Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
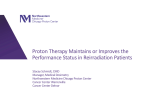
VOLUME 29 䡠 NUMBER 36 䡠 DECEMBER 20 2011 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Evaluating Survivorship Care Plans: Results of a Randomized, Clinical Trial of Patients With Breast Cancer Eva Grunfeld, Jim A. Julian, Gregory Pond, Elizabeth Maunsell, Douglas Coyle, Amy Folkes, Anil A. Joy, Louise Provencher, Daniel Rayson, Dorianne E. Rheaume, Geoffrey A. Porter, Lawrence F. Paszat, Kathleen I. Pritchard, André Robidoux, Sally Smith, Jonathan Sussman, Susan Dent, Jeffrey Sisler, Jennifer Wiernikowski, and Mark N. Levine See accompanying editorial on page 4740 Author affiliations appear at the end of this article. Submitted May 5, 2011; accepted August 18, 2011; published online ahead of print at www.jco.org on October 31, 2011. Supported by grant No. 17423 from the Canadian Breast Cancer Research Alliance, and by a clinician scientist award from the Ontario Institute for Cancer Research with funds from the Ontario Ministry of Research and Innovation (E.G.). Presented in part at the 47th Annual Meeting of the American Society of Clinical Oncology, June 3-7, 2011, Chicago, IL. Authors’ disclosures of potential conflicts of interest and author contributions are found at the end of this article. Clinical Trials repository link available on JCO.org. Corresponding author: Eva Grunfeld, MD, DPhil, FCFP, Ontario Institute for Cancer Research and Department of Family and Community Medicine, University of Toronto, 500 University Avenue, Room 352, Toronto, Ontario M5G 1V7, Canada; e-mail: eva [email protected]. © 2011 by American Society of Clinical Oncology A B S T A C T Purpose An Institute of Medicine report recommends that patients with cancer receive a survivorship care plan (SCP). The trial objective was to determine if an SCP for breast cancer survivors improves patient-reported outcomes. Patients and Methods Women with early-stage breast cancer who completed primary treatment at least 3 months previously were eligible. Consenting patients were allocated within two strata: less than 24 months and ⱖ 24 months since diagnosis. All patients were transferred to their own primary care physician (PCP) for follow-up. In addition to a discharge visit, the intervention group received an SCP, which was reviewed during a 30-minute educational session with a nurse, and their PCP received the SCP and guideline on follow-up. The primary outcome was cancer-related distress at 12 months, assessed by the Impact of Event Scale (IES). Secondary outcomes included quality of life, patient satisfaction, continuity/coordination of care, and health service measures. Results Overall, 408 survivors were enrolled through nine tertiary cancer centers. There were no differences between groups on cancer-related distress or on any of the patient-reported secondary outcomes, and there were no differences when the two strata were analyzed separately. More patients in the intervention than control group correctly identify their PCP as primarily responsible for follow-up (98.7% v 89.1%; difference, 9.6%; 95% CI, 3.9 to 15.9; P ⫽ .005). Conclusion The results do not support the hypothesis that SCPs are beneficial for improving patient-reported outcomes. Transferring follow-up to PCPs is considered an important strategy to meet the demand for scarce oncology resources. SCPs were no better than a standard discharge visit with the oncologist to facilitate transfer. J Clin Oncol 29:4755-4762. © 2011 by American Society of Clinical Oncology INTRODUCTION 0732-183X/11/2936-4755/$20.00 DOI: 10.1200/JCO.2011.36.8373 R The prevalence of cancer survivors is increasing worldwide as a result of the growth and aging of the population and improved survival through earlier diagnosis from screening and improved treatments. It is estimated that there are approximately 22.4 million survivors globally,1 and 11.7 million are in the United States, which represents approximately 4% of the US population.2 In 2006, the Institute of Medicine (IOM) published an influential report that described the heath care and health system needs of cancer survivors for “the period following first diagnosis and treatment and prior to the development of a recurrence of cancer or death.” 3(p23) The IOM report issued 10 recommendations; chief among them was the recommendation that patients completing primary treatment should be provided with a survivorship care plan (SCP), described as a “comprehensive care summary and follow-up plan” to be “written by the principal providers who coordinated oncology treatment.”3(p151) The key elements of SCPs are a personalized treatment summary, information on possible late and long-term effects, information on signs of recurrence,guidelinesforfollow-upcare,identification of providers, recommendations for healthy living, and identification of supportive care resources.4 Because the growing number of cancer survivors has raised concern about the strain that © 2011 by American Society of Clinical Oncology Information downloaded from jco.ascopubs.org and provided by at ST LUCAS ANDREAS ZIEKENHUIS on September 24, Copyright © 2011 American Society Clinical Oncology. All rights reserved. 