Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
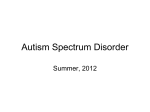
COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS i490318 Karen Hopmann Th. Widdings Veg 50 N - 9020 Tromsø [email protected] Cognitive and Emotional Processing of Social Stimuli in Students with Autistic Traits An EMG Study Words: 9164 01.06.2012 Master Thesis Neuropsychology Experimental Research Maastricht University (UM) Faculty of Psychology & Neuroscience Internship at: Universitetet i Tromsø (UiT) – Institute of Psychology Supervisors: Ole Åsli (UiT), Hans Stauder/Petra Vlamings (UM) COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS Content Abstract ................................................................................................................................................... 3 Acknowledgements ................................................................................................................................. 4 1 Processing of Social Stimuli in Autism Spectrum Disorder................................................................. 5 1.1 Autism Spectrum Disorder ............................................................................................................ 5 1.1.1 Autistic phenotype. ................................................................................................................. 8 1.1.2 Facial processing in ASD. .................................................................................................... 11 1.2 Startle Eyeblink Response ........................................................................................................... 12 1.3 Hypotheses .................................................................................................................................. 14 1.4 Relevance .................................................................................................................................... 15 2 Method ............................................................................................................................................... 16 2.1 Participants .................................................................................................................................. 16 2.2 Materials ...................................................................................................................................... 16 2.2.1 EMG/picture presentation. ................................................................................................... 16 2.2.2 SAM/VAS subjective measure. .............................................................................................. 17 2.2.3 Autism spectrum quotient questionnaire. ............................................................................. 18 2.3 Procedure ..................................................................................................................................... 18 2.4 Apparatus and EMG .................................................................................................................... 19 2.5 Data Analysis .............................................................................................................................. 19 3 Results ................................................................................................................................................ 20 3.1 Autism Spectrum Quotient Questionnaire................................................................................... 20 3.2 Ratings ......................................................................................................................................... 20 3.3 Startle Eyeblink Response ........................................................................................................... 21 4 Discussion .......................................................................................................................................... 22 4.1 Hypotheses revisited.................................................................................................................... 23 4.2 Limitations .................................................................................................................................. 25 5 Conclusion .......................................................................................................................................... 27 References ............................................................................................................................................. 28 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS Abstract Autism spectrum disorder (ASD) is a pervasive developmental disorder that becomes apparent early in an individual’s lifetime. As the name of the disorder indicates, autistic symptoms occur on a spectrum. Less severe expressions of the symptoms can arise in a normal student population, showing autistic traits. The current study investigated cognitive and emotional processing of facial stimuli in a group of students scoring high (n = 12) versus low (n = 16) on a test of autistic traits, the Autism Spectrum Quotient Questionnaire (AQ). To test this, the startle eyeblink response, elicited by a white noise while watching pictures of faces, was recorded with electromyography (EMG). No differences in startle eyeblink response to facial stimuli between individuals scoring high and low on the AQ were found. Moreover, a subjective test of arousal and valence revealed no differences between the groups. For the EMG measure, the different emotions led to differences in startle eyeblink responses. Here, fearful faces presented frontally elicited higher startle response magnitude than frontally displayed angry faces and neutral faces presented from a 45° angle. In addition, the angle of picture presentation exposed a significant difference, with frontally presented pictures eliciting higher startle eyeblink responses than presentation from the side. It is concluded that fear reactions in individuals with high autistic traits are comparable to those of the control group. Keywords: Autism spectrum disorder (ASD), social stimuli, fear, autistic traits, startle eyeblink response COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS Acknowledgements I would like to thank my supervisor at Tromsø University, Ole Åsli, whose encouragement, guidance and support from the initial to the final level enabled me to develop an understanding of the subject. He has shown his support in a number of ways, starting with laboratory instructions, guidance with writing, and last but not least given great support with statistical analyses. Furthermore, giving me free rein to execute all laboratory work helped a lot to develop independence in my work. Also, I want to thank my supervisor at Maastricht University, Petra Vlamings, for her support regarding background knowledge of ASD. I appreciate the help and support, especially when the current topic had to be changed, and her knowledge of the current field of study. My thanks go to Hans Stauder at Maastricht University for taking over for Petra Vlamings without hesitation, when she was not able to supervise my work anymore. Without his effort, a smooth delivery of my thesis would not have been possible. Finally, I offer my regards to all of those who supported me in any respect during the completion of the project, most especially to my family and friends. Karen Hopmann COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS 1 Processing of Social Stimuli in Autism Spectrum Disorder Flo and Kay Lyman, born in New Jersey in 1956, are the only known female savant autistic twins in the world. Diagnosed with autism spectrum disorder, they have experienced a lot of harassment throughout their lives. However, these twins seem to be unique in a lot of ways. Flo and Kay can remember every day in detail since adolescence. They know what they had for dinner or what the weather was like of any given day in the past. Asked which day of the week it was on November 30th of 1938, they answer correctly that it was a Wednesday, although they were not even born at that time. Their mental abilities and memories appear to be special; however, the disorder of autism restricts them in their social acts. Flo and Kay need routines, they live for themselves following the same patterns each and every day. They seem to be absurdly obsessed with TV-star Dick Clark. The twins know about their difficulties, but manage their lives in their own ways and appear happy and resilient. (Retrieved April, 11, 2011, from http://splicetv.com/work/clients/flo_and_kay_twin_savants.html; http://www.examiner.com/article/flo-and-kay-twin-autistic-savants) This case of two very special autistic women is a good example of the unique nature of the disorder of autism. Savants are rare, yet most commonly observed in developmental disorders like autism. These individuals have abilities which seem genius to a normal healthy person, such as recalling accurate dates and events. Nevertheless, something that appears to be a unique gift for someone can equally have severe consequences for the person concerned. Autism spectrum disorder (ASD) is a heterogeneous syndrome restricting an individual’s life in many aspects. 