Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Menstruation wikipedia , lookup
Reproductive health wikipedia , lookup
Birth control wikipedia , lookup
Prenatal development wikipedia , lookup
HIV and pregnancy wikipedia , lookup
Women's medicine in antiquity wikipedia , lookup
Maternal health wikipedia , lookup
Prenatal testing wikipedia , lookup
Prenatal nutrition wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
List of medical mnemonics wikipedia , lookup
Maternal physiological changes in pregnancy wikipedia , lookup
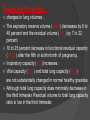
Dr. khaled wagih Assistant professor of pulmonary medicine Ain shams university Objectives I. ANATOMIC CHANGES OF NORMAL PREGNANCY - Airways - Respiratory Muscles and the Thoracic Cage II. PHYSIOLOGICAL CHANGES OF NORMAL PREGNANCY - Respiratory Physiology - Cardiovascular Physiology - Sleep Disturbances - Dyspnea of Pregnancy III. ACUTE RESPIRATORY DISTRESS IN PREGNANCY IV. RESPIRATORY DISEASES IN PREGNANCY - Asthma - Venous Thromboembolism - Pulmonary Hypertension - Sleep-Disordered Breathing - Cystic Fibrosis PULMONARY COMPLICATIONS IN PREGNANCY Pulmonary Complications Obstetric Causes: Dyspnea of pregnancy Mechanical Hormonal (biochemical) Hemodynamic changes Pulmonary diseases Pneumothorax and pneumomediastinum Valsalva maneuver (second stage of labor) Pulmonary edema Aspiration Eclampsia Tocolytic therapy Pulmonary embolism Amniotic fluid embolism Disseminated intravascular coagulation Trophoblastic embolism Transfusion reactions Sepsis (septic abortion) Pleural effusion Postpartum Pulmonary hypertension Sarcoidosis, rhinitis, asthma, tuberculosis, and cystic fibrosis The respiratory system is affected by the normal anatomic and physiologic alterations that take place throughout pregnancy, parturition, and early postpartum. A healthy pregnant woman experiences minimal or tolerably mild respiratory symptoms. A pre-existing pulmonary problem, however, can be exacerbated by pregnancy. On the other hand, the normal course of the pregnancy can be adversely affected by preexisting respiratory disorders to the point of threatening the pregnancy itself ANATOMIC CHANGES OF NORMAL PREGNANCY: Basic structural changes occur in the upper and lower airways, thoracic cage, and the respiratory muscles, most notably the diaphragm. Airways : upper airways Hyperemia, friability, mucosal edema, and hypersecretion of the airway mucosa May be aggravated by preeclampsia, upper respiratory tract infection, or allergic rhinitis. Nasal obstruction, epistaxis, sneezing episodes, and vocal changes. Nasal and sinusoidal polyposis is often seen and tends to recur in women with each pregnancy. Nasal obstruction may contribute to upper airway obstruction during sleep, leading to snoring and even obstructive sleep apnea. Lower airways : The anatomic changes not characterized, but some of the mucosal changes that affect the upper airways may also occur in the central portion of the airway, such as the larynx and trachea. Nonspecific complaints of airway irritation, such as irritant cough or sputum production, may be intensified during pregnancy, often in association with functional changes in airway reactivity and/or coexistent pulmonary conditions. The physiological causes of nasal mucosal changes appear to be predominantly mediated by estrogens Respiratory Muscles and the Thoracic Cage: The enlarging uterus produces upward displacement of the diaphragm. Although the diaphragm may be elevated up to 4 cm cephalic, diaphragmatic function is not impaired increase in the antero posterior and transverse diameters of the thoracic cage. Diminished tone and activity of the abdominal muscles Progressive relaxation of the ligamentous attachments of the ribs broadens the subcostal angle by approximately 50percent. , There is a 5 to 7 cm increase in chest circumference. upward and lateral displacement of the cardiac apex on chest radiography. PHYSIOLOGICAL CHANGES OF NORMAL PREGNANCY: Both respiratory and cardiovascular changes ensure the delivery of necessary oxygenated blood and other nutrients required for this process. Respiratory Physiology : changes in lung volumes . The expiratory reserve volume ( ERV) decreases by 8 to 40 percent and the residual volume ( RV ) by 7 to 22 percent. 