2014 fromof85.90.80.12 4755 Grunfeld et al providing long-term routine follow-up has put on specialist oncology resources,5 SCPs are also viewed as potentially valuable for facilitating transition from active treatment to survivorship and from specialist care to routine follow-up in primary care.5-7 Since publication of the IOM report, many organizations internationally have dedicated substantial resources to implementing SCPs.7-12 Although there is growing literature on SCPs generally, and although they are considered to have face validity,3 there has never been, to our knowledge, a rigorous evaluation of the benefits of SCPs on patient outcomes.13 Asagroupwithoneofthemostprevalentadultcancersthathasboth high incidence and greater than 80% long-term survival,14 breast cancer survivors are an important target population for receipt of SCPs.6 The objective of this randomized trial was to determine if an SCP for breast cancer survivors who are ready for transition from oncologist care to follow-up with their own primary care physician (PCP) improves patient-reported outcomes. We hypothesized that patientreported outcomes would be positively affected by an SCP up to 12 months after random assignment. PATIENTS AND METHODS Trial Patients Trial participants were women with early stage breast cancer who completed primary treatment at least 3 months previously, except for continued use of tamoxifen or an aromatase inhibitor, and who were without recurrent or new primary cancer. Patients were excluded if they were still experiencing complications of primary treatment, did not have a PCP to provide care, were previously enrolled on a study requiring oncology follow-up, were actively followed up for another primary cancer, or had a PCP who already had a patient enrolled on the trial (to avoid contamination). Exclusion criteria were minimal to maximize generalizability.15 Because survivors who have been in oncology follow-up longterm are less likely to accept transfer to the PCP and are more likely to experience anxiety,16,17 the effectiveness of the intervention was expected to be different for those who had been in oncology follow-up for a longer period. Therefore patients were randomly assigned within two strata: those diagnosed less than 24 months or diagnosed ⱖ 24 months earlier. All trial participants gave written informed consent. The trial was approved by the ethics committees of each participating center. Patients were enrolled between April 2007 and July 2009 and were followed up for 2 years. Design and Intervention We conducted a multicenter, randomized trial. Those collecting outcome data remained blinded to the treatment allocation group. The intervention was developed by using an implementation framework18 with input from oncologist, PCP, and patient perspectives to identify barriers and supports to transition from oncologist to routine follow-up in primary care. The intervention was developed to be practical and as consistent with usual practice as possible so as to be generalizable to both oncology and primary care settings. Assessed for eligibility (N = 1,109) Excluded Enrolled in another study Unable to comply with protocol On or candidate for Herceptin PCP already in study Other Approached Declined participation Randomly assigned (n = 408) Allocated to control No SCP group Strata: < 24 months ≥ 24 months (n = 208) n = 91) (n = 117) Transferred to PCP (n = 203) Recurrence (n = 1) Patient withdrawal (n = 1) Investigation of recurrence (n = 1) Patient moved (n = 1) Lost to follow-up (n = 1) Analyzed Completed questionnaires Baseline 3 months 6 months 12 months 4756 (n = 186)† (n = 207) (n = 169) (n = 164) (n = 153) © 2011 by American Society of Clinical Oncology Allocated to intervention SCP group (n = 200) Strata: < 24 months n = 89) ≥ 24 months (n = 111) (n = 191) Transferred to PCP (n = 3) Recurrence (n = 4) Patient withdrawal (n = 1) Investigation of recurrence (n = 1) Lost to follow-up Analyzed Completed questionnaires Baseline 3 months 6 months 12 months (n = 472) (n = 217) (n = 70) (n = 57) (n = 49) (n = 83)* (n = 637) (n = 229) Fig 1. Trial flow diagram. (*) Details of other reasons include the following: primary treatment, fewer than 3 months (n ⫽ 13); under investigation for recurrence (n ⫽ 20); no community-based primary care physician (PCP; n ⫽ 30); actively followed up for another cancer (n ⫽ 20). Four patients met two exclusion criteria: primary treatment for fewer than 3 months and previously enrolled on other study (n ⫽ 1), and previously enrolled on other study and actively followed up for another cancer (n ⫽ 3). (†) Transferred to PCP and completed at least one postbaseline questionnaire. SCP, survivorship care plan. (n = 170)† (n = 200) (n = 163) (n = 154) (n = 146) JOURNAL OF CLINICAL ONCOLOGY Information downloaded from jco.ascopubs.org and provided by at ST LUCAS ANDREAS ZIEKENHUIS on September 24, Copyright © 2011 American Society Clinical Oncology. All rights reserved. 2014 fromof85.90.80.12 Evaluating Cancer Survivorship Care Plans Table 1. Baseline Demographic and Clinical Characteristics by Trial Group Control: No Survivorship Care Plan (n ⫽ 208) Baseline Characteristic Age, years Mean SD Education Less than secondary Completed secondary Postsecondary Unknown Marital status Single Married/cohabiting Widow Separated/divorced Tumor grade 1 2 3 Unknown Tumor size, cm 0 to 1.9 2 to 4.9 ⱖ5 Unknown No.of positive nodes 0 1 to 3 ⱖ4 Unknown Type of surgery Mastectomy Breast-conserving surgery Type of treatment Radiation Chemotherapy Hormonal therapy Tamoxifen Aromatase inhibitor Time from diagnosis, monthsⴱ Stratum ⬍ 24 Median Range Stratum ⱖ 24 Median Range All patients Median Range Baseline patient-reported measure Cancer-specific distress: IES Intrusion Mean SD Avoidance Mean SD No. % No. Table 1. Baseline Demographic and Clinical Characteristics by Trial Group (continued) % Baseline Characteristic 61.7 10.2 13 57 109 29 6 27 52 14 19 54 103 24 10 27 52 12 29 130 21 28 14 63 10 14 19 142 18 20 10 71 9 10 49 76 64 19 24 37 31 9 42 82 57 19 21 41 29 10 116 73 11 8 56 35 5 4 124 59 8 9 62 30 4 5 143 43 20 2 69 21 10 1 133 49 17 1 67 25 9 1 56 152 27 73 