1.1 Autism Spectrum Disorder In 1943, Leo Kanner made the first diagnosis of ‘infantile autism’ (Volkmar, State, & Klin, 2009). Symptoms such as social impairments, repetitive behaviors, and difficulties with language were described as the core symptoms (McIntosh, Reichmann-Decker, Winkielman, & Wilbarger, 2006). However, the most noticeable sign was the “pervasive lack of interest in other people, including their parents” (Klin & Volkmar, 1999, p. 248). Since then, diagnostic tools, classifications, and different expressions of the disorder have been further developed and explored. Nowadays, the syndrome is known under the overall term autism spectrum disorder (ASD). The spectrum comprises many forms of symptom manifestations, varying 5 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS from severe limitations in daily functioning to less severe forms of the disorder. Approximately 1 in 100 children and adolescents are affected by the disorder today, many more than originally assumed (Charman et al., 2011). Boys tend to be four to five times more frequently affected than girls, while female patients generally suffer from more severe forms of ASD (Klin & Volkmar, 1999). While the basic symptoms described by Kanner around 70 years ago are generally still applicable, such as the lack of social interactions, problems with communication, the expression of repetitive behaviors, as well as the differentiation from schizophrenia, some are now proven to be wrong. For instance, it has been established recently that parenting has rather small to no influence on the development of autism, which is in contrast with Kanner’s original suggestion that parents influence the syndrome pathogenesis (Klin & Volkmar, 1999). Moreover, Kanner falsely claimed that children suffering from infantile autism are principally clever rather than mentally retarded. Today it is known that about half until up to three-quarters of the autistic population have an IQ below 70. This demonstrates a connection to syndromes like mental retardation (Barlow & Durand, 2002; Charman et al., 2011). Furthermore, Charman et al. (2011) imply that especially verbal IQ is much lower in autistic individuals in comparison to rather preserved performance IQ. This stands in contrast to what was previously assumed. Therefore, the connection between use of verbal assessment forms of IQ and communication problems in autistic individuals should be accounted for and needs further investigation. The spectrum comprises a large scale of symptom expressions. Five subtypes of ASD are described by the DSM-IV-TR, shown in figure 1. These include Asperger’s syndrome, autistic disorder, Rett’s disorder, childhood disintegrative disorder, and unspecified subtypes (pervasive developmental disorder not otherwise specified, PDD-NOS). PDD-NOS encompasses the largest amount of affected individuals (Barlow & Durand, 2002; Golaria, Grill-Spector, & Reiss, 2006; Volkmar et al., 2009). Comorbidity is very common in individuals with ASD and more than half of the affected patients additionally suffer from an intellectual disability or experience other psychiatric problems (Charman et al., 2011). 6 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS Autism spectrum disorder Autistic Disorder Rett's Disorder Childhood Disintegrative Disorder Pervasive Developmental Disorder, Not Otherwise Specified Asperger's Syndrome Figure 1: The five subtypes of ASD as defined by the DSM-IV-TR (APA, 2000). Along these lines, often mistakenly called autism, ASD is a pervasive developmental disorder, characterized by expression of stereotyped behaviors, and impairments in non-verbal communication skills and social interactions (American Psychiatric Association, 2000). However, symptoms are extremely heterogeneous throughout the group of patients. Difficulties, for example in executive functions, are recognized to be apparent, yet not globally evident (South, Larson, Krauskopf, & Clawson, 2010). South et al. (2010) explain this by the fact that inconsistent findings are common in a young field of research such as autistic examinations. This heterogeneity has lead to further uncertainties in the description of the causes of ASD. There is convincing evidence to believe in a genetic predisposition of autism spectrum disorder. In case of having one child suffering from ASD, the chance that siblings are affected lies at about three to five percent, although they are often suffering from milder forms of the disorder (Barlow & Durand, 2002; Rutter, 2006). This supports the theory that certain genes are responsible for the development of ASD (Rutter, 2006; Volkmar et al., 2009). Yet, the exact genes involved in the development of the disorder still need to be investigated. ASD certainly is a disorder with many facets, and environmental factors are additionally influencing the development. However, empirical support in the area of pathogenesis is very rare, and symptom expression varies from individual to individual. The former suggestions of parental influence, such as nurturing style, socioeconomic status, and causation through vaccination, could furthermore not be confirmed in later studies (Barlow & Durand, 2002; Klin & Volkmar, 1999; Rutter, 2006). While the causes are relatively unknown, a reliable diagnosis can nowadays be made already at an early age. Such early diagnoses were much less common a generation ago, when 7 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS ASD was mostly not recognized before children attended school (Rutter, 2006). Diagnoses are mostly done by a pediatrician using specialized diagnostic tools. These include specific scales which are appropriate for the assessment of ASD, such as the Autism Diagnostic Observation Schedule (Volkmar et al., 2009). Four major components are important for a successful diagnosis of ASD. These components comprise an early onset, dysfunctions in social interactions and symbolic play, communicative problems, and stereotyped behaviors with resistance to change (Klin & Volkmar, 1999). These are consistent with the typical symptoms described in the DSM-IV-TR. With doctors and psychologists being more familiar with the disorder and diagnostic tools getting more advanced, an early diagnosis can be made more easily (Rutter, 2006). The treatment, as much as the knowledge about the origin of the disorder, is still in its fledgling stage. Different therapies exist, including behavioral and social therapy, as well as pharmacological interventions. As up to three-quarters of the autistic population have an IQ below 70, there are vast parallels between pervasive developmental disorders and individuals who are mentally retarded (Barlow & Durand, 2002). Consequently, the treatment has some overlap. As in mentally retarded individuals, no treatment until now can promise to restore complete health, and can only improve the situation for the affected patients. Behavioral therapies commonly aim at improving the integration into social life and reducing stereotyped and repetitive behaviors, likewise improving communicative skills (Klin & Volkmar, 1999). It is important to give social treatment frequently and start early with interventions to achieve the best possible outcome (Barlow & Duran, 2002). While psychosocial and behavioral treatment seems to improve some of the symptoms, the effectiveness of medication could not be successfully proven. In particular, the heterogeneity of the disorder causes problems, because no single drug can cure all of the symptoms of ASD in any given individual. Special dietaries, vitamins, and some forms of medical treatment were used in the past, but did not show significant effects. Pharmacological treatment might only help to reduce some symptoms, and merely on a temporary basis (Barlow & Durand, 2002). 1.1.1 Autistic phenotype. The name autism spectrum disorder alone implies a heterogeneous nature of the disorder, with many aspects of symptom expression. Asperger’s syndrome, for example, is often specified as a case of less severe autism, even though this generalization does not meet the whole truth. However, patients suffering from Asperger’s syndrome generally have a higher average IQ with preserved higher communication skills and fewer problems restricting 8 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS normal living (Volkmar et al., 2009). They do, in spite of this, have problems with social interactions and often need to follow routines, sometimes expressing abnormal patterns of behavior. As language abilities are generally preserved, a less severe perception of the autistic symptoms is common (Barlow & Durand, 2002). One example is that professors or other intellectual people diagnosed with ASD are mostly suffering from a form of Asperger’s syndrome. This indicates that also in a student population, autistic traits or cases are present. Moreover, Barlow and Durand (2002) state that Asperger’s syndrome is often not diagnosed, hence not recognized, indicating the presence of autistic symptoms in the normal population. Furthermore, it is claimed that the spectrum of ASD can reach into the non-clinical population, thus suggesting autistic traits in the neurotypical population (Suda et al., 2011). Especially individuals with a family history of ASD or siblings diagnosed with some sort of autistic disorder, have a greater chance to experience symptoms. Nevertheless, these symptoms are generally less severe in siblings (Rutter, 2006). Due to this, there is a great chance of finding an autistic phenotype in everyday life, such as in a