Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
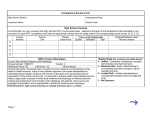
A Case Study: Effects of Lymphatic Drainage on the Symptom Management of Fibromyalgia REBECCA GORGITZA 1005 West Bay Rd, Gambier Island, BC V0N 1V0 250-308-9214 [email protected] Okanagan Valley College of Massage Therapy 200 - 3400 30th Avenue Vernon BC V1T 2E2 1 R. Gorgitza ACKNOWLEDGEMENTS I would like to thank all those at who supported me in the completion of this case study: Lana Henry, who gave me the green light to start this project and instructor / marker, Leslie Bryant-MacLean. Heartfelt thanks to Megan Pocock, Marlaina Meinzinger, and Sarah Leslie for advice, moral support and encouragement when times got tough and stressful. A special thank you to Shanson Lunny who helped me with computer challenges and graphs. And last, but not least, I am grateful to my patient for her co-operation and for sharing her story with me. Without her, this study would not have been possible. 2 R. Gorgitza TABLE OF CONTENTS Acknowledgements ........................................................................................ 2 Abstract …………………………………………………………………….. 4 Introduction …………………………………………………………………. 5 What is Fibromyalgia?........................................................................ 5 Pharmacology ..................................................................................... 7 TENS ………………………………………………………………… 8 Physical Activity ……………………………………………………... 9 Massage Therapy …………………………………………………… 10 Methods ……………………………………………………………………….. 14 Study Design …………………………………………………………… 14 Participant ……………………………………………………………… 14 Outcome Measures……………………………………………………… 15 Measurement Instruments ……………………………………………… 16 Control …………………………………………………………………. 18 Lymphatic Drainage Intervention ...……………………………………. 19 Outcomes ………..……………………………………………………………... 22 Discussion ……..………………………………………………………………. 26 Conclusion …………………..…………………………………………………. 28 References …………………………..…………………………………………. 29 3 R. Gorgitza ABSTRACT Objective: This study aimed to determine whether or not lymphatic drainage has a beneficial effect on symptom management of fibromyalgia. Methods: The study design was a 6-session case study. A female participant with fibromyalgia was selected to complete the study. She underwent six 1-hour long sessions of full body lymphatic drainage, with sessions every other day. The Widespread Pain Index and Symptom Severity questionnaires were used as outcome measures to be completed weekly before and after the intervention, and at shorter increments of time during the intervention. Results: The participant experienced fewer painful areas, fewer symptoms, and less symptom severity during the intervention compared to before. In the time monitored after the intervention, the number of painful areas, symptoms, and symptom severity remained decreased compared to before the intervention. Discussion and Conclusion: Overall, the participant of the study reported a significant decrease in symptom severity and tender points on the WPI alongside some negative effects directly after treatment. More research into the benefits of lymphatic drainage needs to be done to rule out biases of this study such as data collection time. Keywords: fibromyalgia, lymphatic drainage, massage, chronic pain, case study 4 R. Gorgitza INTRODUCTION What is Fibromyalgia? Fibromyalgia (FM) is a chronic pain syndrome characterized by diffuse, widespread muscle and joint tenderness and stiffness. Symptoms accompanying physical Locations of tender point in the body image a pain may include exhaustion, fatigue, headaches, cognitive issues, anxiety, and depression. The American College of Rheumatology(ACR) has defined the system of diagnosis for this condition as follows: “The patient must present with chronic widespread pain in all 4 quadrants of the body for at least 3 months, as well as localized pain at 11 of the 18 tender points (TP).” (Crofford, 2013) This condition may go through phases of remission and exacerbation though complete remission is rare. The etiology of FM is unknown though there are many theories. The ACR proposes that genetics combined with triggers such as stress or physical injury are related to the condition. A hyperactivity of the neurotransmitter ‘substance P’ in cerebrospinal fluid, neuroendrocrine, psychological, nutritional, or sleep 5 R. Gorgitza disturbances and deficiencies are all theories that have been outlined in various studies. (Crofford, 2013) FM affects women more than men (9:1), and it has a