10 to 25 percent decrease in functional residual capacity ( FRC ) after the fifth or sixth month of pregnancy. Inspiratory capacity ( IC ) increases. Vital capacity ( VC ) and total lung capacity (TLC) are not substantially changed in normal healthy gravidas, Although total lung capacity does minimally decrease in the third trimester. Residual volume to total lung capacity ratio is low in the third trimester. Tidal volume increases considerably, 30 to 35%, as a result of increased ventilatory drive. Maximum voluntary ventilation does not change greatly during pregnancy. Values of FEV1 throughout pregnancy are not significantly different from the non pregnant condition. Increased gastric and esophageal pressure occurring in late pregnancy has been considered major factors that produce a decrease in trans pulmonary pressure leading to peripheral airway collapse. An increase in lung water, resulting in a change in the elastic properties of the lungs. Progressive increases of airway conductance have been reported to occur between 6 months of pregnancy and term along with a decrease in airway resistance. Total pulmonary resistance, consisting of both airway and tissue resistance, is reduced by approximately 50 percent in pregnancy. Lung compliance does not change. Compliance of the thoracic cage decreases, as the anatomic changes in chest wall and the decrease in tone and activity of the abdominal musculature In early pregnancy, the diffusing capacity is either unchanged or slightly increased. Throughout the rest of pregnancy, the diffusing capacity decreases, returning to normal or slightly lower than normal values. The relative contributions of the specific factors that affect diffusion, such as membrane diffusing capacity and pulmonary capillary blood volume, are not known. Minute ventilation increases 20 to 50 percent before the end of the first trimester due to the effect of increased serum progesterone Carbon dioxide production and oxygen consumption increase as a result of the increase in basal metabolic rate. Progesterone levels increase gradually during pregnancy from 25 ng/ml at 6 weeks to 150 ng/ml at 37 weeks. Mouth occlusion pressures increase progressively during pregnancy in keeping with increasing progesterone levels. Estrogen may have an additional effect by causing an increased responsivity of the respiratory center. Arterial PCO2 falls to levels of 32 to 28 mmHg. plasma bicarbonate decreases to 21 to 18 mEq/L. Arterial pH is maintained in the range of 7.40 to 7.45. Values for arterial PO2 are generally greater than 100 mmHg during pregnancy. With the supine position, the alveolar-arterial oxygen gradient may widen, and mild arterial hypoxemia may develop. Respiratory responses during parturition are greatly affected by stage of labor and the response to pain and anxiety During labor, tidal volumes ranging from 350 to 2250 ml and minute ventilations from 7 to 90 L/min have been recorded. The higher values were close to the maximum voluntary ventilation and were associated with the second stage of labor The lower values were obtained in the first stage of labor while the patient was sedated. Along with the alveolar hyperventilation, oxygen consumption during labor doubles and can even triple (e.g., to 750 ml/min) during uterine contractions. The possibility of relative hypoventilation between contractions coupled with the grave implications of fetal hypoxemia makes it reasonable to be liberal in the use of oxygen Sleep Disturbances: Sleep quality is often poor. Sleep disruption can be due to leg cramps, low back pain, urinary frequency, or responsibilities relating to child care. Total sleep time and daytime sleepiness increase during the first trimester, whereas sleep time decreases and complaints of an increase in the number of nocturnal arousals increase in the third trimester. Sleep Disturbances: Polysomnographic studies have shown an increase in sleep latency, an increase in the amount of stage I sleep and a decrease in rapid eye movement (REM) sleep and delta sleep, as well as an increase in the number of awakenings. The incidence of sleep-disordered breathing during pregnancy is unknown. Cardiovascular Physiology: Beginning around the fifth week of pregnancy and continuing into the postpartum period. Cardiac output increases and peaks near term at 30 to 50 percent above normal. Increases in heart rate, stroke volume (10 to 30%) above prepartum values by week 12 and a decrease (20 to 30%) in pulmonary and peripheral vascular resistances. This response is principally a result of an increase in endogenous catecholamines and an increase in venous return of up to 300 to 500 ml of blood that occurs during uterine contractions. Maternal blood volume increases progressively throughout pregnancy, beginning as early as 4 to 6 weeks of gestation and plateauing at approximately 32 to 34 weeks of gestation .Total blood volume increases up to 35 to 50 percent above baseline (approximately 1.6 L), peaking by the third trimester. Plasma volume increases to a greater degree than red blood cell mass, which increases less, and more gradually, to an average increase of about 25%. These changes result in a decrease of hemoglobin concentration and hematocrit, producing the “physiological anemia of pregnancy.” The increase in blood volume is probably determined by multiple, primarily endocrine factors, such as estrogen stimulation of aldosterone, nonrenal renin, and atrial natriuretic factor. Chorionic somatomammotropin, progesterone, and possibly prolactin probably stimulate the increase in red blood cell mass. Extracellular water increases by 1 to 2 L, results in the