Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
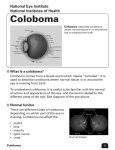
Problem oriented medical diagnosis Savita Bhat MS, DO (CMC Vellore) DNB ,MNAMS Optic Discs Mimicking Glaucoma T raditionally the diagnosis of primary open angle glaucoma (POAG) is a triad of increased intraocular pressures, characteristic optic nerve head (ONH) changes and corresponding visual field changes. Recent definition of glaucoma excludes intraocular pressure as a defining factor (1).The diagnosis of glaucoma depends on functional psychological tests and imaging technology of ONH morphology. Structural changes precedes that of functional changes. Despite the advent of new technology to assess ONH changes with Heidelberg Retinal Tomogram (HRT), Scanning Laser Ophthalmoscope (SLO) and Optical Coherence Tomography (OCT) available for research, clinical acumen in detecting glaucomatous features of ONH is imperative in routine clinical practice. Very often in our busy outpatient practice , large disc associated with large cup and similar lesions are over diagnosed and labeled as “glaucoma”. It is therefore imperative to differentiate glaucoma from non glaucomatous disc anomaly. Several conditions pose as ONH mimickers and these lesions often reiterates the need of careful clinical examination of ONH.(2,3). We present a series of three such cases. Fig. 2 However, the fields remained stable on the following visits. Fields in 2003 showed no progression (Fig.3). Case-I A 40 -year old male presented with complaints of defective vision for distance. On examination, best corrected visual acuity in both eyes was 6/9 N6. Right eye - -9.00 Dsph and left eye -8.00/-1.00 Dcyl x 90º. Applanation tonometry in the right eye and left eye was 20mmHg and 23mmHg respectively. Extra ocular movements, pupil and anterior segment was within normal limits. Fundus picture showed tilted optic disc with prominent inferonasal margin as in Fig.1. Fig. 3 The diagnosis of congenital optic disc syndrome was made. Points to remember regarding congenital tilted disc syndrome are as follows: ♦ Bilateral ♦ Situs inversus of retinal vessels ♦ Inferior or inferonasal crescent or conus -Fuch’s coloboma Fig. 1 ♦ Prominence of inferonasal fundus ♦ Posterior inferonasal Staphyloma 6-9 diopters Visual field examination done in 2002 showed corresponding arcuate defects emanating at the disc and enlarging beyond it as seen typically in glaucoma (Fig.2). ♦ Refractive error – astigmatism/myopia ♦ Field defects refraction scotoma or bi-temporal hemianopia which may need neuro imaging. (4,5) 117 Address for correspondence- [email protected], Giridhar Eye Institute, Kadavanthra, Kochi Vol. XXIV, No.2, Jun. 2012 Kerala Journal of Ophthalmology Case-II Case-III. A 52 year old male presented with complaints of eye strain in 2005. On examination, his unaided visual was 6/6 in both eyes and near vision was N6. Extra ocular movements, pupil and anterior segment were within normal limits. Applanation tonometry in both eyes was 14mmHg. The diurnal variation of tension in the right eye was 12-18 mmHg and left eye was 12-16mmHg. Fig(4) shows abrupt absence of normal optic disc structure with inferior disc pallor and corresponding wedge shaped nerve fiber layer defect better seen in red free photograph . A 48 -year old man came for a routine ophthalmic evaluation for renewal of driving license. On examination, best corrected visual acuity was 6/6 N6. Extra ocular movements, pupil and anterior segment were normal. Applanation tonometry in both eyes was 12mmHg. Fundus picture in Fig (7) shows a typical double disc sign with bridge of retinal tissue called bridge coloboma and shows an abrupt absence of normal optic disc feature. Fig. 7 Fig. 4 The fields in Fig(5) shows characteristic superior defect which remained the same and did not progress (Fig.6) as in a typical glaucoma. Note the large size of optic discs in both eyes with normal structure of superior discs. Also, left eye has an optic nerve pit. Fields in Fig.