greater incidence with increased age - over 50 being the highest incidence. Traumatic experiences that occur in the early years of life, lifestyle choices, and previous episodes of depression are all things that may put a person at risk of developing fibromyalgia. Thus far, no piece of research can fully prove any of these theories, and there is no “cure” or “quick fix” for the disorder. (Alnigenisis et al., 2001) With no cure and a lot of pain and exhaustion, fibromyalgia patients experience a lessened quality of life. It is stated that the symptoms and disability created by FM can have a negative impact on all aspects of life: activities, abilities, self-esteem, and generally health-related quality of life (Dragoi et al., 2012). Many patients are forced to reduce work hours or leave work because of the symptoms they combat (Dragoi et al., 2012). Sleep disturbances are related to FM and they influence everyday lifestyles of FM patients (Theadom, 2010). Lack of sleep can affect productivity rates, lead to difficulty maintaining relationships, and may exacerbate FM symptoms. This cycle of sleeplessness, FM symptoms and pain affect not only health-related quality of life, but also has negative social, functional, and personal implications (Theadom, 2010). 6 R. Gorgitza Since there is no remedy and complete remission is rare, pain management and symptomatic relief are the options for treatment. Medication, TENS, massage, and physical training are some of the methods out there for sufferers to utilize (Ekici et al., 2009) Pharmacology There are plenty of pharmacological options to treat this condition: a range of various antidepressants, muscle relaxants, benzodiazepines, local anesthetics, tricyclic antidepressants (TCA), selective serotonin reuptake inhibitors (SSRI), serotonin and noradrenaline reuptake inhibitors (SNRI), and other drugs such as Tramadol are used to combat fatigue, depression, and pain. Gabapentin and pregabalin are also commonly prescribed for pain and sleep disturbances associated with FM. These drugs have been tested and have been found to be more effective than a placebo in decreasing FM symptoms (Kim et al., 2003). Each drug class has a different rate of effectiveness combined with different adverse effects. TCAs and SNRIs are considered to be much more effective than SSRIs in controlling chronic pain syndromes although it is difficult to say which medication is most successful in decreasing pain and other FM symptoms. Furthermore, pharmacological methods have been found to normalize sleep patterns, decrease sympathetic tone, and combat exacerbations of pain, thus 7 R. Gorgitza affecting the symptoms of FM. However, alongside these benefits are the adverse effects of the medications which may include mild to severe: dizziness, weight gain, nausea, and insomnia. The effectiveness of pharmacological methods is approximately 30% symptom reduction, stated by Staud and thus these methods are often combined with other therapies (Staud, 2010). TENS Transcutaneous Electrical Nerve Stimulation (TENS) is a therapy form that electrically stimulates the skin in order to provide “descending inhibition” pain control. Nociceptive neurons, or pain receptors, are inhibited by the activation of descending inhibitory pathways from the midbrain brainstem. This means that pain coming from pain receptors does not make it to the brain. Noehren notes that TENS best inhibits pain associated with ongoing noxious stimuli such as movement but is less effective in curbing pain at rest. This is significant to improve quality of living and to decrease pain associated with functional activities, when used appropriately (Noehren et al., 2015). For best results TENS should be applied daily over a long period of time. The amount of time TENS should be applied varies and can range from less than one hour to several hours per day. Dailey concluded that the pain relief is most significant during the active TENS or directly after, with pain levels returning to 8 R. Gorgitza normal post-treatment (2013). Kaye has stated that in the beginning stages of treatment, TENS can decrease pain by up to 80%, however, this rate of effectiveness decreases over a period of a few months. (2002) Physical Activity Physical training is yet another alternative therapy for fibromyalgia. Physical training encompasses a wide variety of aquatic or land-based strengthening, stretching, aerobics, balance and postural exercises. It can improve quality of life by decreasing fibromyalgia symptoms, as well as improving