57 143 29 72 171 89 154 108 67 82 43 74 52 32 162 86 135 109 52 81 43 68 55 26 11.2 3.5-23.8 12.4 3.6-29.2 80.1 3.7-300 82.3 11.8-375 35.3 3.5-300 35.3 3.6-375 8.1 7.3 8.4 7.9 10.7 18.0 12.0 10.2 Control: No Survivorship Care Plan (n ⫽ 208) Intervention: Survivorship Care Plan (n ⫽ 200) No. No. % % Total score 61.2 10.4 (continued in next column) www.jco.org Intervention: Survivorship Care Plan (n ⫽ 200) Mean 18.9 20.4 SD 14.5 16.3 Mean 49 49 SD 9 9 Mean 50 51 SD 11 9 Mean 75 76 SD 19 19 Health-related quality of life: SF-36 Physical component scale Mental component scale Patient satisfaction questionnaire Physician primarily responsible for follow-up† Primary care physician 68 33 67 34 Cancer physician 113 54 113 57 Cancer surgeon 36 17 30 15 Other 15 7 9 5 No response 10 5 7 4 Abbreviations: IES, Impact of Events Scale; SD, standard deviation; SF-36, short-form 36 of the health-related quality-of-life questionnaire. ⴱ Five patients were randomly assigned on the basis of incorrect stratification information. †Some patients indicated multiple providers. The control condition, which applied to patients both in control (ie, no SCP) and intervention (ie, SCP) groups, all routine follow-up care was transferred to the patient’s own PCP. All cancer specialists involved in the patient’s follow-up care (ie, surgical, radiation, and medical) agreed to the transfer so that all patients were under exclusive PCP follow-up. Patients had a standard discharge visit with the oncologist, and a discharge letter was sent to the PCP, which was consistent with usual practice. There was an instruction to PCPs to refer patients back to the oncologist if a recurrence or new primary cancer developed and an instruction both to patients and PCPs to schedule the first follow-up visit in approximately 3 months (all subsequent visits were arranged between the patient and PCP). In addition, patients were able to access any supportive care services available at the cancer center according to usual procedures. Patients in the intervention group additionally received a comprehensive SCP that consisted of the prescribed elements, including a personalized treatment summary,4 a patient version of the Canadian national follow-up guideline,19 a summary table of the guideline that served as a reminder system, and a resource kit tailored to the patient’s needs on available supportive care resources. These documents were compiled in a binder and were reviewed with the patient during a 30-minute educational session with a nurse, who also made an explicit statement that follow-up care was now the responsibility of the PCP and that access to the oncologist was available when needed. These documents were also sent to the patient’s PCP together with the full follow-up guideline,20 a user-friendly summary version, and a reminder table. Recruitment and Follow-Up Patients were enrolled through nine tertiary care cancer centers throughout Canada, where they received adjuvant treatment and were receiving © 2011 by American Society of Clinical Oncology Information downloaded from jco.ascopubs.org and provided by at ST LUCAS ANDREAS ZIEKENHUIS on September 24, Copyright © 2011 American Society Clinical Oncology. All rights reserved. 2014 fromof85.90.80.12 4757 Grunfeld et al routine follow-up care. After providing informed consent, eligible patients were allocated according to a prescribed computer-generated center and stratum-specific randomization schedule in a 1:1 ratio to either the intervention or control group. Concealed allocation was performed by contacting the trial coordination center of the Ontario Clinical Oncology Group by telephone. Assessments were completed at baseline and at 3, 6, 12, 18, and 24 months. All patients were followed up for recurrence or death. We report here the 12-month primary outcome assessment. Outcomes Trial outcomes were selected to measure the objectives and expected benefits of SCPs. Patient-reported outcomes were used to measure the domains of cancer-specific distress (ie, Impact of Events Scale [IES])21; general psychological distress (ie, profile of mood states [POMS]),22 for which higher scores indicate worse distress; health-related quality of life (ie, short form 36 physical and mental component summaries [ie, short-form 36 of the healthrelated quality-of-life questionnaire, PCS and MCS])23; patient satisfaction Table 2. Trial Outcomes Outcome Score At 3 Months SCP Variable Cancer-specific distress by IES Intrusion Avoidance a Total score Psychologic distress by POMS Tension/anxiety Depression/dejection Anger/hostility Fatigue/inertia Confusion/bewilderment Vigor/activity Total scoreb Patient satisfaction by PSQ General satisfaction Technical quality Communication Financial aspect Time spent with doctor Accessibility and convenience Total scorec,d General health status by SF-36e Physical component scale Mental component scale Continuity of care by CCCQd,f Informational Management Relational Total score Physician primarily responsible for follow-up, %g Primary care physician Cancer physician Cancer surgeon Other At 6 Months No SCP SCP At 12 Months No SCP SCP Mean SD Mean SD Difference 95% CI for Difference Mean SD Mean SD Difference 7.3 10.0 17.4 7.3 9.5 15.4 7.4 9.7 17.1 7.1 8.9 14.3 ⫺0.1 0.3 0.2 ⫺1.6 to 1.4 ⫺1.7 to 2.3 ⫺3.0 to 3.4 6.7 10.5 17.2 7.0 9.9 15.1 7.5 10.5 18.0 7.2 9.2 14.8 ⫺0.8 0.0 ⫺0.8 2.9 2.2 2.1 4.7 3.7 9.7 8.8 3.3 3.1 3.0 4.2 1.9 4.6 12.8 3.3 2.5 2.3 4.9 3.9 9.7 9.9 3.4 3.5 3.2 4.4 2.1 4.5 14.6 ⫺0.3 ⫺0.4 ⫺0.2 ⫺0.2 ⫺0.1 0.0 ⫺1.0 ⫺1.1 to 0.4 ⫺1.1 to 0.4 ⫺0.9 to 0.5 ⫺1.1 to 0.8 ⫺0.6 to 0.3 ⫺1.0 to 1.0 ⫺4.0 to 1.9 2.2 1.7 1.6 4.2 3.3 9.5 6.6 2.5 2.5 2.2 3.7 1.6 4.6 9.6 2.9 2.3 2.3 4.8 3.8 9.6 9.5 3.4 3.6 