student population on university campuses. Particularly, students at faculties of natural sciences, such as mathematics, physics and others, have been found to have a higher possibility of scoring in the upper range when tested for autistic traits. One of those questionnaires testing for autistic traits is the Autism Spectrum Quotient Questionnaire (AQ; Baron-Cohen, Wheelwright, Skinner, Martin, & Clubley, 2001). With the AQ, a range of domains - such as social problems - common for ASD can be assessed. Individuals scoring high on the AQ are seen to have higher autistic traits. Ridley, Homewood, and Walters (2011) examined the performance on motor and verbal tasks and found a correlation between motoric problems and higher scores on the AQ, indicating a cerebellar dysfunction in people with autistic traits. They claimed that these findings point toward an autistic spectrum or continuum reaching into the non-clinical population, including the students tested in their study. An autistic phenotype exists both in the clinical and non-clinical population. In accordance with the assumption of South, Ozonoff and McMahon (2005) that patients with Asperger’s syndrome and high-functioning autistic individuals can develop special interests in the field of natural sciences, it is of high interest for the present study to find participants interested in natural sciences. Especially students of mathematics, physics and similar subjects will possibly contribute to a higher representation of the autistic phenotype in a non-clinical population. The higher prevalence of autistic traits in these fields of studies can be explained by the fact that autistic traits are often manifested in a greater interest or focus on details instead of social interactions or information processing as a whole. 9 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS There appears to be an overall interest in the natural, instead of the personal, environment (Ridley et al., 2011). Another explanation can be given by the ‘extreme male brain’ (EMB) theory of autism by Baron-Cohen (2002), stating that an autistic brain might be “an extreme of the normal male profile” (Suda et al., 2001, p. 7). Generally, there is a higher prevalence of autistic traits in the neurotypical male population in contrast to females, supporting the EMB theory. The study by Suda et al. (2011) showed that in face-to-face conversation a female brain shows additional activation in the superior temporal sulcus, where empathy is recognized; whereas male brains tend to show activation in the prefrontal cortex only - thus in the planning or systemizing part. Given these outcomes, it can be theorized that male brains are often more systematically driven than female brains. Precisely that is also stated by the empathizingsystemizing (E-S) theory (Baron-Cohen, 2005). The E-S theory states that the female brain is “predominantly hard-wired for empathy and that the male brain is predominantly hard-wired for understanding and building systems” (Baron-Cohen, 2005, p. 23). According to this theory, there are three types of brains. The first one is the female or empathizing brain (type E), the second one a male or systemizing brain (type S), and a third type, called the balanced brain (type B), which comprises characteristics of both types. These categorizations and typical preferences are already present in infants (Baron-Cohen, 2005). Combining this theory together with the EMB theory, the higher rate of autistic traits in individuals studying systematic studies can be explained. Furthermore, in accordance with the EMB theory, different studies also confirmed higher scores on the AQ in students of mathematics, physics or engineering in comparison to students of humanity studies (Baron-Cohen et al., 2001). In the study by Baron-Cohen et al. (2001), students of so-called systematic studies were much more likely to reach a higher score on the AQ. Ridley et al. (2011) found a mean AQ score of 19.59 in systematic studies, compared to only 13.47 in students of humanities. This clearly supports the importance of finding participants in the field of natural science studies, as these individuals might be representing the autistic phenotype reaching into the normal population. In sum, autistic traits can be found everywhere in the population, clinical or not. Nevertheless, defining an autistic phenotype is a rather complicated matter. As well as the whole spectrum disorder, the phenotype is of vast heterogeneity. Charman et al. (2011) point out the important role of identifying the connection between heritability, neurocognitive and biological development, and the behavior of the patient. Combined, this would lead to a better understanding of the autistic phenotype. Moreover, identifying the different subtypes of the spectrum is of great importance. Not only cognitively autistic individuals vary a lot, as in for 10 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS example intelligence, but also their behaviors show immense diversities. Future studies must concentrate on further investigation of the autistic phenotype and its expression, both cognitively and behaviorally (Charman et al., 2011). 1.1.2 Facial processing in ASD. Individuals suffering from autism spectrum disorder are restricted in their daily routines in many ways. While some forms are rather mild, others can be extremely severe, resulting in total isolation of the patient. Especially families and caregivers will experience difficulties, as verbal and social interaction with the patient can be frequently impossible. Since these deficits occur early in a patient’s life, a lot of symptoms are already apparent before a diagnosis can be made. One of the characteristic symptoms is the general avoidance of social and facial stimuli. In their 2005 study on gaze fixation, Dalton and colleagues came to the conclusion that individuals with ASD show diminished gaze fixation and avoid looking at faces. This, in turn, leads to overall less eye contact and diminished social interactions. Different models have been proposed to explain the deficit in facial processing of autistic individuals. In their article, Golarai, Grill-Spector, and Reiss (2006) introduce three models explaining the facial processing deficit of individuals suffering from ASD. The first model describes the phenomenon by a bottom-up effect caused by difficulties in low-level visual processing, for example motion processing. This inability to process movements accurately leads to problems in facial processing. A second model explains the deficit as a consequence of a selected top-down ignorance and disinterest in human interaction. A third more neurological - model suggests that the responsible brain areas for facial processing are less developed as a consequence of a smaller amount of time spent viewing faces. This could have occurred due to either a bottom-up or a top-down effect. Additionally, a study in Cambridge discovered that babies with lower levels of testosterone, as well as individuals with a type E - hence ‘female’ - brain, show higher levels of eye contact (Baron-Cohen, 2005). This finding supports a connection between diminished facial processing in individuals with ASD and the overrepresentation of male individuals in the clinical group. Additionally, neuropathological research confirmed disruptions in certain brain areas, especially the prefrontal cortex, the thalamus, the amygdala, the superior temporal sulcus, and the fusiform gyrus (Baron-Cohen et al., 1999; Hall, Doyle, Goldberg, West, & Szatmari, 2010). Particularly the two latter areas are recognized to be involved in facial processing. An alteration in signal or neurobiology in individuals with ASD gives strong reason for a connection between brain alterations and cognitive and behavioral differences (Suda et al., 11 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS 2011). Moreover, a connection to social anxiety seems to exist. Garner, Mogg, and Bradley (2006) found that individuals suffering from social anxiety avoid looking at faces and social stimuli in general. They suggest a problem in facial processing of these individuals. This can be associated with distorted facial processing in individuals suffering from ASD (Golarai et al., 2006). An additional explanation might be that faces as social stimuli elicit fear in patients with ASD, as much as the presence of an overall deficit in basic emotional processing, leading to avoidance of social interactions, and hence avoidance of interaction with faces (Wilbarger, McIntosh & Winkielman, 2009). Already Kanner proposed anxiety as a considerable factor in his original description of infantile autism (White, Oswald, Ollendick, & Scahill, 2009). Previous studies have focused on the activation of different brain structures in individuals with ASD. In particular, the amygdala appears to show abnormal activation in response to certain stimuli. The mid-brain structure is involved in rapid and automatic fear processing and usually becomes activated when possible danger is processed, inducing a rapid response - such as the fight-or-flight response (Golarai et al., 2006; Öhman, 2009). Moreover, this structure is involved in the recognition of fear and shows neuronal abnormalities in individuals with ASD (Baron-Cohen et al., 1999; Hall et al., 2010). Dalton et al. (2005) discovered that individuals with ASD, who are fixating faces, show hyperactivation of the left amygdala, hence putting forward a fear reaction. To avoid overarousal of fear-relevant brain structures, avoidance of faces - which induce fear in these individuals - could lead to a hypoactivation of the amygdala in general, as seen in the study by Dalton. 