overall fitness. Different exercise groups can affect different changes: for example, research has associated strength training with improved well-being and physical function whereas a combination of different forms of exercise decreased pain and improved physical function. The number of tender points a patient has as well as the intensity of pain experienced can be decreased by an appropriate physical training program, and the benefits reaped have been noticed to remain for up to 4 months post training (Dragoi et al., 2012). A wide array of activities have been studied and suggested to have positive impact on people suffering fibromyalgia. Bursch found that aerobic and strength exercise plans as well as Pilates were most beneficial with fibromyalgia though other forms are effective as well (2011). It is also stated that fibromyalgia 9 R. Gorgitza patients are generally able to do moderate to vigorous levels of activity, but they may have difficulty adhering to such programs due to pain and other symptoms. Unique fitness programs must be created for each specific person based on case history in order to avoid adverse effects. Despite all the benefits shown, adverse effects such as musculoskeletal complaints and exacerbations of symptoms such as pain, stiffness, and fatigue are not uncommon with these types of therapy. Physical training, much like the other therapies described above, is often used in conjunction with other types of treatments. (Gowans et al., 2013) Massage Therapy The effects of massage therapy on fibromyalgia patients are also in question. Not a lot of research has been done on this topic, and it is difficult to group all such studies together as the techniques and modalities used are so varied. For the purpose of this study, lymphatic drainage will be the main focus. The application of lymphatic drainage defined as light, repetitive techniques used to pump lymph fluid through superficial lymphatic capillaries. Each manipulation must be repeated 5+ times, strokes must be towards the heart, and the principle of ‘proximal to distal’ must be used in order for this technique to be most effective. No oil is required for this technique because it relies on the drag of the skin under a pressure of approximately 20-40mmhG to pump the fluid 10 R. Gorgitza and not collapse the vessels. Greater pressure can collapse the superficial vessels and momentarily prevent drainage. (Rattray, 2000) Direction of Lymphatic Flow in the Bodyimage b Typically this modality is used to treat edema and swelling related to trauma or post-surgery in order to reduce the formation of scar tissue. Lymph drainage is also effective in decreasing pain perception via gate-control pain inhibition. It affects the nervous system by inhibiting firing of the sympathetic nervous system, promoting relaxation and allowing for a faster healing rate. It is known to help regulate the immune system, clear blockages, eliminate metabolic waste and toxins from the body. This explains why increased urine output with 11 R. Gorgitza high concentrations of inflammatory and pain mediators excreted post-treatment has been noted. (Rattray, 2000) However, there are contraindications. Lymphatic drainage would not be appropriate for a patient with edema due to heart failure or thrombosis, bacterial, viral, or fungal infection, or lymphatic obstruction by parasite. Special care must be taken when working with patients who have had lymph nodes removed, or who suffer from conditions (eg. toxoplasmosis, sinusitis, bronchitis) which may be flared up by this technique. This technique is not effective for those with lowprotein edemas (eg. edemas caused by liver or kidney pathologies). Lymphatic drainage should only be performed proximally and locally to the edemous region; any distal work is contraindicated. These cautions do not directly apply to fibromyalgia; however, they must be taken into account with every patient. Ekici’s comparison study has shown the Vodder’s Method MLD was more effective in decreasing fibromyalgia symptoms such as anxiety, fatigue, stiffness, and pain than the deeper connective tissue massage also studied (2009). Participants receiving MLD reported feeling more well-rested upon waking in the morning as well as being less tense and less anxious. Lymphatic drainage affects the physical pain suffered by fibromyalgia patients as well as the fatigue and secondary symptoms. Adverse effects of this treatment, however, are the sensation of nausea, feeling ill, and increased frequency of urination. More 12 R. Gorgitza research is needed in this field to determine the longevity and quality of the benefits (Ekici et al., 2009). In conclusion, several studies have been completed on each of these forms of therapy though very few solid outcomes have been reached. It seems that a combination of these therapies gives the best results and is most often used clinically. The effect of lymphatic drainage on fibromyalgia symptoms seems to be a subject with the least amount of research of all topics reflected upon. This has led to the goal of this study: to collect information on whether lymphatic drainage is a successful symptom management technique for fibromyalgia. 