3.2 4.6 2.5 4.7 15.3 ⫺0.6 ⫺0.6 ⫺0.7 ⫺0.6 ⫺0.6 ⫺0.2 ⫺2.9 95% CI for Difference No SCP 95% CI for Difference Mean SD Mean SD Difference ⫺2.3 to 0.8 ⫺2.1 to 2.1 ⫺4.1 to 2.5 6.5 9.6 16.1 7.1 10.2 15.8 7.2 9.6 16.8 7.6 9.0 15.2 ⫺0.7 ⫺0.0 ⫺0.7 ⫺2.3 to 1.0 ⫺2.1 to 2.1 ⫺4.1 to 2.8 ⫺1.3 to 0.0 ⫺1.3 to 0.1 ⫺1.3 to ⫺0.1 ⫺1.5 to 0.3 ⫺1.0 to ⫺0.1 ⫺1.2 to 0.9 ⫺5.7 to ⫺0.1 2.5 2.1 2.1 4.5 3.5 10.1 7.7 3.0 3.0 3.0 4.1 1.8 4.8 12.0 3.2 2.4 2.4 5.4 3.8 9.8 10.3 3.5 3.4 3.4 5.0 2.2 4.8 15.1 ⫺0.7 ⫺0.3 ⫺0.3 ⫺0.9 ⫺0.3 0.3 ⫺2.6 ⫺1.4 to 0.0 ⫺1.0 to 0.4 ⫺1.0 to 0.4 ⫺1.9 to 0.1 ⫺0.7 to 0.2 ⫺0.7 to 1.4 ⫺5.6 to 0.5 73 74 74 81 71 18 15 16 18 19 69 72 72 80 68 20 16 18 18 22 3.9 1.9 1.5 0.9 3.4 ⫺0.2 to 8.0 ⫺1.4 to 5.2 ⫺2.2 to 5.1 ⫺3.0 to 4.7 ⫺1.0 to 7.8 72 73 75 80 71 21 16 16 19 20 71 71 72 80 67 21 16 18 16 20 1.9 1.2 3.0 0.3 3.8 ⫺2.7 to 6.5 ⫺2.3 to 4.8 ⫺0.7 to 6.8 ⫺3.6 to 4.1 ⫺0.6 to 8.2 69 70 74 79 70 21 17 16 19 20 71 73 72 82 68 21 17 20 17 20 ⫺2.3 ⫺2.9 1.4 ⫺2.7 2.0 ⫺7.1 to 2.5 ⫺6.8 to 0.9 ⫺2.6 to 5.5 ⫺6.6 to 1.3 ⫺2.5 to 6.4 63 72 19 13 61 70 18 14 1.6 2.2 ⫺2.4 to 5.5 ⫺0.6 to 5.1 63 72 19 14 61 70 18 14 1.5 2.0 ⫺2.6 to 5.6 ⫺1.1 to 5.1 61 70 20 14 63 71 16 14 ⫺2.1 ⫺1.1 ⫺6.1 to 1.8 ⫺4.2 to 1.9 48 51 9 9 49 50 9 11 ⫺1.1 0.8 ⫺3.0 to 0.8 ⫺1.4 to 3.1 49 52 9 9 49 49 9 11 0.0 2.6 ⫺2.0 to 2.0 0.4 to 4.8 48 51 9 9 48 50 9 11 ⫺0.2 1.8 ⫺2.3 to 1.8 ⫺0.4 to 4.1 0.1 ⫺0.0 0.1 0.0 ⫺0.1 to 0.2 ⫺0.1 to 0.1 ⫺0.1 to 0.2 ⫺0.1 to 0.1 3.7 3.6 3.9 3.6 0.2 ⫺0.0 0.1 0.1 ⫺0.0 to 0.3 ⫺0.1 to 0.1 ⫺0.1 to 0.3 ⫺0.1 to 0.2 3.5 3.5 3.8 3.6 0.0 ⫺0.1 ⫺0.0 ⫺0.0 ⫺0.2 to 0.2 ⫺0.2 to 0.1 ⫺0.2 to 0.2 ⫺0.1 to 0.1 ⫺2.5 to 10.2 96.1 2.6 1.3 1.3 2.8 ⫺2.9 to 8.5 98.7 0.7 1.3 1.3 3.6 3.6 3.9 3.6 92.8 4.8 4.2 3.6 0.7 0.5 0.7 0.4 3.5 3.6 3.8 3.6 0.8 0.5 0.7 0.5 88.9 7.6 7.0 4.1 3.8 0.8 0.6 0.7 0.5 3.5 3.6 3.8 3.6 93.3 4.8 3.6 3.0 0.8 0.5 0.8 0.5 0.7 0.5 0.7 0.4 3.5 3.6 3.8 3.6 89.1 5.1 6.4 1.9 0.7 0.5 0.7 0.5 9.6 3.9 to 15.9h Abbreviations: CCCQ, continuity/coordination of care; IES, Impact of Events Scale; POMS, profile of mood states; PSQ, personal satisfaction questionnaire; SCP, survivorship care plan; SD, standard deviation; SF-36, short-form 36 of the health-related quality-of-life questionnaire. a Theoretical range is 0 to 75; higher scores indicate greater distress. b Theoretical range is 0 to 100; higher scores indicate greater distress. c Theoretical range is 0 to 100; higher scores indicate greater satisfaction. d PSQ interpersonal manner subscale and CCCQ patient preference subscale had ␣ ⬍ .7, which suggests poor reliability in this patient group; therefore, results are not shown. e SF-36 physical and mental component scales are standardized and weighted to have a mean of 50 and SD of 10 in the US general population; higher scores indicate better functioning. f Theoretical range is 0 to 5; higher scores indicate better continuity/coordination. g Some patients indicated multiple providers. Denominator is the number of patients who listed at least one provider. h Difference in the proportion of patients who named their primary care physician as primarily responsible; P ⫽ .0005. 4758 © 2011 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY Information downloaded from jco.ascopubs.org and provided by at ST LUCAS ANDREAS ZIEKENHUIS on September 24, Copyright © 2011 American Society Clinical Oncology. All rights reserved. 2014 fromof85.90.80.12 Evaluating Cancer Survivorship Care Plans (ie, Medical Outcomes Study-Patient Satisfaction Questionnaire [MOS-PSQ])24; andcontinuity/coordinationofcare(ie,CCCQ),25 forwhichhigherscoresindicate better quality of life, satisfaction, and continuity and coordination of care. The primary instrument in this trial was the IES, which assesses distress anchored to a specific event, defined as breast cancer. Cancerspecific distress rather than general distress was considered most relevant, both for this patient population and for the trial intervention.22,26,27 The IES has been validated extensively21 in English and French and has been used widely in breast cancer populations.22,27-29 The instrument consists of 15 questions, each with four choices, that have scores ranging from 0 to 5 (for which higher scores represent a more stressful impact); the IES total score ranges from 0 to 75. It comprises two subscales, intrusion (score range, 0 to 35) and avoidance (score range, 0 to 40). The primary outcome was the change in IES total score from baseline to 12 months. Secondary outcomes included a similar change in the total score and subscales of the following patient-reported measures: POMS, healthrelated quality of life short form 36, MOS-PSQ, and CCCQ. Health services outcomes included the frequency with which patients declined transfer to PCP, the frequency and types of postdischarge visits to the oncologist, and the awareness of which physician was primarily responsible for follow-up care. The primary analysis was based on a two-sample t test for the change in IES total score from baseline to 12 months, with imputation of 6-month data for those missing 12-month data within each stratum. Supportive linear regression analyses were performed to investigate the effect of the intervention and strata on the 12-month scores after analysis was adjusted for the baseline score, age in years, education, tumor grade, and number of months since diagnosis. Additionally, an analysis of covariance model with 12-month absolute IES scores as the outcome and baseline IES scores and intervention group as covariates was performed. Intervention effects within stratum were assessed in the multivariable model. Profiles of the various scores over time were investigated by using a repeated-measures, linear, mixed model that adjusted for the baseline score, age