Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
DO. Use of specimen turnaround time as a component of laboratory quality-a
comparison of clinician expectations
with laboratory performance. Am J Cliii Pathol 1989;92:613-8.
5. Henderson AR. The priority test request form: a method for
improving communication
between the physician and the emergency clinical biochemistry laboratory. J Cliii Pathol 1979;32:
97-9.
6. Henderson AR. The test request
communication
between the physician
form:
a neglected
route
for
and the clinical chemist? J
Cliii Pathol 1982;35:986-98.
7. Valenstein PN, Emancipator
K. Sensitivity,
specificity, and
reproducibility
of four measures of laboratory turnaround
time.
Am J Cliii Pathol 1989;91:452-7.
8. Gardner MJ, Gardner SB, Winter PD. Confidence interval
analysis microcomputer
program. London: British Medical Journal, 1989:77pp.
9. Hilborne LH, Oye RK, McArdle JE, Repinaki JA, Rodgerson
DO. Evaluation of stat and routine turnaround
times as a componentof laboratoryquality. Am J Clin Pathol 1989;91:331-5.
10. Howanitz PJ, Steindel SJ. Intralaboratory
performance and
laboratorians’ expectations forstat turnaround times. Arch Pathol
Lab Med 1991;115:977-83.
11. Barnett RN, MclverDD, Gorton WL. The medical usefulness
of stat tests. Am J Clin Pathol 1978;69:520-4.
12. Howanitz PJ, Steindel SJ, Cembrowski GS, Long TA. Emergency department stat test turnaround times. Arch Pathol Lab
Med 1992;116:122-8.
13. McConnell TS, Writtenberry-Loy
C. Whither waiting turnaround times of laboratory tests for emergency room patients. Lab
Med 1983;14:644-7.
14. Donabedian A. Explorations in quality assessment and monitoring. Vol. 1. The definition of quality and approaches to its
assessment. Ann Arbor: Health Administration
Press, 1980:163
pp.
15. Juran JM. Juran on quality by design. New York: The Free
Press, 1992:538 pp.
16. Selker HP, Beshsnsky JR, Pauker SG, Kassirer JP. The
epidemiology of delays in a teaching hospital. The development
and use of a tool that detects unnecessary hospital days. Med Care
1989;27:112-29.
17. Valenstein
PN. Turnaround time-can
we satisr clinicians’
demands for faster service? Should we try? [Editorial]. Am J Cliii
Pathol 1989;92:705-6.
CUN. CHEM. 39/6, 1059-1063 (1993)
Glutamine Stability in BiologicalTissues Evaluated by Fluorometric Analysis
V. Bruce Grossie, Jr.,”3 John Yick,’
Mark Alpeter,’
Thomas C. Welbourne,2 and David M. 0th’
quantity of plasma (25 L) or tissue (200 mg) and is a
Although glutamine has been considered unstable during
convenient method for quantifying this important amino
storage and therefore difficult to quantitate, recent results
suggest this amino acid is stable at low pH ranges. We
acid.
evaluated the stability of glutamine in plasma and tissue
extracts, using fluorometric analysis. The measured conIndexing Terms: amino acids
sample handling
centration of glutamine detected varied linearly up to 0.8
mmol/L for the aqueous solution (r2 = 98.7, P = 0.0001)
Glutainine is an important amino acid for the nutriwith a mean (±SD) coefficient of variation of 2.41% ±
tional regimens of catabolic and cancer patients (1-3).
0.79%. When glutamine was dissolved in 50 g/L trichloManipulation
of the amino acid composition of total
roacetic acid (TCA), the values were essentially unalparenteral nutrition formulas for catabolic and tumortered. Glutamine in an aqueous solution and stored at
bearing hosts has received considerable attention in the
-70#{176}C
was stable for at least 16 days; glutamine in TCA
past few years (1-11). Glutamine is the most abundant
was stable for 6-8 days, then decreased to a concentracirculating free amino acid and in intracellular pools is
tion significantly lower than that of the aqueous solution.
a precursor for amino acid, protein, and nucleotide
The expected and observed concentrations in plasma
synthesis and is required for ammonia genesis by the
were equal (r2 = 0.99975) for increasing amounts of
kidney (12).
added glutamine. Glutamine concentrations in plasma
Glutamine
has previously been considered to be unwere stable for >1 year when stored at -70 #{176}C.
The
stable in aqueous solutions when subjected to heat (12,
glutamine of a transplantable rat sarcoma and a normal
13). Gilbert et al. (14) presented results showing that
rat liver could be extracted with 50 g/L TCA with high
the concentration of anions such as phosphate adversely
efficiency (88.6% ± 1.9% and 90.2% ± 0.04%, respecaffected glutaunine stability.