1.2 Startle Eyeblink Response In addition to fMRI studies investigating the activation of the amygdala, physiological studies are often used to examine the nature of fear reactions (Globisch, Hamm, Esteves, & Öhman, 1999; Öhman, 2009; van den Hout, de Jong, & Kindt, 2000). Higher skin conductance responses were observed in individuals with phobias while watching images representing the feared object (Öhman, 2009; van den Hout et al., 2000). Similarly, startle reflex modulation has gained much evidence in the last years regarding fear reactions. Advantages of this measure are amongst other things the good temporal resolution (Åsli, Kulvedrøsten, Solbakken, & Flaten, 2009), similar reactions across age and gender groups, and the independence of language and voluntary actions (Wilbarger et al., 2009). Hamm, Cuthbert, Globisch, and Vaitl (1997) reported a higher eyeblink magnitude, hence an increased startle eyeblink response, in individuals with ophio- and arachnophobia watching 12 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS pictures of snakes or spiders, respectively. Furthermore, the participants showed avoidance behavior, represented in less time viewing the given picture. This parallels the behavior of individuals with ASD, who avoid looking at social stimuli, such as faces, because these are inducing fear, just like pictures of spiders induce fear in someone suffering from arachnophobia. Usually, avoidance behavior is expressed with heightened startle eyeblink responses in healthy individuals toward unpleasant stimuli. The startle eyeblink response is enhanced by negative events and reduced by positive stimuli in comparison to control objects (Dichter et al., 2010). A loud noise for example is interpreted as a threatening situation and a startle eyeblink response occurs. Positive events associated with the startle probe (noise) usually reduce this automatic reflex. The startle eyeblink response is generally intact in individuals with ASD, hence giving the possibility to test affective reactions in a group of patients (Wilbarger et al., 2009). Negative events coupled with an aversive noise should elicit higher startle responses, while positive events paired with noise should reduce the startle effect in both healthy and autistic individuals. As in the study of Wilbarger et al. (2009), Dichter, Benning, Holtzclaw, and Bodfish, (2010) investigated the startle eyeblink response of individuals with ASD to pictures of different valence in comparison to neurotypical participants. The EMG results suggested an enhanced startle eyeblink response to positive stimuli for the ASD group. The diminished response to unpleasant stimuli did not reach significance. Moreover, the study demonstrated an enhanced postauricular reflex to unpleasant pictures, stating an exaggerated avoidance response, measured behind the ear (pulling back of the ear). Dichter et al. (2010) concluded that deficits in emotional informational processing are present in individuals with ASD, consistent with the findings of Wilbarger et al. (2009). Nevertheless, studies concerning the startle eyeblink response in reaction to facial stimuli are generally fairly contradictive (Alpers, Adolph, & Pauli, 2011). While enhancement of the startle eyeblink response to negative scenes has become obvious in many studies, there is still a lot of uncertainty about the influence of the emotion expressed in facial pictures. Alpers et al. (2011) explain this discrepancy by higher emotional arousal of scenes, while facial expressions do not create this high level of arousal in the viewer, leading to diverse results. The present study is focusing on the startle eyeblink response, triggered by an acoustic probe of white noise. Startle responses are commonly tested in affective or attention measures (Flaten, Nordmark, & Elden, 2005). The latency of an acoustic startle is relatively short with about 6-8 msec. Operating as a startle center, especially the nucleus reticularis pontis caudalis 13 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS (nRPC) located in the pons, is thought to be the main structure involved in the response. This is supported by the finding that a startle response can be elicited by electrical stimulation at this site (Lee, López, Melone, & Davis, 1996). The nRPC is connected to the muscles around the eye controlling the eyeblink reflex. Furthermore, input from the amygdala is received here (Dichter et al., 2010). Since there is a connection between the amygdala and startle response amplitude, an abnormal startle eyeblink response in individuals with ASD could moreover indicate a dysfunction of the amygdala as pointed out previously (Wilbarger et al., 2009). 1.3 Hypotheses Given that individuals suffering from ASD show abnormal gaze patterns when processing faces (Dalton et al., 2005), and that previous studies showed abnormalities in the neurology of autistic individuals (Golarai et al., 2006), autistic individuals are expected to express more anxiety when processing faces. Consequently, an enhanced startle eyeblink response to facial objects can be expected. The assumption that an autistic phenotype exists and extends far into the non-clinical population, leads to the presumption that the group scoring high on the autism spectrum quotient questionnaire will show an increased startle eyeblink response magnitude in response to social stimuli, in this case faces. As a result, the first hypothesis is as follows: Hypothesis 1: The high scoring group on the AQ is more likely to show increased startle reflexes when viewing social stimuli/faces, due to elicited fear. Wilbarger et al. (2009) demonstrated that fear reactions in autistic individuals are unconscious and found out that individuals with ASD do not differ from healthy individuals in a subjective measure of fear. With a visual analogue scale (VAS), where subjective feelings regarding valence and arousal levels can be indicated, emotion recognition can be measured. Autistic participants in the study by Wilbarger et al. (2009) recognized the right emotions, consistent with those of healthy individuals, yet showed enhanced fear reactions indicated objectively by the startle eyeblink response to stimuli not indicated as fear inducing in the subjective measurement. Based on that study, valence and arousal ratings are expected to show no difference between the groups, pointing to an unconscious mechanism of fear. Hypothesis 2: No difference is expected between the experimental and the control group in the subjective ratings of valence and arousal. 14 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS The principle of the startle eyeblink response is based on the fact that fear reactions elicit higher eyeblink responses - as a form of the fight-or-flight reflex. Fear is expressed automatically. Accordingly, negative events or pictures elicit a higher startle eyeblink response, while positive events or pictures diminish the response (Dichter et al., 2010). Taking this as a starting point, a difference in startle magnitude to the different emotions shown in the stimuli pictures is expected in the present study. Hypothesis 3: A difference in startle magnitude between the different emotions is expected. 1.4 Relevance The present study aims at investigating the cognitive and affective nature of face processing in students with autistic traits by measuring the startle eyeblink response. Some studies have been conducted in this field of research, investigating emotional processing in children and adolescents with ASD (Dichter et al., 2010; Wilbarger et al., 2009); however, the field of research is new and further support of existing theories is of great importance. Since the spectrum of the disorder can range widely and symptom expression is of high heterogeneity, it is important to extend investigations of the effect into the non-clinical population. The autistic phenotype is of vast diversity and autistic traits can be seen in, for example, a student population. Considering that even students can express distorted social behavior or experience similar developmental problems typical for individuals with ASD, it is of high relevance to identify the problems and restrictions in daily life. If it can be established that a certain amount of students are showing enhanced incidences of autistic traits, further investigations in this field will have to be made. With this, an understanding of the wide spectrum of ASD can be better understood and social support can be established for individuals affected. Consequently, this will help doctors, psychologists, parents and caregivers to improve in the field of dealing with the disorder. Specialized therapies can be developed to make life easier for patients and their families. 