in years, education, tumor grade, and number of months since diagnosis. The proportion of patients naming their PCP as primarily responsible for their care was calculated, and the number of patients who reported at least one physician responsible was in the denominator. The difference between groups was estimated by using the continuity-corrected score statistic. All statistical analyses were performed with SAS, version 9.1(SAS Institute, Cary, NC) or R software, version 2.7.1 (www.r-project.org). Statistical Analysis Sample size was calculated to detect a six-point change in IES total score within each stratum separately by using a two-sample t test. A change of that magnitude was considered clinically important on the basis of the results of a previous trial in a similar patient population29; it corresponds to an effect size of 0.46. The level of significance within each stratum was set to ␣ ⫽ .025 (two sided) to account for the multiple testing. To obtain 80% power and allow for 10% dropout, 100 patients per group per strata were targeted. Intention-to-treat analyses were performed within each stratum separately and were combined across strata. Results within stratum were similar to the combined analysis; hence, only the combined results are presented for brevity. Descriptive statistics summarized patient characteristics and baseline measures by randomized group. Means and standard deviations (SDs) summarized outcome measures at 3, 6, and 12 months after baseline, and 95% CIs for the difference in means were constructed at each assessment time for total scores and subscale scores. Scoring was performed according to the recommended procedures for each instrument.25,30-33 For all measures, the within-patient change from baseline scores was calculated as the postbaseline score minus the baseline score. For outcomes in which scoreswithahighvalueindicateaworseoutcome(ie,IES,POMS),anegativevalue indicates improvement from baseline, and a positive value indicates worsening from baseline. For outcomes in which high scores indicate better functioning (ie, PCS, MCS, MOS-PSQ, and CCCQ), a negative value indicates worsened function, and a positive value indicates improvement. The difference in means between treatment groups was calculated as the intervention score minus the control score: a positive value indicates that the average intervention score was higher than the average control score, indicating a worse outcome for IES and POMS and a better outcome for PCS, MCS, MOS-PSQ, and CCCQ. RESULTS Trial Patients Of the eligible patients, 64% agreed to participate (Fig 1) and to accept transfer to the PCP for routine follow-up. Overall, 408 breast cancer survivors were enrolled: 180 were enrolled in the stratum of fewer than 24 months, and 228 were enrolled in the stratum of ⱖ 24 months. Baseline characteristics were balanced between the two trial groups (Table 1). Greater than two thirds of patients had nodenegative tumors and received breast-conserving surgery and adjuvant radiation and hormonal therapy; approximately 40% received adjuvant chemotherapy. The mean time from diagnosis to enrollment was 35 months, and the maximum time was 300 months (38% were diagnosed greater than 6 years previously). Patient Outcomes The results up to the 12-month visit are reported. There were no statistically significant or clinically important between-group differences on total scores, subscale scores (Table 2), or change scores (Table 3) on any outcome measure at any time point. The between-group comparisons of change from baseline on total and selected subscale scores are shown in Figure 2. All patients showed a non– clinically important improvement over time in the primary outcome for both IES total scores and subscale scores. At 12 months, changes in the IES Table 3. IES Total Score: Change From Baseline to 12 Months by Intervention and Time Since Diagnosis Group Patients diagnosed at ⬍ 24 months No SCP SCP Patients diagnosed at ⱖ 24 months No SCP SCP All patients No SCP SCP At Baseline At 12 Months Change Effect of SCP Intervention No. of Patients Mean SD Mean SD Mean SD Mean 95% CI P 80 74 21.1 20.9 15.3 15.3 18.4 18.0 15.0 16.2 ⫺2.7 ⫺2.9 13.1 11.3 ⫺0.3 ⫺4.2 to 3.7 .90 100 91 17.1 18.0 13.2 15.8 16.8 15.0 15.4 15.2 ⫺0.3 ⫺3.0 12.6 13.5 ⫺2.6 ⫺6.4 to 1.1 .16 180 165 18.9 19.3 14.2 15.6 17.5 16.4 15.2 15.7 ⫺1.4 ⫺2.9 12.8 12.5 ⫺1.6 ⫺4.3 to 1.1 .25 Abbreviations: IES, Impact of Events Scale; SCP, survivorship care plan; SD, standard deviation. www.jco.org © 2011 by American Society of Clinical Oncology Information downloaded from jco.ascopubs.org and provided by at ST LUCAS ANDREAS ZIEKENHUIS on September 24, Copyright © 2011 American Society Clinical Oncology. All rights reserved. 2014 fromof85.90.80.12 4759 Grunfeld et al A SCP No SCP B PSQ IES: Total 6 0 6 SCP No SCP 0 -6 -6 0 3 6 9 12 0 3 Time (months) C SCP No SCP SF-36: PCS IES: Intrusion D 0 0 SCP No SCP 6 0 3 6 9 12 0 3 Time (months) SCP No SCP F SF-36: MCS IES:Avoidance 6 9 12 Time (months) 4 0 -4 SCP No SCP 6 Fig 2. Trial outcomes: change scores over time. Blue line, supportive care plan (SCP) group; gold line, no SCP. CCCQ, Continuity/Coordination of Care; IES, Impact of Events Scale; POMS, profile of mood states; PSQ, personal satisfaction questionnaire; SF-36, short-form 36 of the health-related quality-of-life questionnaire. 