lesions • Lower T Spine refers to abdomen and iliac crests 96 97 Thoracic Nerve Root Lesions • Nerve root pain either mechanical compression or chemical irritation • May occur due to disc lesions, facet injuries/swelling, osteophytes, scarring, etc. • In true nerve root pain, distal pain (anterior, next to sternum) will be greater than proximal pain (back) • Neurological symptoms (numbness, P & N) may be present if compression only 98 Thoracic Nerve Root Lesions • Costochondritis may closely simulate T-nerve root symptoms b/c pain located anteriorly at sternum • Upper T spine will refer symptoms into upper extremities • Spinal dura can produce vague symptoms up and down the spine – least mobile at T6 and is common source of pain in pts w/ + neurodynamic signs 99 Facet Joint Dysfunction • Commonly injured – seat belts in MVA • Usually produce localized sharp pain unilaterally • In chronic stage – pain may be dull, aching • Pain more likely to be aggravated by compressing/ closing down facet joint 100 Facet Joint Dysfunction • Pain may be referred into nerve root distribution but no neuro symptoms • Referred pain will be more intense proximally (back) vs. distally (sternum) • Acutely swollen/ damaged joints – pain with coughing, sneezing or deep breathing 101 Ligamentous Injuries • Pain in T Spine can be from highly ligamentous reinforced joints • Any force applied to ribcage can affect ligaments which not only stabilize joints but play important role in proprioception 102 Ligamentous Injuries • Pain from ligamentous structures commonly described as vague, ill defined, spread around the area, not producing symptoms distally nor producing neuro symptoms • Both ALL and PLL innervated by SVN and will cause pain that spreads up and down spinal canal 103 Rib Cage Injuries • Rib injuries common • Force applied to ribcage dissipated by ribs • Rib fractures may be present in severe traumatic injuries – usually very painful • Breathing may increase pain • Area very tender to palpation 104 Rib Cage Injuries • In acute injuries – hematoma may be present – tap test with reflex hammer or vibration with tuning fork will produce pain • Old, chronic, slow healing rib fractures may become a chronic source of discomfort 105 Muscle Injuries • True muscle injuries of the spine are very uncommon, yet often the focus of physical therapy intervention. • The musculoskeletal system does, however, get affected through joint injuries and postural changes. • Muscle spasms and especially trigger points are very common in the upper thoracic spine, especially the muscles surrounding the scapula. • In assessing trigger points be sure to assess the posterior primary rami from the nervous system - a possible source/ mechanism for maintained pain/ tender spots in TP areas. 106 Trigger Points 107 Thoracic Outlet Syndrome Subclavian artery vs. Brachial plexus 108 TOS • Vascular: Rare – 1.5% of TOS patients – Hard to treat conservatively 109 TOS: Neurogenic • 98.5% of TOS patients • Responds to conservative care • True neurogenic TOS: axonal compression – – – – – hand weakness muscle wasting cervical rib positive EMG for axon loss special tests: Adson’s test (Plewa and Delinger 1998) 110 TOS Common clinical presentation of all TOS patients • Numbness/tingling in the ring and small fingers but can encompass the entire hand • Paresthesias occur at night and/or during daily activities • Vague pain in the involved extremity • (Can occur in the hand, elbow, shoulder and/or cervical spine) • Subjective complaints of hand/arm weakness especially with arm raised overhead • Subjective complaints of swelling in the arm in the absence of true swelling 111 T4 Syndrome • Well described in clinical field by Maitland • Precise etiology is unknown • May be an autonomic syndrome or mechanical problem involving ZPJs • Sometimes referred to as “glove-syndrome” because of dull aching symptoms covering whole hand (non dermatome) and +/- neuro symptoms (P & N) • Symptoms usually unilateral 112 T4 Syndrome 113 Thoracic Hypomobility • Very common • Sudden onset of symptoms • Can be severe at times • Often aggravated by movements – breathing, coughing and sneezing 114 Thoracic Hypomobility • Localized posteriorly slightly off midline towards one side (suggesting CT joint) • One side – radiates slightly a few inches • Chest wall pain common • Costochondral region • Low back pain – T/L junction • Great response to mobs + manips • Marked relief in few sessions • Need exercises for prevention 115 MRI Thoracic Fractures 116 Vertebroplasty vs. Kyphoplasty PMMA 117 Kyphoplasty 118 Vertebroplasty vs. Kyphoplasty 119 Kyphoplasty and PT • Thirty-eight patients (10 men and 28 women) were treated for 47 levels initially. • L1 and L2 were the most common level of fracture. • Over the follow-up period (average, 8 months), 10 patients sustained 17 subsequent fractures. • Eight patients sustained fractures in the first 2 months after the index procedure, all with at least one fracture at an adjacent level. • Of the 17 subsequent fractures, there were nine at the adjacentabove levels, four at adjacent-below levels, and four at remote levels. Incidence of Subsequent Vertebral Fracture after Kyphoplasty. Spine. 29(20):2270- 2276, October 15, 2004. 120 Kyphoplasty & PT 121 Referral from the C-spine 122 123 124 C-Facet Joints • • • • Synovial Ceiling tile setting Vascularized ++ Nerve supply 125 C-Facet - Car accident - Fracture of superior articular process - Missed on x-ray 126 C-Facet: Crush injury MVA 127 C-Facet Ligamentum flavum bruise: MVA 128 C-Facet Pain referrals 129 There is growing evidence that trigger points (TP’s) are in fact an epi-phenomenon, and rather than being the originator of the pain, they are more a consequence of the damaged tissue. (Cohen 1996, Wall 1993) 130 131