15 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS 2 Method 2.1 Participants To recruit participants, flyers were hung up at different faculties of the University of Tromsø, Norway, with focus on the natural science faculty. After early drop-out of one participant, 40 students between 19 and 31 years participated in the study (M = 22.96, SD = 2.698 for age). Twenty-two participants were male. The participants were divided into two age-controlled groups, the experimental group scoring 17 or higher on the AQ and the control group scoring below 17, resulting in 14 participants representing the experimental group high in autistic traits and 26 participants low in autistic traits. The latter served as the control group. Freitag et al. (2007), who evaluated a short edition of the German version of the AQ (AQ-k) as a screening instrument, came to the conclusion that a threshold of 17 is reasonable in screening neurotypical individuals for autistic traits. This cut-off score was adapted for the present study to achieve a realistic division into two groups. The mean AQ score was 15.1 (SD = 5.261) for the 40 participants. Table 2 Demographics of all Participants per Gender Gender Male Female N Minimum Maximum M SD Age 22 19 26 22.36 2.172 AQ 22 5 27 16.05 5.753 Age 18 20 31 23.67 3.144 AQ 18 5 20 13.94 4.478 Note. SD = Standard Deviation. 2.2 Materials 2.2.1 EMG/picture presentation. To record the strength of the startle eyeblink response, surface-electrodes were attached to the muscle under the right eye, a muscle called ‘orbicularis oculi’. These electrodes recorded the electromyographic (EMG) activity in comparison to a control 16 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS electrode adjusted to the forehead (Hamm et al., 1997). White noise of 95dB was presented over headphones during picture presentation. Acoustic probes were semi-randomized and occurred at one out of three given points in time after picture onset (2.5, 3.5 or 4.5 seconds after onset). No same latency occurred more than twice after each other. With this, different latencies of responses could be accounted for. Five acoustic probes were presented before first picture onset, so that participants got habituated to the noise. The acoustic probe was presented with picture display, hence occurring while the participants were viewing the object on a screen. Some control noises were presented during a black screen, functioning as baseline stimuli. To ensure that participants paid attention to the presented images, a web-cam had been installed next to the screen, so that the whole session could be followed from the experimenter’s room. Twenty-seven different pictures were presented randomly on a computer screen in front of the participant. All of these pictures were appearing twice in each session, so that a total number of 54 images were shown. Picture presentation of one set of all pictures took about 20 minutes. The pictures represented facial images (photographs) showing six happy, six fearful, six angry and six neutral emotional faces, each seen out of two different angles. One direction was a frontal view of the faces; the other a 45° sideways turned photograph showing the face from the left-hand side. Three neutral control images, representing objects, appeared randomly as control variables. Pictures were taken from the Karolinska Directed Emotional Faces set (KDEF; Lundqvist, Flykt, & Öhman, 1998), originally consisting of 4900 standardized emotional facial pictures, showing different emotional reactions. Four out of seven original emotions were selected (happy, fearful, angry, and neutral), presented out of two angles (original dataset consisting out of five angles). Cultural validity was met due to the objectiveness of the measurement. Therefore, no influence on the measurement was expected due to the different nationalities of the participants. 2.2.2 SAM/VAS subjective measure. To test the difference between objective and subjective feelings of fear, the Self Assessment Manikin (SAM; Bradley & Lang, 1994) in combination with a visual analogue scale (VAS) was given after the experimental session. Participants indicated on a continual line (VAS) how much arousing/calming and positive/negative they experienced each of the 27 pictures seen before in the EMG session. Pictures were presented again and participants could individually decide for how long they wanted to see each of the pictures. After that, the VAS appeared and indication could take place via mouse click. Images (SAM) helped to identify 17 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS the right emotions. Those images might especially be of importance when verbal IQ is in a lower range, so that identification of the right answer is easier than when answers have to be read. The subjective measure was done because fear reactions can often be unconscious (Wilbarger et al., 2009). If so, the subjective measurement of fear should not show any differences in fear ratings between the two groups. 2.2.3 Autism spectrum quotient questionnaire. The last test to be conducted in the testing session was the autism spectrum quotient questionnaire (AQ), a self-administered forced-choice 4-point scale questionnaire, containing of 50 items. Skills like attention switching, imagination ability, social skills, communication skills, and attention to detail are assessed by the AQ. Only the latter category is known to be improved in individuals with ASD, while the other four categories are generally underdeveloped in patients (Baron-Cohen et al., 2001). The AQ has been found to be an efficient tool for assessing the autistic phenotype in a non-clinical population (Wheelwright, Auyeung, Allison, Baron-Cohen, 2010). Participants indicated on a scale if they strongly agreed, slightly agreed, slightly disagreed or strongly disagreed with the given statement. Presence of the autistic trait was scored with 1, absence with 0, such that total scores could range from 0 to 50. For Norwegian students the Norwegian version of the AQ was used, for international students the original English version was given to avoid misunderstandings due to language (Baron-Cohen et al., 2001). 2.3 Procedure After signing the informed consent, participants sat down on a comfortable chair in the testing room in front of a computer screen. The experimenter again instructed participants about the procedure, the duration, and nature of the experiment. The importance of following the pictures at all times was especially emphasized. Three electrodes were prepared with twosided tape and gel. The skin below the orbicularis oculi muscle under the right eye and on the forehead was cleansed and the electrodes attached. As soon as the participants’ eyes got habituated to the electrodes, headphones were placed over the ears, the web-cam placed in the right position, and instruction to look at the screen while picture presentation was given once more. The computer screen was switched on and the experimenter left the room. In the experimenter’s room the test program was started after validating and controlling the sound settings. The pictures appearing on the test screen could also be followed on the 18 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS experimenter’s screen as well as the video from the web camera, so that errors in presentation could directly be detected and adjusted. After completing the EMG session, participants were taken to the experimenter’s room, seated in front of another computer screen, where the subjective measure (VAS/SAM) was carried out. Instructions were given on screen and by the experimenter. Following the subjective test, participants answered to the 50 statements of the AQ by indicating one point on a 4-point response scale (strongly agree, slightly agree, slightly disagree, or strongly disagree). Participant’s help was compensated with two lottery scratch tickets, worth 50 Norwegian Crowns (~ 8 US $). 2.4 Apparatus and EMG EMG activity was recorded with three sintered-pellet silver chloride AgCl miniature surface electrodes of 4 mm diameters, filled with Microlyte electrolyte gel (Coulbourn Instruments). Two electrodes were attached to the skin at the right orbicularis oculi with an interdistance of around 1.5 cm, while the control electrode was placed in the middle of the forehead. The EMG signal was amplified by a factor of 50000 and filtered (8-1000 Hz) by a Coulbourn V75-04 bioamplifier. The signal was further integrated with a Coulbourn V76-24 contour-following integrator with 10 ms constant. On a LabLinc V interface on a connected computer the output was recorded (100 ms before until 200 ms after stimulus presentation). Noise stimuli lasted 50 ms and were presented at 95 dB over Sennheiser HD 250 headphones. Different latencies of noise presentation were accounted for in semi-randomized order. 