(8) in the right eye showed enlargement blind spot and left eye shows typical superior arcuate scotoma. Fig. 8 Fig. 5 Red free photograph of left eye confirms inferior NFL defect in this area. (Fig.9) Fig. 6 This patient was diagnosed to have optic nerve coloboma. 118 Fig. 9 Savita Bhat - Optic Discs Mimicking Glaucoma Case II and III are different spectrum of ONH coloboma. Case III left eye also had ONH pit. The characteristic features of optic disc coloboma are: ♦ PAX 2 gene mutation ♦ Visual acuity affected with involvement of papillomacular bundle ♦ Common in females , as hemiaminopia with associated trans sphenoidal basal encephocele, mid facial anomalies and clefting syndrome ♦ Retinal detachment ♦ Sub-retinal choroidal neovascular membrane. The systemic conditions associated with colobomas are♦ Charge Syndrome (coloboma, heart defect, atresia choanae, mental retardation, genito urinary abnormalities, ear defects) ♦ Goltz syndrome ♦ Lenz microphthalmia syndrome ♦ Meckel – Gruber syndrome ♦ Walker Warburg syndrome. ♦ Goldenhar’s syndrome Optic disc coloboma is classified as an excavated optic disc anomaly which are as follows: ♦ Morning glory disc anomaly ♦ Optic disc coloboma ♦ Peripapillary Staphyloma The features of Morning glory syndrome are: Figure 10 shows disc coloboma ,iris and choroidal coloboma Morning glory disc is akin to the flower of the same name in Figure11.Also seen are the straight course of vessels in the angiogram. ♦ Non closure of fetal fissure ♦ Bowl shaped excavation occupying a large disc ♦ Excavation decentered inferiorly ♦ Inferior neuro retinal rim is thin or absent ♦ No glial tissue ♦ Normal peripapillary retinal blood vessels ♦ Familial and bilateral ♦ Serous macular detachment is common ♦ Iris, ciliary and retinal coloboma are associated Figure11 119 Vol. XXIV, No.2, Jun. 2012 Kerala Journal of Ophthalmology The ophthalmic differences between morning glory disc and peripapillary coloboma are - . Peripapillary staphyloma is usually unilateral with deep fundus excavation surrounding the disc. There are posterior scleral defects. The normal cup is placed within an atrophic area,. There is no glial tissue. Pigmentary changes are present. Retinal vessels are normal. Vision is normal but slightly myopic. Scotoma or enlarged blind spots may be present. No systemic association. Ophthalmic differences between peripapillary Staphyloma and morning glory disc. OPTIC DISC PITS Figure11 ♦ Congenital large funnel shaped excavation of posterior fundus which involves the disc ♦ Central tuft of glial tissue ♦ Significantly increase in number in one minute from the edge of the disc and run straight ♦ Peripapillary pigmentary disturbances ♦ Macular capture ♦ Difficulty in differentiating (Figure 11) arteriole from venules Optic disc pits are found in 1 in 10,000 cases. They are unilateral and affected disc is larger in size. The pit is present in the temporal part of the disc and often the disc has a cilioretinal artery. 25 -75 % of eyes are associated with serous macular detachment and called Kranenberg’s syndrome. Paracentral arcuate scotoma with enlarged blind spot are common and field defects poorly correlate with location of pit. Pathogenesis is uncertain and has no systemic association. Therefore, different optic disc anomalies should be considered before diagnosing glaucoma in routine practice. The common optic disc anomalies mimicking glaucoma are ♦ Normal variants include a congenital deep cup, large physiological cup, myopic disc ♦ congenital tilted disc. ♦ Morning glory syndrome ♦ Optic disc coloboma, ♦ peripapillary Staphyloma, ♦ Unilateral ♦ Visual acuity 6/6 or no PL ♦ optic disc pit. Table 1 gives ophthalmic differences between Morning glory disc and optic disc coloboma. MORNING GLORY OPTIC COLOBOMA MORNING GLORY DISCDISC OPTIC DISCDISC COLOBOMA discwithin lies