0 -6 0 3 6 9 12 0 3 Time (months) 6 9 12 Time (months) SCP No SCP 0 SCP No SCP 0.3 CCCQ 4 POMS 12 -6 -4 G 9 Time (months) 4 E 6 0 -0.3 -4 0 3 6 9 12 0 Time (months) 3 6 9 12 Time (months) total score overall, and within the strata defined by time since diagnosis, were reduced in the intervention group, but the effects were not statistically significant (Table 3). The analysis of covariance model showed no statistically significant effect for intervention (P ⫽ .26) on the 12-month IES total score overall after analysis was adjusted for baseline IES total score, nor within either stratum (P ⫽ .18 for ⱖ 24 months since diagnosis and P ⫽ .87 for ⬍ 24 months since diagnosis). The intervention estimates were only minimally affected by the adjustment modeling, and there was no statistically significant interaction effect (P ⫽ .38) between intervention and time since diagnosis. (7.9%) had an oncologist visit. These visits were for suspected recurrence (n ⫽ 6 control and n ⫽ 10 intervention), consideration for an aromatase inhibitor (n ⫽ 5 control and n ⫽ 9 intervention), and routine follow-up (n ⫽ 6 control and n ⫽ 2 intervention). Greater than 89% of patients were able to correctly identify their PCP as primarily responsible for follow-up, although fewer control than intervention patients could do so at each assessment (Table 2). At 12 months, this difference was statistically significant (89.1% v 98.7%; 9.6% difference; 95% CI, 3.9 to 15.9; P ⫽ .005). Health Service Outcomes Five control and nine intervention patients were not transferred to the PCP for follow-up as a result of reasons related to recurrence or other reasons (n ⫽ 1 control and n ⫽ 4 intervention). After transfer to the PCP, 16 control patients (7.8%) and 15 intervention patients DISCUSSION 4760 © 2011 by American Society of Clinical Oncology The results of this trial do not support the hypothesis that SCPs are beneficial for improving patient-reported outcomes of breast cancer survivors. We found no benefit on any outcomes either transiently JOURNAL OF CLINICAL ONCOLOGY Information downloaded from jco.ascopubs.org and provided by at ST LUCAS ANDREAS ZIEKENHUIS on September 24, Copyright © 2011 American Society Clinical Oncology. All rights reserved. 2014 fromof85.90.80.12 Evaluating Cancer Survivorship Care Plans (proximal to the time of transfer to primary care) or at 12 months, which was our primary outcome. Alternative explanations for why we found no differences in cancer-related distress and other outcomes need consideration. The patient-reported outcomes studied were selected to align with the anticipated benefits of SCP to improve cancer-related and general distress, overall health-related quality of life, patient satisfaction, continuity/coordination of care, and transition to primary care.6,7,13 Still, the IES may not have been sensitive enough to capture some intervention effects. Clinical outcomes, such as recurrence rates or survival, were not studied, because they are not expected to be affected by SCPs. We have already shown previously that other clinical outcomes, such as delay in diagnosing recurrence34 or the rate of serious clinical events,35 are not negatively affected by exclusive PCP follow-up. We considered using empowerment, defined as feeling more in control and better able to manage the multifaceted challenges of the cancer experience,36 as the main outcome. However, no instruments validated for patients with cancer were available at the time of trial implementation. An additional consideration is the choice of patient population. It may be that these patients were better adjusted as a result of the time since their original cancer diagnosis, or that breast cancer patients are relatively well informed and have good access to resources compared with those who have other cancers. Thus, our results do not inform as to whether SCPs could be beneficial for other cancer groups, suchaspatientswithprostateandcolorectalcancer,orforaselectedgroup of breast cancer survivors who have greater needs, by using a needs-based stratified approach. The trial findings are generalizable to settings where PCPs are available to provide survivorship care. In such settings, provider satisfaction and PCP knowledge acquisition as a result of SCPs are important topics for additional research, particularly the extent to which the SCP met the needs of PCPs for providing survivorship care.37 We believe that the results of this trial can be generalized to other breast cancer survivors who are ready for transition to follow-up care with a PCP: the HRQOLs resembled that of other Canadian and American women who had completed primary breast cancer treatment.38,39 This trial also supports the findings of our previous trials, which found that transfer of follow-up care to PCPs does not negatively affect a range of patient-reported outcomes.34,35 Transferring routine follow-up to primary care is considered an important strategy to meet the future demand for oncology resources.5,6 In the absence to date of research evidence about the effectiveness of SCPs, SCPs have been perceived as a transition document to facilitate this transfer from oncology care to primary care.6,7 The perception has also been that those who have been followed up longer would be more difficult to transfer and that the SCP could be an effective tool to facilitate that transfer.6,7 In fact, in this trial, for which all patients were transferred to their PCP and one third had been followed up for longer than 5 years (and maximum of 25 years), most patients in both groups and both strata maintained their willingness to be transferred to their PCP, and few patients returned to oncology follow-up after transfer. REFERENCES 1. Living beyond cancer: Finding a new balance. Bethesda, MD, President’s Cancer Panel, US Department of Health and Human Services, www.jco.org Thus, the SCP did not contribute beyond the control condition of a standard discharge visit with the oncologist. It has been shown that patients can be confused about who is responsible