2.5 Data Analysis Since the differences in reactions of the group scoring high on autistic traits in contrast to the group scoring low on the AQ, plus the individual differences within the groups, were investigated, the data was analyzed with repeated-measures analysis of variance (ANOVA). This statistical method accounts for the between-subject variable measuring the differences between the two groups tested (high versus low scoring group) and the within-subject variable which measures the differences in startle eyeblink response between individuals within one given group. Therefore, the between-subject design explained whether there was a significant effect in startle eyeblink response between the different groups, for example if the high scoring group truly showed enhanced startle responses to faces (hypothesis 1). The withinsubject component explained the differences within each group. A repeated-measures ANOVA combines these factors in one analysis. The analysis was done for the EMG session 19 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS and the subjective measure individually. The advantage of a within-subject design is the reduction of variability and an increased power to detect significant effect. To measure the dependent variable startle magnitude, the different emotions compared with the baseline object were used as a 4-level within-subject factor. A 2-level within-subject factor for direction was added. As a between-subject factor the low and high scoring groups on the AQ were used. 3 Results 3.1 Autism Spectrum Quotient Questionnaire The scores of the AQ showed large variations between the 40 participants (M = 15.10, SD = 5.261), supporting the view of an autistic phenotype reaching into the normal population. The participants’ scores ranged from 5 (very low autistic traits) to a score of 27, reaching as high as the cut-off score for autism spectrum disorder mentioned in another study (Woodbury-Smith, Robinson, Wheelwright, & Baron-Cohen, 2005). Twelve participants had to be excluded from further analysis because they were drinking coffee during the three hours prior to the experimental session. The startle eyeblink response is known to be influenced by caffeine, which has lead to exclusion of these participants in the present study (Mikalsen, Bertelsen, & Flaten, 2001). After exclusion of the given participants from further analysis, 12 high scoring and 16 low scoring individuals were included. Seventeen of the 28 participants were male. The mean score of the AQ after exclusion was 16.04 (SD = 5.31) with a mean age of 22.57 (SD = 2.69) for the 28 participants. 3.2 Ratings The subjective SAM/VAS measure showed a significant difference in valence ratings of the different emotions (F (8,240) = 62.844, p < .001). Happy faces from either side were rated more positively than neutral, fearful and angry faces. Objects were rated having neither positive nor negative value. For the valence rating no difference between the groups was found (F (8,232) = .205, p = .99). All emotions elicited the same ratings of positivity/negativity, independent of the AQ score. As for the valence ratings, arousal levels of the SAM/VAS also reached significance (F (8,240) = 31.775, p < .001). Higher arousal levels were elicited by angry and fearful faces from either direction, in comparison to rather low activation by neutral, happy and object 20 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS stimuli. Equally to the subjective valence scores, ratings of arousal did not differ between the high and low scoring group (F (8,232) = 1.17, p = .32). 3.3 Startle Eyeblink Response Contrary to the prediction of higher startle eyeblink response to facial stimuli for the group high in autistic traits, no significant difference was found in comparison to the control group. The repeated-measures ANOVA did not reach significance for the between-subject effect of high against low AQ groups, F (1, 26) = .035, p = .853. Overall, the high scoring group showed rather a diminished startle eyeblink response to all stimuli. Startle eyeblink response to objects was used as a baseline. Table 3 summarizes F-scores and p-values of the repeated-measures ANOVA. Table 3 Within-Subject Analysis for Emotions, Direction, and All Interaction Effects with the Between-Subject Variable AQhigh Effect Mean Square F Sig. emotions 0.254 2.451 0.106 Emotions · AQhigh 0.034 0.581 0.535 direction 0.524 12.873 0.001* Direction · AQhigh 0.002 0.046 0.832 Emotions · direction 0.188 2.078 0.134 emotions·direction·AQhigh 0.035 0.392 0.683 Note.*significant at .005 level. Nevertheless, a clear significant difference between the different angles of presentation was found (F (1, 26) = 12.873, p = .001). Frontal presentation of the pictures led to higher overall startle eyeblink responses in both groups. Presentation from the side resulted in lower magnitude and reduced difference between the dissimilar emotions, especially for the high scoring group (see figure 2). Furthermore, there was a difference in startle activation between the four emotions (F (7,203) = 2.339, p = .0257), confirming hypothesis 3. A post- 21 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS hoc Tukey test revealed significant differences between angry frontal and fearful frontal, and neutral sideways and fearful frontal picture presentations. Figure 2: Startle eyeblink responses for all four emotions for both groups with frontal (left) and angular (right) picture presentation 4 Discussion In the present study the startle eyeblink response to social stimuli in students with high autistic traits was assessed. No confirmatory evidence could be found for hypothesis 1, stating that higher startle eyeblink response to facial stimuli would be observed for the group scoring high on autistic traits. There was no difference in startle magnitude between the two groups. Hypothesis 2, maintaining that no difference between the groups for the objective measures should be expected, could be confirmed. The ratings of valence and arousal were the same regardless of AQ score. The third hypothesis, holding that there is a difference in startle eyeblink response between the different emotions presented, could be confirmed. Pictures representing fear from a frontal perspective elicited higher startle than frontal angry or neutral sideways facial expressions. Moreover, a difference between the different angles of picture presentation was found. Pictures seen from the front resulted in higher startle eyeblink responses than pictures seen from a 45° angle from the side. Subsequently, the results will be discussed. 22 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS 4.1 Hypotheses revisited Students high in autistic traits did not show an enhanced response to social stimuli in comparison to the control group. Consequently, hypothesis 1 could not be confirmed. Nevertheless, the finding is consistent with the overall picture of the current research in this new field. Hypotheses and results regarding startle eyeblink response in individuals with ASD are contradicting and different theories exist (Alpers et al., 2011). Bernier, Dawson, Panagiotides, and Webb (2005) examined the two hypotheses of enhanced versus diminished fear reactions due to under- versus over-responsiveness of the amygdala. As in the present study, they came to the conclusion that there was no difference between the experimental and control group. The same conclusion was drawn by Salmond, de Haan, Friston, Gadian, and Vargha-Khadem (2003) who did not find any difference in startle eyeblink response to nice and scary pictures between autistic children and to the neurotypical group. There are several reasons for the fact that no difference was found between the two groups. First of all, the before mentioned range of diverse results suggests that in this young field of research no clear picture of results exists yet. As for the different emotions, results vary for the startle eyeblink response between ASD and control groups. In addition, Alpers et al. (2011) explain the difference not by the valence, but arousal of the different pictures. They claim that higher arousing pictures lead to higher startle responses, regardless of the valence of the picture. Their study results show higher startle responses to both positive and negative pictures with highly arousing level, in comparison to low arousing pictures of either valence. A lower startle response of individuals with ASD was explained by a greater alertness of healthy individuals. Regarding this conclusion, the current study shows similar results, with no difference between the experimental and control group, but a tendency to overall lower startle responses in the high scoring AQ group. As predicted and confirmed by Wilbarger et al. (2009), patients do not differ from a neurotypical group in subjective measures of valence and arousal. The difference in startle eyeblink response found in that study was explained by an unconscious process for objective measurements. The present study found that recognition of emotional and facial stimuli is normal in individuals scoring high on the AQ, indicated by no difference in valence and arousal ratings between the two groups. Wilbarger et al. (2009) drew the same conclusion for their sample of patients with ASD. The two different groups used in the two studies might not be comparable without any deduction. However, the present results point toward the direction of an autistic phenotype reaching into the normal population with comparable results to those found in individuals suffering from ASD. Moreover, the results of the subjective 23 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS measurement confirm that identification of the different emotions is intact and equivalent in the two groups. The fact that hypothesis 1 could not be confirmed is therefore not due to a defect in emotional processing, but possible cognitive processing distortions as predicted by Wilbarger et al. (2009). The presence of aberrant cognitive processes has to be investigated in future studies. The finding that the different emotions differed significantly from each other is consistent with the study by Anokhin and Golosheykin (2010) who investigated the reaction to fearful faces, which elicited higher startle response than neutral or happy faces. However, they did