within the excavation Excavation lies within the disc OpticOptic disc lies the excavation Excavation lies within the disc Symmetrical defect Asymmetrical defect Symmetrical defect Asymmetrical defect lies within the excavation)(Excavation (Excavation lies inferiorly (Disc(Disc lies within the excavation) lies inferiorly withinwithin the disc) the disc) Central glial tuft No tuft glial tuft Central glial tuft No glial Severe peripapillary pigmentary Minimal Minimal peripapillary pigmentary Severe peripapillary pigmentary peripapillary pigmentary disturbances disturbances disturbances disturbances Anamolous retinal vasculature Normal Normal retinal vasculature Anamolous retinal vasculature retinal vasculature 120 Peripapillary staphyloma is usually unilateral with deep fundus excavation Peripapillary staphyloma is usually unilateral with deep fundus excavation surrounding the disc. are posterior scleral defects. The normal surrounding the disc. ThereThere are posterior scleral defects. The normal cup iscup is placed an atrophic no glial tissue. Pigmentary placed withinwithin an atrophic area,.area,. ThereThere is nois glial tissue. Pigmentary changes are present. Retinal vessels are normal. Vision is normal changes are present. Retinal vessels are normal. Vision is normal but but systemic association. Ophthalmic differences between peripapillary Staphyloma and morning glory disc. Savita Bhat - Optic Discs Mimicking Glaucoma Table 2 enlists ocular and systemic differences between morning glory discTable and opticocular disc 2 enlists andcoloboma. systemic differences between morning glory disc and optic disc coloboma. Optic disc pits are found cases.DISC TheyCOLOBOMA are unilateral and MORNING GLORY DISCin 1 in 10,000 OPTIC More common females, rareThe in pit No sex or racial affected disc isin larger in size. is present in the predilection temporal part of black the disc and often the disc has a cilioretinal artery. 25 -75 % of eyes are Rarely familial Often familial associated with serous macular detachment and called Kranenberg’s Rarely bilateral Often bilateral syndrome. Paracentral arcuate scotoma with enlarged blind spot are Not associated with iris,ciliary and Iris, ciliary and choroidal common and field defects poorly correlate with location of pit. choroidal colobomas colobomas common Pathogenesis is uncertain and has noOften systemic association. Rarely associated with multisystem associated with multisystem genetic disorders genetic disorders Basal encepholocele common Basal encepholocele rare Table 3 enumerates differences between peripapillary staphyloma and morning syndrome. Table 3glory enumerates differences between peripapillary staphyloma and morning glory syndrome. OPTIC DISC PITS PERIPAPILLARY STAPHYLOMA Deep cup shaped excavation Relatively normal, well-defined optic disc Absence of glial and vascular anomalies Embryological : fifth month Defect in posterior sclera MORNING GLORY DISC Less depth funnel shaped excavation Grossly anomalous poorly –defined optic disc Central glial bouquet of vascular anamolies Embryological : four weeks Defect in distal optic stalk Therefore, Table different optic disc anomalies should be considered before 4 enlists the difference in glaucomatous and non glaucomatous features of ONH diagnosing glaucoma in routine practice. The common optic disc anomalies Non glaucomatous mimicking glaucoma are Glaucomatous Age Usually elderly Younger age group congenital Normal variants include a congenital deep cup,with large physiological anamoloies cup, myopic disc Laterality May be unilateral or congenital tilted disc. Primary glaucomas are bilateral bilateral Morning glory syndrome Presentation Incidental or on Optic disc coloboma, Asymptomatic evaluation of peripapillary Staphyloma, headache optic disc pit. Visual acuity Good until late stage Poor if papillomacular of disease bundle involved Table 4 enlists the difference in glaucomatous