for follow-up care.40 Indeed, at baseline in this trial, one third of patients identified their PCP as primarily responsible for follow-up, despite formally receiving follow-up care at the tertiary cancer center where they were enrolled.41 It is noteworthy, therefore, that the SCP in this trial did result in a higher proportion of patients with correct knowledge of which physician was primarily responsible for follow-up care. Others have expressed concerns about who will prepare SCPs.4,7,8,42 Our goal was to conduct a pragmatic trial that was consistent with usual practice and feasible to implement within the time and health human resource constraints of tertiary cancer centers. Hence, both the compilation of the SCP and educational session were undertaken by an oncology nurse. It is possible that, had the intervention been offered by an oncologist, the findings could have been different. Certainly the control group, who received only the standard discharge visit with their oncologist, transitioned as well as those who also received the SCP. This suggests that, if a standard discharge visit is consistently applied, it can accomplish many of the objectives articulated for SCPs. The concept of an SCP is compelling and is considered to have face validity.3 This has led to the widespread endorsement of SCPs by many organizations. However, given the potential barriers to implementation4,7,42 and opportunity costs associated with compiling and implementing a comprehensive SCP given scarce oncology resources,5 careful thought must be given to the benefits that could be realized. The only benefit identified in this trial was that more patients correctly identified the PCP as primarily responsible for follow-up care. The question remains whether this is sufficiently compelling to warrant the necessary resource allocation.13 AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST The author(s) indicated no potential conflicts of interest. AUTHOR CONTRIBUTIONS Conception and design: Eva Grunfeld, Jim A. Julian, Elizabeth Maunsell, Douglas Coyle, Amy Folkes, Anil A. Joy, Louise Provencher, Daniel Rayson, Dorianne E. Rheaume, Geoffrey A. Porter, Lawrence F. Paszat, Kathleen I. Pritchard, André Robidoux, Jonathan Sussman, Susan Dent, Jeffrey Sisler, Jennifer Wiernikowski Provision of study materials or patients: Louise Provencher Collection and assembly of data: Jim A. Julian, Gregory Pond, Amy Folkes, Louise Provencher, André Robidoux, Sally Smith, Mark N. Levine Data analysis and interpretation: Eva Grunfeld, Jim A. Julian, Gregory Pond, Elizabeth Maunsell, Douglas Coyle, Mark N. Levine Manuscript writing: All authors Final approval of manuscript: All authors National Institutes of Health, National Cancer Institute, 2004. http://deainfo.nci.nih.gov/ADVISORY/ pcp/pcp03-04rpt/Survivorship.pdf 2. Estimated US cancer prevalence counts: Who are our cancer survivors in the US? Bethesda, MD, National Cancer Institute, 2009. http://cancercontrol.cancer.gov/ocs/prevalence/ index.html 3. Hewitt ME, Greenfield S, Stovall E: From Cancer Patient to Cancer Survivor: Lost in Transition. Washington, DC, National Academies Press, 2006 © 2011 by American Society of Clinical Oncology Information downloaded from jco.ascopubs.org and provided by at ST LUCAS ANDREAS ZIEKENHUIS on September 24, Copyright © 2011 American Society Clinical Oncology. All rights reserved. 2014 fromof85.90.80.12 4761 Grunfeld et al 4. Implementing Cancer Survivorship Care Planning: Workshop Summary. Washington, DC, Institute of Medicine of the National Academies, 2007 5. Erikson C, Salsberg E, Forte G, et al: Future supply and demand for oncologists: Challenges to assuring access to oncology services. J Oncol Pract 3:79-86, 2007 6. Ganz PA, Hahn EE: Implementing a survivorship care plan for patients with breast cancer. J Clin Oncol 26:759-767, 2008 7. Earle CC: Failing to plan is planning to fail: Improving the quality of care with survivorship care plans. J Clin Oncol 24:5112-5116, 2006 8. Ganz PA, Casillas J, Hahn EE: Ensuring quality care for cancer survivors: Implementing the survivorship care plan. Sem Onc Nurs 24:208-217, 2008 9. American Cancer Society: Survivorship: During and after treatment. Washington, DC. http://www .cancer.org/Treatment/SurvivorshipDuringandAfter Treatment/index 10. The National Cancer Survivorship Initiative Vision. London, United Kingdom Department of Health, 2010. http://www.dh.gov.uk/prod_consum_dh/ groups/dh_digitalassets/@dh/@en/@ps/documents/ digitalasset/dh_111477.pdf 11. Canadian Partnership Against Cancer: Priorities: Survivorship. http://www.partnershipagainst cancer.ca/priorities/cancer-journey/strategicinitiatives/survivorship/ 12. Ganz PA, Earle CC, Schrag D, et al: The survivorship care plan: What, why, how, and for whom. New York, NY, Springer, 2007, pp 287-293 13. Earle CC: Long term care planning for cancer survivors: A health services research agenda. J Cancer Surviv 1:64-74, 2007 14. Coleman MP, Forman D, Bryant H, et al: Cancer survival in Australia, Canada, Denmark, Norway, Sweden, and the UK, 1995-2007: The International Cancer Benchmarking Partnership)—An analysis of population-based cancer registry data. Lancet 377:127-138, 2011 15. Zwarenstein M, Treweek S, Gagnier JJ, et al: Improving the reporting of pragmatic trials: An extension of the CONSORT statement. BMJ 337:a2390, 2008 16. Chait I, Glynne-Jones R, Thomas S: A pilot study exploring the effect of discharging cancer survivors from hospital follow-up on the workload of general practitioners. Br J Gen Pract 48:1241-1243, 1998 17. Thomas SF, Glynne-Jones R, Chait I, et al: Anxiety in long-term cancer survivors influences the acceptability of planned