peripheral edema that occurs in 50 to 80 %of normal pregnancies. Left ventricular wall thickness increases by 28 % and left ventricular mass by 52 % above baseline, resulting in a decrease in left ventricular compliance. Central venous pressure, pulmonary capillary wedge pressure, and left ventricular stroke work do not change significantly Systemic blood pressure, especially the diastolic component, is slightly lower during pregnancy. Diastolic blood pressure reaches its nadir in the middle of the third trimester, falling by 10 to 20% of prepregnancy values. Subsequently, blood pressure increases to near prepregnancy levels. Dyspnea of Pregnancy 60 to 70 %. commonly occur during the first and second trimester and remain stable or improve near term . increased ventilatory drive and increased mechanical load. Excessive chemoreceptor sensitivity to carbon dioxide or hypoxemia. ACUTE RESPIRATORY DISTRESS IN PREGNANCY As a rule, causes of respiratory distress due to conditions specific to pregnancy (e.g., amniotic fluid embolism, or pulmonary edema secondary to preeclampsia or tocolytic therapy) pose little problem in clinical diagnosis. invasive hemodynamic monitoring to differentiate between cardiogenic and noncardiogenic pulmonary edema. Pulmonary thromboembolism should always be strongly considered RESPIRATORY DISEASES IN PREGNANCY Bronchial Asthma: The risks of poorly controlled asthma to the mother and fetus are greater than those posed by most medications (including oral corticosteroids) Approximately 4 to 8 % of pregnant women in the United States are asthmatic No association between asthma and preterm delivery or adverse perinatal outcomes Neonatal sepsis and an increased maternal cesarean section rate in women with moderate or severe asthma. Pharmacologic management is quite similar utilizing inhaled short acting beta2-agonists, inhaled corticosteroids, inhaled long acting beta2agonists, and systemic corticosteroids. leukotriene receptor antagonists and Theophylline are safe Oral corticosteroid use in the first trimester is associated with a small increased risk of isolated cleft lip with or without cleft palate (0.1 to 0.3 percent), and may be associated with increased risks of pregnancy-induced hypertension, preeclampsia, preterm delivery, and low birth weight. Class A: Controlled human studies have demonstrated no risks to the fetus. Class B: Presumed safe, based on animal studies; no wellcontrolled human studies are available. Class C: Safety is uncertain; data from human studies do not exist, and animal studies have shown some question of risk to the fetus. Pregnant women may take these medicines if they clearly need them. Class D: Evidence suggests the possibility of the medication causing birth defects or other problems, but a pregnant woman still might need to take it for her own medical needs. Class X: Proven risks to the fetus outweigh any possible benefits to the mother Venous Thromboembolism: 0.5 to 3.0 per 1000 pregnancies in those without a history of thromboembolism. Prior thromboembolic disease, smoking, prior venous thrombosis, and thrombo-philias are risk factors for deep venous thrombosis or pulmonary embolism (PE) during pregnancy. The risk of venous thromboembolism is greatest in the postpartum period. Evaluation… venous ultrasound LLS. If negative, a ventilation-perfusion (V-P) scan or helical computed tomography (CT) scan should be performed next Confirmed cases of venous thromboembolism during pregnancy should be managed with unfractionated or low molecular weight heparins. Coumarin should be avoided due to the risk of embryopathy. Pulmonary Hypertension: The cardiovascular and hemodynamic changes associated with pregnancy, anesthesia, and delivery pose a severe risk to women with primary pulmonary hypertension, Eisenmenger’s syndrome, and secondary pulmonary hypertension. Studies have documented maternal mortalities in these groups from 30 to 56 percent, although most of these studies evaluated patients who did not receive current vasodilator therapy. Recent case reports have documented successful use of intravenous or inhaled epoprostenol, and sildenafil in pregnant women with pulmonary hypertension; however, their long-term effect on overall pregnancy related mortality is unknown. Pulmonary Edema: Obstetric causes of pulmonary edema include aspiration pneumonia, sepsis, transfusion reactions, allergic reactions, disseminated intravascular coagulation, amniotic fluid embolism, toxemia of pregnancy, tocolytic therapy, and eclampsia, the latter being the most common cause of pulmonary. - Bromocriptine therapy to suppress lactation can also cause postpartum pulmonary edema - Decreased venous tone and venous resistance lead to iatrogenic pulmonary edema. Pleural Effusion Pleural effusions occur with toxemia of pregnancy, preeclampsia, pulmonary edema, pulmonary embolism, choriocarcinoma, and amniotic fluid embolism . Small pleural effusions are common in the postpartum