also find higher startle to angry faces, which could not be confirmed by the present study. In contrast to another study which found higher startle eyeblink response to angry than to fearful faces (Springer, Rosas, McGetrick, & Bowers, 2007), the opposite was found in the current study. A lot of mixed results exist in this field of research and further investigation will be of importance. Especially, the direction of picture presentation has gained little attention in previous studies. As it has been found in the present study, direction of picture presentation influences the startle eyeblink response. Future studies should thus account for different angles of direction in picture presentation. Nevertheless, the current results are corresponding with the theory that negative images elicit higher startle responses in comparison to positive or neutral stimuli regardless of AQ score (Dichter et al., 2010). The effect that different angles of presentation lead to a significant difference in startle eyeblink response has not been investigated by any study before. Frontal presentation elicited greater startle eyeblink response in the present study than images presented in a 45° angle from the left side. An explanation for this finding might be that frontal presentation leads to a rather direct confrontation with the face presented. Therefore, participants feel more addressed by the person in the picture and reactions are more intense. Such as, if an angry face is facing the participant directly, fear reactions increase in comparison to a face just seen from the side and hence not addressing the participant her- or himself directly. That is comparable to the results of the study by Sabatinelli, Bradley, and Lang (2001), who found that startle responses increased when participants were anticipating instead of just watching pictures. Anticipating - or awaiting - a stimulus can be compared to a more direct connection to the picture, as it is expected. This might lead to a stronger link between the participant and the upcoming picture. The same occurs with the different angles of presentation, with facial images confronting the participant more directly, leading to an increased emotional reaction in the participant. The anticipating effect was especially present for positive pictures. 24 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS 4.2 Limitations Different studies have confirmed that autistic individuals generally avoid looking at faces show a hypoactivation of the amygdala and related brain structures (Dalton et al., 2005), and show different patterns of fear reactions regarding social stimuli (Dichter et al., 2010; Wilbarger et al., 2009). Regarding altered neurobiological structures and mechanisms, Dichter et al. (2010) found, that especially the amygdala is involved in the deficits experienced by individuals with ASD. As the amygdala is involved in fear reactions, an altered neurobiology of this brain structure can account for distorted fear reactions. Furthermore, removal of the temporal lobe and amygdala in primates showed symptoms paralleling social deficits found in autism (Wilbarger et al., 2009). These brain structures can also directly influence the startle response. An enhanced startle eyeblink response in individuals with ASD has been found to positive images in the study by Dichter et al. (2010). On the other hand, Wilbarger et al. (2009) did not only find an increased startle eyeblink response, thus higher expression of fear, to positive but to negative stimuli as well. The authors interpreted these results as an indicator of increased defensive system activity in individuals with ASD. The results of the present study are not consistent with these findings; however, the studies described used children with a diagnosis of ASD, while in the current study healthy individuals were examined. Moreover, limitations of the given studies are that different age groups were used, including control and experimental group representing different ages. Additionally, not the same set of pictures as emotional stimuli were used in the studies, which can contribute to dissimilar reactions, especially regarding negative images (Wilbarger et al., 2009). In particular, the selection of facial stimuli pictures plays a major role in distinguishing fear reactions of patients and normal controls. Additionally, the differences in viewing time can contribute to further disparities in the results (Wilbarger et al., 2009). Another limitation results from the fact that individuals with ASD have a general impairment in mimicry, mutual gaze, and patterns of face viewing, which could result in unusual perception of the given stimuli (Golarai et al., 2006). Therefore, patients might not even recognize the valence of pictures due to uncommon gaze patterns. The limitations present in other studies can be further extended to the present study, consistent with the fact that varying results are found across different studies. The startle eyeblink response varies in different experimental settings, and higher startle has been found to positive, negative or both images. This stresses the importance of further investigation in this field of research, to come to reliable results regarding the nature of fear reactions to facial stimuli in ASD and the autistic phenotype. 25 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS Moreover, the present study has some further limitations. First of all, the sample size was not very large and after data reduction only 28 participants could be included in final analyses. Future studies should increase sample size to reach a better basis for generalizations. Unfortunately, the participant with the highest score on the AQ had to be excluded from all analyses due to early drop-out. More participants representing the high scoring group could possibly have changed the results. Furthermore, a generalization to individuals diagnosed with ASD can cause problems. The research field of an autistic phenotype is still in its fledgling stage and no clear results exist whether and how a connection between ASD and the normal population high in autistic traits is present. However, some studies have investigated important features and connections in this young field of research, and with further investigations a better understanding of the nature of ASD and its spectrum into the normal population can be achieved. In addition, results might have been biased by gender effects. Differences in gender were not accounted for and the general higher amount of male participants in the high scoring group could have lead to lower startle magnitude. Anokhin and Golosheykin (2010) found a gender difference in their study, with females expressing a general higher startle eyeblink response than males. In combination with the extreme male brain theory it is reasonable that more males are scoring high on the AQ. The results however showed no difference in startle magnitude in comparison to the control group. The control group had an overall higher, though not significant, magnitude of EMG signals, which could thus be explained by the overrepresentation of females in this group. However, this hypothesis should be further investigated to draw any reliable conclusions. To sum it up, most studies show varying results regarding the startle eyeblink response in individuals with ASD. Findings span from increase to negative, positive or both picture valences to no difference between the experimental and control group, as found in the present study. It has to be further investigated how startle eyeblink responses are affected by the valence of pictures for individuals suffering from ASD or those high in autistic traits. While diagnosis of ASD can be made fairly easily today, the nature and treatment of this severe disorder has to be further explored. Especially, the spectrum which seems to reach into the neurotypical population needs further investigation and will be of importance for a better understanding of this heterogeneous disorder. Autism spectrum disorder is still a young research field, and a lot of studies will be required to fully understand its nature and find better treatment techniques. If we can understand the social deficits these individuals are 26 COGNITIVE AND EMOTIONAL PROCESSING OF SOCIAL STIMULI IN STUDENTS WITH AUTISTIC TRAITS experiencing – especially regarding facial processing and fear reactions – caregivers, psychologists and patients can benefit from that. 5 Conclusion The general symptoms of ASD such as disturbances in non-verbal communication skills, social interactions and the expression of stereotyped behaviors can be found in virtually every patient (American Psychiatric Association, 2000). However, the expression of the syndrome varies vastly between individuals, and the disorder is highly heterogeneous. In this way, the spectrum can reach far into the neurotypical population and autistic symptoms can be observed in individuals not diagnosed with any form of ASD. All symptoms vary on a spectrum and can have expressions from a severe to a mild degree. The avoidance of eye contact and faces can be linked to diminished social interactions in general. The hypothesis of higher startle eyeblink responses in individuals scoring high on the AQ could not be confirmed. There were no differences between the two groups. The second hypothesis that there is no difference between the groups for the subjective measurement could be confirmed. Valence and arousal of the different emotions was experienced in the same way for groups scoring high and low on the AQ. The third hypothesis, that different emotions elicit varying magnitudes of startle eyeblink responses, has been confirmed - with fearful faces presented frontally leading to an increased startle eyeblink response in comparison to angry frontal and neutral pictures presented from the side. In addition, a significant difference was found between the different angles of picture presentation. Frontal presentation elicited higher startle eyeblink responses in comparison to presentation from a 45° angle. Overall, the existence of an autistic phenotype reaching into the non-clinical population could be shown. Fear reactions to facial stimuli appear to be comparable to those expressed by the neurotypical population. However, findings are contradictive in this young field of study and future studies will show how fear reactions to social stimuli are affecting individuals suffering from ASD. It will be of importance to account for the wide spectrum of the disorder as put forward by the present study. 