13 R. Gorgitza METHODS Study Design: This is a case study which began October 12, 2014 wherein case history was collected and an initial relaxation massage was provided to the participant. The participant filled out measures forms beginning in October, 2014, throughout the active intervention, and into February 2015. The intervention of lymphatic drainage was applied for an 11-day period from December 20, 2014 to January 1, 2015, with one-hour long appointments every other day. A total of 7 treatments were applied including the initial full body relaxation massage. Only data collected during the December-January treatment period are used in this study. Participant: The participant was selected based on a convenience sample of women diagnosed with fibromyalgia and known to the researcher. Those with active treatment of the disorder and incompatible schedules for the study were ruled out. The participant was selected in July, 2014 when the study’s procedures, requirements, benefits and risks, were outlined, and questions were answered. An informed consent form was signed. Criteria of the chosen participant are that she is 58 years old, a non-smoker, rarely takes pain medication, and has a moderate 14 R. Gorgitza and consistent level of activity and a balanced diet. She was first diagnosed with FM in 1985 after a work-related accident in 1984 and was unable to return to her job as a flight attendant. She suffered severe back and leg pain, joint pain, neck and head pain, insomnia, exhaustion, fatigue, anxiety, and depression. In 1993, she was re-diagnosed by another rheumatologist after an emergency C-section. Interventions between 1985– 1993 included physiotherapy, TENS, drug therapy, counselling for chronic pain, chiropractics, naturopathy, dietary changes, massage and relaxation techniques. After 1993, she was unable to access the intervention services because of where she lived. She relied on what she had learned in previous interventions and found relief with light exercise, nutrition, warm baths, and drug therapy. She has never returned to work, has good days and bad, feels limited by body pain and lack of sleep, and is frustrated with the condition. With this therapy the patient is looking for relaxation and less pain. Outcome Measures: Primary Outcome: The primary outcome measured was the number of painful body regions. Secondary Outcome: The secondary outcomes measured were the number of secondary fibromyalgia symptoms including fatigue, cognitive function, and more. 15 R. Gorgitza During the active intervention, the participant’s subjective opinion on amount of sleep and overall well-being was recorded before each treatment. Pain, on a 1-10 scale, in the participant’s current area of complaint was recorded preand post-treatment. Measurement Instruments The American College of Rheumatology’s diagnostic form for fibromyalgia was used to collect data. The form is a two-sided page with a Widespread Pain Index (WPI) and a two-part Symptom Severity score (SSa and SSb). The WPI and SSa, as well as the pre-treatment interview, were used to collect data regarding the number of painful body parts and the severity of that pain. Both parts of the SS were utilized to gather data about the secondary outcomes. At the end of each section of the form was a tally box to be used by the patient to determine their ‘score’; the participant of this study was requested to leave those boxes blank to allow the researcher to interpret the information. 