period in normal pregnancy. Sleep-Disordered Breathing: Hormonal changes of increased estrogen resulting in hyperemia and upper airway narrowing. increased progesterone resulting in increased respiratory drive. Other physiologic changes of sleep (decreased FRC and respiratory system compliance) predispose to alterations in sleep during pregnancy. While snoring is increased in pregnancy, and sleep-disordered breathing may worsen during pregnancy, the incidence and prevalence of sleep-disordered breathing during pregnancy are unknown Symptoms of sleep-disordered breathing should be reviewed with women who develop pregnancy-induced hypertension or preeclampsia, and all pregnant women with symptoms of sleep-disordered breathing should be evaluated with a polysomnogram and treated with nasal continuous positive airway pressure as indicated. Cystic As Fibrosis: survival of individuals with cystic fibrosis continues to improve, Maternal and fetal outcomes are satisfactory for women with good lung function and nutritional status. Pregnancy appears to have no deleterious effect on long-term survival in women with cystic fibrosis. Barotrauma: Spontaneous pneumothorax and pneumo mediastinum may appear during pregnancy, but these are more likely to occur during the second stage of labor. Repeated Valsalva maneuvers are the most frequent cause of these problems. Pneumo mediastinum is a rare complication of pregnancy, and symptoms usually are not noted until after delivery Kyphoscoliosis Most common abnormality of the thoracic cage affecting pregnancy. Kyphoscoliosis is known to result in ventilatory failure by interfering with the respiratory mechanics. Severe kyphoscoliosis is associated with increased perinatal and maternal mortality. Regular lung function tests, arterial blood gases measured, and be given oxygen if hypoxaemic Smoking and Pregnancy spontaneous pregnancy loss. placental abruption. preterm premature rupture of membranes. placenta previa. preterm labor and delivery. stillbirth, and low birth weight . postnatal morbidities Smoking and Pregnancy Maternal smoking during pregnancy may impair in utero airway development or alter lung elastic properties, and these effects may be important factors predisposing infants to the occurrence of wheezing illness later in childhood. Tuberculosis Hippocratic view young woman with tuberculosis should become pregnant to improve her outcome!! 1850 - 1920s tuberculosis was harmful during pregnancy, and termination of pregnancy - recommended Tuberculosis during pregnancy -rarely an indication for a therapeutic abortion But pregnant woman with MDRTB, should be offered abortion counseling medications used are known to cause fetal abnormalities Diagnosing tuberculosis in pregnancy Symptoms like malaise & fatigue may be ignored in pregnancy late diagnosis sputum examination and culture -same as for non-pregnant Maternal outcome Depends on site & timing of diagnosis Late diagnosis – morbidity increase 4 fold Early diagnosis – outcome similar to non pregnant women Perinatal outcome Late diagnosis increase incidence of prematurity and LBW Early diagnosis outcome similar to non pregnant woman Anti-tuberculous therapy No increase in congenital malformations or fetal damage when rifampicin, isoniazid and ethambutol are used in combination pyrazinamide is also considered to be a safe drug in pregnancy Congenital tuberculosis Cantewell Criteria 1. Lesion in the first week 2. Primary hepatic complex or caseating granuloma 3. Documented TB of placenta or endometrium 4. Exclusion of TB infection by carrrier Breast feeding Appears to be safe when the mother is taking standard anti-tuberculous medication. If the mother is taking isoniazid, pyridoxine supplementation should be given to the child as a small amount of isoniazid is present in breast milk It is usually unnecessary for the child to receive treatment unless the mother is diagnosed with open (infectious) at the time of delivery Mother with open Tuberculosis Breast feeding can be done with: INAH prophylaxis mother can use a mask Neonate…. INAH prophylaxis is given for 3 months Check Mantoux Mantoux Negative need BCG vaccination Contraception Oral contracepitves: effectiveness is reduced HIV,TB If and pregnancy a pregnant women is diagnosed to have active TB should we screen for HIV? Sarcoidosis Sarcoidosis does not seem to have any adverse effects on the course of pregnancy . Pregnancy, on the other hand, is reported to lead to improvement of sarcoidosis in some patients. Patients with active sarcoidosis usually experience partial or complete resolution of chest roentgenographic abnormalities during pregnancy ,although many in this group will experience exacerbation of sarcoid within 3 to 6 months after delivery Amniotic It’s Fluid Embolism estimated that between 5-18 % of all maternal deaths are due to AFE Reported mortality rates range from 26% to as high 86% AFE constitutes the leading cause of mortality during labor and the first few postpartum hours Maternal death occurs in one of three ways: 1) sudden cardiac arrest, 2) hemorrhage due to coagulopathy, 3) or initial survival w/ death due to ARDS and multiple organ failure Risk Factors for AFE 1. 