27 References Alpers, G. W., Adolph, D., & Pauli, P. (2011). Emotional scenes and facial expressions elicit different psychophysiological responses. International Journal of Psychophysiology, 80, 173-181. American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders. (4th ed., text rev.). Washington, DC: Author. Anokhin, A. P., & Golosheykin, S. (2010). Startle modulation by affective faces. Biological Psychology, 83 (1), 37-40. Barlow, D. H., & Durand, V. M. (2002). Abnormal Psychology (3rd ed.). Belmont: Wadsworth Publishing. Baron-Cohen, S. (2002). The extreme male brain theory of autism. Trends in Cognitive Sciences, 6(6), 248-254. Baron-Cohen, S. (2005). The essential difference: The male and female brain. Phi Kappa Phi Forum, 85(1), 23-26. Baron-Cohen, S., Ring, H. A., Wheelwright, S., Bullmore, E. T., Brammer, M. J., Simmons, A., & Williams, S. C. R. (1999). Social intelligence in the normal and autistic brain: An fMRI study. European Journal of Neuroscience, 11, 1891-1898. Baron-Cohen, S., Wheelwright, S., Skinner, R., Martin, J., & Clubley, E. (2001). The AutismSpectrum Quotient (AQ): Evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. Journal of Autism and Developmental Disorders, 31, 5-17. Bernier, R., Dawson, G., Panagiotides, H., & Webb, S. (2005). Individuals with autism spectrum disorder show normal responses to a fear potential startle paradigm. Journal of Autism and Developmental Disorders, 35 (5), 575-583. Bradley, M., & Lang, P. (1994). Measuring emotion: The self-assessment manikin and the semantic differential. Journal of Behavioral Therapy and Experimental Psychiatry, 25 (1), 49-59. Charman, T., Jones, C. R. G., Pickles, A., Simonoff, E., Baird, G., Happé, F. (2011). Defining the cognitive phenotype of autism. Brain Research, 1380, 10-12. Dalton, K. M., Nacewicz, B.M., Johnstone, T., Schaefer, H. S., Gernsbacher, M. A., Goldsmith, H. H., Alexander, A. L., & Davidson, R. J. (2005). Gaze fixation and the neural circuitry of face processing in autism. Nature Neuroscience, 8, 519-526. Dichter, G. S., Benning, S. D., Holtzclaw, T. N., & Bodfish, J. W. (2010). Affective modulation of the startle eyeblink and postauricular reflexes in Autism Spectrum Disorder. Journal of Autism and Developmental Disorders, 40 (7), 858-869. Flaten, M. A., Nordmark, E., & Elden, Ǻ. (2005). Effects of background noise on the human startle reflex and prepulse inhibition. Psychophysiology, 42, 298-305. Flo and Kay: Twin savants. Retrieved April, 11, 2011, from http://splicetv.com/work/clients/flo_and_kay_twin_savants.html Freitag, C. M., Retz-Junginger, P., Retz, W., Seitz, C., Palmason, H., Meyer, J., Rösler, M., & von Gontard, A. (2007). Evaluation der deutschen Version des Autismus-SpektrumQuotienten (AQ) - die Kurzversion AQ-k. Zeitschrift für Klinische Psychologie und Psychotherapie: Forschung und Praxis, 36(4), 280-289. Garner, M., Mogg., K., & Bradley, B. P. (2006). Orienting and maintenance of gaze to facial expressions in social anxiety. Journal of Abnormal Psychology, 115 (4), 760-770. Globisch, J., Hamm, A. O., Esteves, F., & Öhman, A. (1999). Fear appears fast: Temporal course of startle reflex potentiation in animal fearful subjects. Psychophysiology, 36 (1), 66-75. Golarai, G., Grill-Spector, K., & Reiss, A. L. (2006). Autism and the development of face processing. Clinical Neuroscience Research, 6 (3), 145-160. Hall, G. B. C., Doyle, K. A. R., Goldberg, J., West, D., & Szatmari, P. (2010). Amygdala engagement in response to subthreshold presentations of anxious face stimuli in adults with autism spectrum disorders: Preliminary insights. PLoS ONE 5 (5): e10804. doi:10.1371/journal.pone.0010804 Hamm, A. O., Cuthbert, B. N., Globisch, J., & Vaitl, D. (1997). Fear and startle reflex: Blink modulation and autonomic response patterns in animal and mutilation fearful subjects. Psychophysiology, 34, 97-107. Klin, A., & Volkmar, F. R. (1999). Autism and other pervasive developmental disorders. In S. Goldstein & C. R. Reynolds (Eds.), Handbook of Neurodevelopmental and Genetic Disorders in Children (pp. 247-270). New York: Guildford Press. Lee, Y., López, D. E., Melone, E. G., & Davis, M. (1996). A primary acoustic startle pathway: Obligatory role of cochlear root neurons and the nucleus reticularis pontis caudalis. Journal of Neuroscience, 16, 3775-3789. Lundqvist, D., Flykt, A., & Öhman, A. (1998). The Karolinska Directed Emotional Faces KDEF, CD ROM from Department of Clinical Neuroscience, Psychology section, Karolinska Institutet, ISBN 91-630-7164-9. Mann, D. (2009, February). Flo and Kay: Twin autistic savants. Retrieved April, 11, 2011, from http://www.examiner.com/article/flo-and-kay-twin-autistic-savants McIntosh, D. N., Reichmann-Decker, A., Winkielman, P., & Wilbarger, J. L. (2006). When the social mirror breaks: Deficits in automatic, but not voluntary, mimicry of emotional facial expressions in autism. Developmental Science, 9, 295-302. Mikalsen, A., Bertelsen, B., & Flaten, M. A. (2001). Effects of caffeine, caffeine-associated stimuli, and caffeine-related information on physiological and psychological arousal. Psychopharmacology, 157 (4), 373-380. Öhman, A. (2009). Of snakes and faces: An evolutionary perspective on the psychology of fear. Scandinavian Journal of Psychology, 50, 543-552. Ridley, N. J., Homewood, J., & Walters, J. (2011). Cerebellar dysfunction, cognitive flexibility and autistic traits in a non-clinical sample. Autism, 15(6), 728-745. Rutter, M. (2006). Autism: Its recognition, early diagnosis, and service implications. Journal of Developmental and Behavioral Pediatrics, 27 (2), 54-58. Sabatinelli, D., Bradley, M. M., & Lang, P. L. (2001). Affective startle modulation in anticipation and perception. Psychophysiology, 38, 719-722. Salmond, C. H., de Haan, M. M., Friston, K. J., Gadian, D. G., & Vargha-Khadem, F. F. (2003). Investigating individual differences in brain abnormalities in autism. In U. Frith, & E. Hill (Eds.). Autism: Mind and brain (pp. 247-265). New York: Oxford University Press. South, M., Ozonoff, S., & McMahon, W. M. (2005). Repetitive behavior profiles in Asperger syndrome and high-functioning autism. Journal of Autism and Developmental Disorders, 35 (2), 145-158. South, M., Larson, M. L., Krauskopf, E., & Clawson, A. (2010). Error-processing in high-functioning Autism Spectrum Disorders. Biological Psychology, 85 (2), 242-251. Springer, U. S., Rosas, A., McGetrick, J., & Bowers, D. (2007). Differences in startle reactivity during the perception of angry and fearful faces. Emotion, 7 (3), 516-525. Suda, M., Takei, Y., Aoyama, Y., Narita, K., Sakurai, N., Fukuda, M., Mikuni, M. (2011). Autistic traits and brain activation during face-to-face conversations in typically developed adults. PLos One, 6(5), e20021. doi:10.1371/journal.pone.0020021 van den Hout, M. A., de Jong, P., & Kindt, M. (2000). Masked fear words produce increased SCRs: An anomaly for Öhman’s theory of pre-attentive processing in anxiety. Psychophysiology, 37 (3), 283-288. Volkmar, F. R., State, M., & Klin, A. (2009). Autism and autism spectrum disorder: diagnostic issues for the coming decade. Journal of Child Psychology and Psychiatry, 50, 108-115. Wheelwright, S., Auyeung, B., Allison, C., & Baron-Cohen, S. (2010). Defining the broader, Medium and narrow autism phenotype among parents using the Autism Spectrum Quotient (AQ). Molecular Autism, 1 (10). doi: 10.1186/2040-2392-1-10 White, S.W., Oswald, D., Ollendick, T., & Scahill, L. (2009). Anxiety in children and adolescents with autism spectrum disorder. Clinical Psychological Review, 29 (3), 216-229. Wilbarger, J. L., McIntosh, D. N., & Winkielman, P. (2009). Startle modulation in autism: Positive affective stimuli enhance startle response. Neuropsychologia, 47 (5), 13231331. Woodbury-Smith, M. R., Robinson, J., Wheelwright, S., & Baron-Cohen, S. (2005). Screening adults for Asperger syndrome using the AQ: A preliminary study of its diagnostic validity in clinical practice. Journal of Autism and Developmental Disorders, 35 (3), 331-335. Åsli, O., Kulvedrøsten, S., Solbakken, L. E., & Flaten, M. A. (2009). Fear potentiated startle at short intervals following conditioned stimulus onset during delay but not trace conditioning. Psychophysiology, 46, 880-888.