and non glaucomatous Colour vision Correlates with acuity Correlates with features of ONH and maintained until involvement and end stage disease extent of the lesion Optic disc features Normal to small size Usually large sized Focal or uniform Unaffected part of the affliction of glaucoma disc appears healthy Palllor proportionate Pallor out of to the cup proportion to the cup 121 of disease bundle involved headache headache Correlates with acuityPoor Correlates with Good Good until untillate late stage stage Poor if ifpapillomacular papillomacular and maintained until bundle involvement and ofofdisease disease bundle involved involved end stage disease extent ofwith the Colour Colourvision vision Correlates Correlates with with acuity acuity Correlates Correlates withlesion disc features and Normal to small size involvement Usually large sized and maintained maintained until until involvement and and Kerala Journal Optic of Ophthalmology Vol. XXIV, No.2, Jun. 2012 end end stage stage disease extent extent ofofthe thelesion lesion Focal ordisease uniform Unaffected part of the affliction of glaucoma disc appears healthy Optic Opticdisc discfeatures features Normal Normal totosmall small size size Usually Usually large largesized sized Palllor proportionate Pallor outpart of ofofthe Focal Focal ororuniform uniform Unaffected Unaffected part the to the of cup proportion tohealthy the cup affliction affliction ofglaucoma glaucoma disc disc appears appearshealthy Field defects Nasal step, arcuate Pallor Central ,of cecocentral Palllor Palllor proportionate proportionate Pallor out outof scotoma hemianopia orcup totothe thecup cup proportion proportion totothe the cup arcuate scotoma Field Fielddefects defects Nasal Nasalstep, step,arcuate arcuate Central Central, ,cecocentral cecocentral Progression Invariably progresseshemianopia Will not proress scotoma scotoma hemianopia oror arcuate arcuate scotoma scotoma Systemic Absent May be present esp associations with Progression Progression Invariably Invariablyprogresses progresses Will Will not notcongenital proress proress anomalies Systemic Systemic Absent Absent May May be bepresent presentesp esp Family history May be present Absent associations associations with with congenital congenital anomalies anomalies Family Familyhistory history May Maybe bepresent present Absent Absent Colour vision Visual Visual acuity acuity References: References: 3. Kim M.R., Park S.E., OhSY . Clinical features analysis of congenital optic nerve abnormalities. Jpn.J O Ophthalmol 50;definition 250-5 Johnson GJ.2006, The and 1. Foster PJ, Buhrmann R, Quigley HA, Johnson GJ. 1.Foster PJ, Buhrmann R, Quigley HA, References: TheReferences: definition and classification of glaucoma in classification of glaucoma in prevalence4.surveys. BrCongenital J Ophthalmol Brodsky MC. Optic Disc Anomalies. Surv of prevalence surveys. Br J Ophthalmol 2002;86:238-42. 1.Foster 1.Foster PJ, PJ, Buhrmann Buhrmann R, R, Quigley Quigley HA, HA, Johnson Johnson GJ. GJ. The The definition definition and and Ophthalmol 1994, 39(2):89-112. 2002;86:238-42. 2. Hodgkins P, Lees M, Lawson J et al, Optic disc classification classification ofofglaucoma glaucoma inprevalence prevalencesurveys. surveys. J JalOphthalmol Ophthalmol 5. Apple Br DJBr et .Congenital anomalies of the optic disc. anomalies and frontonasal dysplasia in Br.JOphthalmol 2. Hodgkins P, Lees M, Lawson J et al, Optic disc anomalies and3-41. Surv of Ophthalmol 1982, 27(1): 1998, 82:290-3. 2002;86:238-42. 2002;86:238-42. frontonasal dysplasia Br.J Ophthalmol 1998, 82:290-3. 2.2.Hodgkins HodgkinsP,P,Lees LeesM, M,Lawson LawsonJ Jetetal, al,Optic Opticdisc discanomalies anomaliesand and frontonasal frontonasaldysplasia dysplasiaBr.J Br.JOphthalmol Ophthalmol1998, 1998,82:290-3. 82:290-3. Dr Savita Bhat after her DO,MS, DNB and initial training at CMC Vellore is senior consultant at Giridhar Eye Institute, Kochi 122