16 R. Gorgitza 17 R. Gorgitza The WPI and SS form image c Control: As this study does not include a separate control group, the participant’s past history is used as the comparison. The participant was asked a series of questions on her “norm” during the initial case history and treatment on October 12, 2014. She was also required to fill out the measurement forms weekly from October 3, 2014 until the beginning of the study December 21, 2015 to provide baseline information. Prior to and directly after each treatment session the participant was interviewed for approximately 5 minutes and filled out a measurements form. Twelve hours after the intervention was applied, the participant was asked to 18 R. Gorgitza answer each of the questions on the measurements form again, and the therapist recorded the data. Lymphatic Drainage Intervention: This intervention was provided by the author of this study after learning the application of lymphatic drainage in a series of three 4-hour long classes and several practical applications outside of the classroom. The lymphatic drainage technique uses techniques described in Rattray (2000). This intervention was to be applied every other day from December 21 until January 1, with a total of 6 treatments. For scheduling reasons, one of the treatments was spaced 2 days from the previous. The therapeutic goals of this treatment series were as follows: 1. Promote parasympathetic nervous system firing to encourage restful sleep at night 2. Promote lymphatic flow/drainage to improve removal of metabolites from tissue and decrease pain To achieve these goals deep diaphragmatic breathing techniques as well as a variety of lymphatic drainage techniques were used. Each of the treatments was 60 minutes in length, and it began with the participant practicing deep diaphragmatic breathing while the therapist applied terminus pumping. Terminus 19 R. Gorgitza pumping is the gentle press and release across the upper chest where the left and right thoracic lymphatic ducts converge with the left and right subclavian vein. Gentle nodal pumping was applied before addressing the limb distally. After terminus was pumped, the sequence nodes pumped and body parts addressed is as follows: Nodes Regions addressed Cervical anterior cervical region, face, head Axillary anterior chest, upper arm Cubital forearm, hands Upper abdomen Inguinal Popliteal Lower abdomen, anterior and posterior Location of Lymphatic Structures in the thigh, shin Bodyimage d Calves Sacrum, sacral pumping Lower, middle, upper back, posterior cervical region 20 R. Gorgitza The principles of addressing lymph nodes before limbs and working proximal to the node before distal were followed. Each section of the body was addressed with stationary circles and local techniques. These modalities Stationary circles are used to treat large surface areas. The palm and fingers of one or both hands gently press and release in a circular motion. Pressure is applied in the direction towards the lymph node or “upstroke,” and released on the “downstroke.” were repeated 2-4 times per area. For example, when addressing the arm, the axillary nodes of that arm were pumped, stationary circles and local techniques were applied sequentially from the shoulder to the elbow. Then, the techniques were repeated, starting again at the shoulder and working towards the elbow, and so on, before moving to the cubital nodes and lower arm. This process was used for all regions of the body addressed. Local techniques: Use of the web of the hand is used for smaller limbs or distal portions of limbs. The webspace between the thumb and index finger of the therapist’s hand softly wraps around the limb, and strokes upwards. Double handed webspace can be used for larger limbs. Use of the broad surfaces of the thumbs is similar to “stationary circles” on a smaller scale. After each treatment, as homecare, the participant was assigned a warm Epsom salts bath for approximately 20 minutes. 21 R. Gorgitza OUTCOMES Figure 1 (WPI Scores) Figure 1, on the left, compares the baseline WPI measurements taken in the 12 weeks prior the intervention with the follow-up measurements taken in the 5 weeks after the intervention ended. Pre-intervention, it can be seen that there are many peaks and valleys in the number of painful areas, with the longest period of consistency being 3 weeks. During the follow-up a more consistent and lower number of painful regions were noted. On the right side of Figure 1, the measurements taken each treatment during the 2-week intervention period are described. During this time, the highest WPI score remained the highest and most variable of the three assessment times, 22 R. Gorgitza with an average of 10. Directly post intervention as well as 12 hours after, an average score of 8 was recorded. The overall trend of Figure 1 shows a decrease in the number of painful areas recorded through the process of the intervention, and from before to after the intervention was applied. Figure 2 (SSa Scores) As seen in Figure 2, across the 19 weeks of data collection, the lowest levels of fatigue, cognitive symptoms, and unrefreshed waking were recorded during the intervention (weeks 13 and 14), and after the intervention (weeks 1519). Cognitive symptoms remained consistently low post-lymphatic drainage application, dropping from an average score of 2 (moderate, considerable, often problems), to an average of 1 (slight, mild, or intermittent problems). However, fatigue and unrefreshed waking levels dropped during the intervention weeks and spiked again in the weeks following. 