2. 3. 4. 5. 6. 7. Advanced age Multiparity Tumultuous labor Rupture of membranes Fetal death Trauma Uterine overdistention (multiple gestation, fetal macrosomia) Pathophysiology of AFE The anaphylactoid reaction to AFE breaks down to 3 phases: Immediate Phase: occurs when initially exposed and can present as 1) resp distress 2) cyanosis 3)hemodynamic instability 4) cerebral hypoperfusion w/ seizures, confusion or coma Second Phase: characterized by coagulopathy and hemorrhage ; this may be the first and only presentation of AFE Pathophysiology Phase Three: the period after the acute insult is over and the tissue injury is established These patients may die from the severe lung or brain injury, multi-organ failure, or because of an infection acquired during the stay at the ICU Clinical Manifestations Signs and symptoms tend to be nonspecific and common to other forms of embolism Resp distress, cyanosis, cardiovascular collapse, coma, and hemorrhage tend to be the five cardinal signs of AFE Hemorrhage and fetal distress may be the initial symptoms Diagnosis of AFE In the past, the definitive diagnosis was made only at autopsy by finding fetal squamous cells in the maternal pulmonary circulation However, cells of fetal origin were only found in 73% of patients who expired and underwent autopsy Conversely , some Obstetricians have found fetal squamous cells in maternal circulation w/o any evidence of AFE Diagnosis of AFE CXR may be completely normal and the EKG may show signs of acute right ventricular strain in the early stages Echocardiography at the bedside usually confirm severe left ventricular failure Most patients are hemodynamically unstable so it is often difficult to do any specific testing in time to alter management Management of AFE Treatment of AFE is supportive and directed toward: Maintaining oxygenation Maintaining cardiac output, SBP>90 mmHg Acceptable peripheral organ perfusion (urine output >25 ml/hr) Correcting coagulation abnormalities RE-establishing uterine tone Management of AFE Pharmacological treatment may include: • Crystalloids, vasopressors, and inotropic agents (fluids should be restricted once the initial hypotensive episode has resolved to prevent pulmonary edema w/ subsequent ARDS) • Corticosteroids (Hydrocortisone 500mg Q6 hr) • Therapeutic heparinization to limit intravascular coagulation is controversial • In rare instances, cardiopulmonary bypass and pulmonary thromboembolectomy have been successfully used Venous Air Embolism (VAE) VAE is possibly the most common embolic event during the intraoperative period and air can be demonstrated by precordial Doppler auscultation in up to 50% of C/S’s Even so, VAE is responsible for only about 1% of maternal deaths for a rate of approximately one death per 100,000 live births Risk Factors for VAE A gradient of -5 cm H2O between the periphery and the heart would allow significant entry of air into venous circulation Trendelenburg position and exteriorizing the uterus during C/S increase this gradient Uterine exteriorization is thought to predispose to VAE by: 1) increasing the hydrostatic gradient by raising the incisional area above the level of the heart ; 2) by the simultaneous enlargement of the uterine sinuses providing more exposure to air Pathophysiology The major cause of death from VAE is circulatory arrest from air entrapped in the right ventricular outflow tract 5 ml/ kg of air may be lethal by formation of an “air lock” in the right ventricle or in the pulmonary arterial circulation ; this can result in cardiogenic shock In combination w/ PA vasoconstriction , this phenomenon can result in acute cor pulmonale Increased capillary permeability, platelet activation, and coagulopathy may result from the effect of air on endothelial surfaces Clinical Manifestations Massive VAE can present as a sudden and devastating event w/ hypotension, hypoxemia, and even cardiac arrest Typically, the clinical picture is much less dramatic Significant hemodynamic compromise at delivery is only seen about 0.7% to 2% of the time Signs of air embolism include tachycardia, tachypnea, cyanosis, mottled skin, and occasionally, a wheel-mill murmur heard by stethoscope Resuscitation of Massive VAE 1. Discontinue nitrous oxide and give 100% O2 2. Prevent further air entrapment ( flood surgical field, change position) 3. Support ventilation as needed 4. Support circulation 5. If hemodynamic instability persists, consider placement of central line to attempt aspiration of air 6. Expedite delivery 7. If there is delayed emergence from GA, consider neurodiagnostic imaging to r/o intracerebral air ( arterial gas embolism) ; these patients may benefit from hyperbaric therapy, esp. if done w/in 5 hrs Thank You