discharge from follow-up. Psychooncology 6:190-196, 1997 18. Logan J, Graham ID: Toward a comprehensive interdisciplinary model of health care research use. Sci Commun 20:227-246, 1998 19. CMAJ: Clinical practice guidelines for the care and treatment of breast cancer: Guidelines for Physicians/Questions and Answers for Women, 2005. http://www.cmaj.ca/cgi/content/full/158/3/DC1 20. Grunfeld E, Dhesy-Thind S, Levine M, et al: Clinical practice guidelines for the care and treatment of breast cancer: Follow-up after treatment for breast cancer—Summary of the 2005 update. CMAJ 172:1319-1320, 2005 21. Sundin EC, Horowitz MJ: Impact of event scale: Psychometric properties. Br J Psychiatry 180: 205-209, 2002 22. Stanton AL, Ganz PA, Kwan L, et al: Outcomes from the moving beyond cancer psychoeducational, randomized, controlled trial with breast cancer patients. J Clin Oncol 23:6009-6018, 2005 23. Ware JE, Kosinski M, Keller SD: SF-36 Physical and Mental Health Summary Scales: A User’s Manual. Boston, MA, The Health Assessment Lab, New England Medical Center, 1994 24. Ware JE, Snyder MK, Wright R, et al: Defining and measuring patient satisfaction with medical care. Eval Program Plann 6:247-263, 1983 25. Booth L, Selby P, Brown J, et al: Measurement of continuity and co-ordination of patient care in a cancer centre. Qual Life Res 10:246, 2001 26. Kiebert GM, Welvaart K, Kievet J: Psychological effects of routine follow up on cancer patients after surgery. Eur J Surg 159:601-607, 1993 27. Goodwin PJ, Black JT, Bordeleau LJ, et al: Health-related quality-of-life measurement in randomized clinical trials in breast cancer: Taking stock. J Natl Cancer Inst 95:263-281, 2003 28. Mandelblatt J, Armetta C, Yabroff KR, et al: Descriptive review of the literature on breast cancer outcomes: 1990 through 2000. J Natl Cancer Inst Monogr 33:8-44, 2004 29. Goodwin PJ, Ennis M, Bordeleau LJ, et al: Health-related quality of life and psychosocial status in breast cancer prognosis: Analysis of multiple variables. J Clin Oncol 22:4184-4192, 2004 30. Ware J, Kosinski M, Dewey J: How to Score Version 2 of the SF-36 Health Survey. Lincoln, RI, Quality Metric Incorporated, 2000 31. Hyer K, Brown LM: The impact of event scale, revised: A quick measure of a patient’s response to trauma. Am J Nurs 108:60-68, 2008 32. McNair DM, Lorr M, Droppleman LF: Profile of Mood States Manual. New York, NY, Multi-Health Systems, 2003 33. Marshall G, Hays R: The Patient Satisfaction Questionnaire Short Form (PSQ-18). Santa Monica, CA, RAND Corporation, 1994 34. Grunfeld E, Mant D, Yudkin P, et al: Routine follow-up of breast cancer in primary care: A randomised trial. BMJ 313:665-669, 1996 35. Grunfeld E, Levine MN, Julian JA, et al: Randomized trial of long-term follow-up for early-stage breast cancer: A comparison of family physician versus specialist care. J Clin Oncol 24:848-855, 2006 36. Maunsell E, Lauzier S, Brunet J, et al: Measurement of five dimensions of patient empowerment in oncology: Validation of Health Education Impact Questionnaire (heiQ). Asia Pacific J Clin Oncol 6:3s, 2010 (suppl; abstr 61) 37. Bober SL, Recklitis CJ, Campbell EG, et al: Caring for cancer survivors: A survey of primary care physicians. Cancer 115:4409-4418, 2009 (suppl) 38. Whelan TJ, Goss PE, Ingle JN, et al: Assessment of quality of life in MA. 17: A randomized, placebo-controlled trial of letrozole after 5 years of tamoxifen in postmenopausal women. J Clin Oncol 23:6931-6940, 2005 39. Ganz PA, Kwan L, Stanton AL, et al: Physical and psychosocial recovery in the year after primary treatment of breast cancer. J Clin Oncol 29:1101-1109, 2011 40. Miedema B, MacDonald I, Tatemichi S: Cancer follow-up care: Patients’ perspectives. Can Fam Phys 49:890-895, 2003 41. Grunfeld E, Levine MN, Julian J, et al: Breast cancer survivors perception of family physician (FP) or specialist as principal provider of routine follow-up care. J Clin Oncol 28:658s, 2010 (suppl; abstr 9090) 42. Jacobs LA, Palmer SC, Schwartz LA, et al: Adult cancer survivorship: Evolution, research, and planning care. CA Cancer J Clin 59:391-410, 2009 Affiliations Eva Grunfeld, Ontario Institute for Cancer Research; Eva Grunfeld, Lawrence F. Paszat, Kathleen I. Pritchard, University of Toronto; Lawrence F. Paszat, Institute for Clinical Evaluative Sciences; Kathleen I. Pritchard, Sunnybrook Health Sciences Centre, Toronto; Jim A. Julian, Gregory Pond, Mark N. Levine, Ontario Clinical Oncology Group; Jim A. Julian, Gregory Pond, Jonathan Sussman, Mark N. Levine, McMaster University; Jonathan Sussman, Jennifer Wiernikowski, Mark N. Levine, Juravinski Regional Cancer Centre, Hamilton; Douglas Coyle, Ottawa Health Research Institute; Susan Dent, The Ottawa Hospital Cancer Centre, The University of Ottawa, Ottawa, Ontario; Elizabeth Maunsell, Unité de recherche en santé des populations (URESP), Université Laval; Louise Provencher, Centre des Maladies du Sein Deschênes-Fabia, Centre de Recherche FRSQ du CHA Universitaire de Québec, Québec; André Robidoux, Centre Hospitalier de l’Université de Montréal, Montréal, Québec; Amy Folkes, Cancer Care Nova Scotia; Daniel Rayson, Dorianne E. Rheaume, Geoffrey A. Porter, Dalhousie University, Halifax, Nova Scotia; Anil A. Joy, Cross Cancer Institute, University of Alberta, Edmonton, Alberta; Sally Smith, BC Cancer Agency, British Columbia; Jeffrey Sisler, University of Manitoba, Winnipeg, Manitoba, Canada. ■ ■ ■ 4762 © 2011 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY Information downloaded from jco.ascopubs.org and provided by at ST LUCAS ANDREAS ZIEKENHUIS on September 24, Copyright © 2011 American Society Clinical Oncology. All rights reserved. 2014 fromof85.90.80.12