23 R. Gorgitza Figure 3 (SSa Scores) A further breakdown of the SSa data taken during the treatment period is shown in Figure 3. After the first treatment, the overall level of cognitive symptoms before and after treatments decreased to a score of 1 (slight, mild, or intermittent problems). After two sessions, fatigue levels consistently remained at a score of 1. From the 4th session on, the level of waking unrefreshed remained at a score of 1. Waking unrefreshed was only measured pre-session, based on the participants experience waking that morning, and 12 hours post-session based on waking the day after the treatment. The 5th session was performed in the morning, so only a pre-intervention measurement was taken. 24 R. Gorgitza Figure 4 (SSb Scores) The top graph Figure 4, the number of symptoms in relation to the weeks of data collected is shown. The average number of symptoms experienced in the weeks prior to intervention is 15.75, decreasing to 11 during treatments, and post intervention is 11.4. On the bottom, is a further breakdown of symptoms experienced at each treatment session. The average number of symptoms is highest pre-treatment, 12.5, whereas directly after treatment the average is 7.7, and 7.3 twelve hours later. 25 R. Gorgitza DISCUSSION This study explored whether lymphatic drainage is an effective symptom management technique for fibromyalgia. Measurements of the number of painful regions (WPI score), severity of symptoms (SSa), and number of symptoms (SSb) related to fibromyalgia were recorded before, during, and after the intervention was applied, and this data was compared. Shown in the results section is an overall decrease of the average WPI, SSa, and SSb scores once the treatment sessions began in comparison to the 12 weeks prior to treatment. This information is supported by the results obtained in Ekici’s study (2009). However, the participant had ended a series of chiropractic appointments just prior to beginning the intervention but after submitting the pre-intervention questionnaires. This decreased strain on the body could also have an effect on the level of symptoms. Since the improvement in condition occurred over a period of a couple lymphatic drainage treatments, though, it is likely related to the study intervention. The decrease in fibromyalgia symptoms remained for at least 5 weeks after the intervention period ended. Data was only collected for 5 weeks postintervention, and so long-term impact of the treatments can’t be discussed. In order to better understand the impact of this study, data could have been collected during equal lengths of time pre- and post-intervention. 26 R. Gorgitza Despite the improvement in symptoms overall, the treatments caused the participant an increase in discomfort directly after sessions. She reported feeling groggy, tired, dizzy, nauseous, and/or “mucousy” post-treatment, making it difficult to fall asleep. These are common adverse effects of lymphatic drainage. She indicated she felt better and slept longer the night after a morning treatment rather than after the evening sessions. This should be taken into consideration for further research. However, her subjective pain levels also decreased after each session compared the pre-treatment. To expand this research, a more formal set-up of recording subjective pain levels could have been used. This study relied completely on the WPI and SS form, and an interview provided by the practitioner. The interview questions were inconsistent, and so the data regarding pain levels, hours of sleep per night, and quality of life have been eliminated from this study. A Visual Analog Scale (VAS) to measure pain, and a selection of questionnaires on sleep, depression, activity levels could be used to determine level of quality of life, thus giving a clearer look into the impact of lymphatic drainage massage on this condition. 27 R. Gorgitza CONCLUSION Lymphatic drainage may be helpful in the management of fibromyalgia symptoms, specifically the number of painful areas associated with the conditions as well as the number and severity of secondary symptoms. However, this information is case-specific, and more research needs to be done to confidently state the external validity of this symptoms management method. 28 R. Gorgitza REFERENCES 1 Alnigensis, M., Bradley, J., Wallick, J., Emsley, C. Massage Therapy in the Management of Fibromyalgia: A Pilot Study. (2001). Journal of Musculoskeletal Pain, 9(2), 55-67. Retrieved February 8, 2014, from EBSCOhost. 2 Bursch, A., Webber, S., Brachaniec, M., Bidonde, J., Dal Bello-Haas, V., Danyliw, A., . . . Schachte, C. (2011, July 5). Exercise Therapy for Fibromyalgia. Retrieved November 13, 2014. 3 Crofford, L. (2013, January 1). Fibromyalgia. Retrieved September 22, 2014, from https://www.rheumatology.org/Practice/Clinical/Patients/Diseases_And_Conditio ns/Fibromyalgia/ 4 Dailey, D., Rakel, B., Vance, C., Liebano, R., Amrit, A., Bush, H., . . . Sluka, K. (2013). Transcutaneous electrical nerve stimulation reduces pain, fatigue and hyperalgesia while restoring central inhibition in primary fibromyalgia. Pain, 154, 2554-2562. Retrieved March 17, 2015, from EBSCOhost. 29 R. Gorgitza 5 Dragoi, D., Traistaru, R., Rosulescu, E., Vasilescu, M., Matei, D., & Popescu, R. (2012). A 12-week physical training program – effects on fibromyalgia patients. Medicina Sportiva (2012), VIII(1), 1769-1774. Retrieved November 13, 2014, from EBSCOhost. 6 Ekici, G., Bakar, Y., Akbayrak, T., & Yuksel, I. (2009). COMPARISON OF MANUAL LYMPH DRAINAGE THERAPY AND CONNECTIVE TISSUE MASSAGE IN WOMEN WITH FIBROMYALGIA: A RANDOMIZED CONTROLLED TRIAL. Journal of Manipulative & Physiological Theraputics, 32(2), 127-133. Retrieved November 24, 2014, from EBSCOhost. 7 Gaufin, J., Hankama, T., Hannonen, P., Kautiainen, H., Pohjolainen, T., & Haanpää, M. (2013, May 1). DO FIBROMYALGIA PATIENTS USE ACTIVE PAIN MANAGEMENT STRATEGIES? A COHORT STUDY. Retrieved September 22, 2014, from http://www.medicaljournals.se/jrm/content/?doi=10.2340/165019771133&html=1 30 R. Gorgitza 8 Gowans, S., DeHueck, A., Voss, S., & Richardson, M. (1990). A randomized, controlled trial of exercise and education for individuals with fibromyalgia. Arthritis Research and Therapy. Retrieved March 16, 2015, from EBSCOhost. 9 Kaye, V. (2002). Transcutaneous Electrical Nerve Stimulation. EMedicine Journal, 3(1). Retrieved March 10, 2015, from http://emedicine.medscape.com/article/325107-overview 10 Kim, S., Landon, J., & Lee, Y. (2003). Patterns of health care utilization related to initiation of amitriptyline, duloxetine, gabapentin or pregabalin in fibromyalgia. Arthritis Research and Therapy, 17, 18-18. Retrieved March 8, 2015, from EBSCOhost. 11 Noehren, B., Dailey, D., Rakel, B., Vance, C., Zimmerman, M., Crofford, L., & Sluka, K. (2015). Effect of Transcutaneous Electrical Nerve Stimulation on Pain, Function, and Quality of Life in Fibromyalgia: A Double-Blind Randomized Clinical Trial. Physical Therapy, 95(1), 129-140. Retrieved February 2, 2015, from EBSCOhost. 31 R. Gorgitza 12 Rattray, F., & Ludwig, L. (2000). Clinical Massage Therapy: Understanding, Assessing, and Treating Over 70 Conditions (pp. 35-37, 217-220, 224, 981-986). Elora, Ontario: Taluls Incorperated. 13 Staud, R. (2010). Pharmacological Treatment of Fibromyalgia Syndrome: New Developments. Retrieved December 8, 2014. 14 Theadom, A., & Cropley, M. (2010). ‘This constant being woken up is the worst thing’ – experiences of sleep in fibromyalgia syndrome. Disability and Rehabilitation, 32(11), 1939-1947. Retrieved March 8, 2015, from EBSCOhost. Images in order of appearance image a (n.d.). Retrieved April 9, 2015, from http://physioworks.com.au/images/InjuriesConditions/Fibromyalgia.png?bc_t=NlThhdnKeLS/hzcn0sWNWQ, April 9, 2015 image b What is Lymph Drainage. (n.d.). Retrieved March 13, 2015, from http://www.lymphdrainage.com.au/what-is-lymph-drainage-therapy.html 32 R. Gorgitza image c New Clinical Fibromyalgia Diagnostic Criteria. (2010, February 23). Retrieved October 1, 2014, from http://www.sdhct.nhs.uk/patientcare/proformas/pain/questionnaire - widespread pain index and symptom severity score.pdf image d Lymph Nodes and Cancer: What is the Lymph System? (2013, January 1). Retrieved March 8, 2015, from http://www.cancer.org/acs/groups/cid/documents/webcontent/~export/ACSPC030892-CLEAN~4~DYN_ACS_CID_TEMPLATE/178262-1.gif 33 R. Gorgitza