Herskowitz
et al. (15),
tively); the extracted glutamine is stable in TCA for at least
however, reported that glutamine
concentration
is sta7 days without neutralization when stored at -70 #{176}C.ble at refrigerator
temperatures
(5#{176}C,
pH 6.2) for 2
Fluorometric analysis of glutamine required only a small
days; stored at -20#{176}C
(pH 6.2), the concentration of
glutamine was stable for 3-7 days. Shih (16) demonstrated that the stability of glutamine at 37#{176}C
for 24 h
1Department of General Surgery, Box 106, The University of
was 100% at pH 3 but decreased with increasing pH to
Texas M.D. Anderson Cancer Center, 1515 Holcombe, Houston,
TX 77030.
-35% at pH 10. Rosenblum (17) reported that gluta2Department of Physiology and Biophysics, LSU Medical Cenmine remained stable when prepared in citrate or aqueter, Shreveport,
LA.
ous solution and deproteinized plasma.
‘Author for correspondence.
No study has evaluated the stability of glutamine in
Received July 13, 1992; accepted January 18, 1993.
CUNICAL CHEMISTRY,
Vol.39, No. 6, 1993 1059
tissue extracts, however, even though many articles
concerning the importance of this amino acid have been
published. The purpose of this study was to evaluate the
stability of glut.amine in plasma and tissue extracts by
using a fluorometric
analysis
for glutamine
and gluta-
B represent the results for glutainine,
glutamate,
stan-
dard, and the blank, respectively.
(R2GLN-R1GLN)-(R2B-R1B)
f
Glutamine
=
mate.
1
(R2ST-R1STD)
1
Materials and Methods
x STD concentrationJ
Procedures
Assay. L-Glutamine
(Sigma Chemical Co., St. Louis,
MO) was assayed by a modification of the procedure of
Lund (18), which measures the change in the fluorescence of NADH (Sigma Chemical Co.). The procedure is
detailed in Table 1. The glutamine
in the plasma or
tissue extract was converted to glutamate by glutaminase (Grade V; Sigma Chemical Co.). The resulting
glutamate was then assayed by measuring the NADH
formed by the conversion of glutamate to a-ketoglutarate and ammonia by glutamate dehydrogenase (Boehringer Mannheim Corp., Indianapolis,
IN). The NADH
was measured with a Perkin-Elmer
LS-50 Luminescence Spectrometer (Perkin-Elmer
Corp., Stafford, TX)
at an excitationwavelength of 342 nm (5-nm slit width)
and an emissions wavelength of 459 nm (20-nm slit
width).
Calculations. The calculations for glutamine and glutainate in plasma (mo]/L) and tissues (mol/g wet tissue)
were similar to those by Lund (18), where Ri and R2
represent the fluorescence values from the different
stages of the assay (Table 1), and GLN, GLU, STD, and
Table 1. Procedure for Spectrofluorometric
Glutamate
-glutamate
1(R2GLU-R1GLU)-(R2B-R1B)
ST
=
L
(R2
D-R1STD)
x STD concentration
Standard curve. Initially, glutamine was dissolved in
sterile water or 50 g/L trichloroacetic acid (TCA) solution and assayed as shown in Table 1. Each concentration was assayed in triplicate, the coefficient of variation
(CV) for each concentration was calculated as described
by Zar (19), and the mean CV was then calculated from
the CVs from the seven concentrations. Preliminary
results demonstrated that 50 gIL TCA was the best acid
for tissue extraction. The effect of 50 g/L TCA on the
fluorometric assay and standard curve of glutamine was
therefore compared with results for an aqueous solution.
Stability:
aqueous vs 50 gIL TCA Standard concentrations of glutamine were prepared in sterile water (n
=
5) or 50 g/L TCA (n = 5). One aliquot of each solution
Analysis for Glutamine and Glutamate
In Plasma and Tissues
Added to essay
Reaction cemponsnt
2
3
4
5
6
Part II
1
2
3
4
5
6
7
8
9
Glutamlns
Acetate buffer (1.0 mmol/L, pH 4.9), L
Sample, L
Standard,L
Sterilewater, L
Glutaminase,#{176}
L
Incubate(37 ‘C), mm
Cold TCA (50 g/L), &L
Centrifuge, mm
Pyrophosphatebuffer (26 g/L, pH 8.6), L
Samplefrompartl,uL
NAD (20 g/L 30 mmol/L), L
Glutamate
25
55
25
25
Standard
25
Blank
25
25
30
25
30
60
60
180
180
30
60
180
10
10
10
10
2000
140
2000
2000
140
2000
140
40
40
8
8
8
45
45
45
40
Mbctwuce
Measure fluorescence three times and averagereading(Ri)
GLDH (20 U/mg),d&L
8
Mix twice
Incubateat room temperature (covered), mm
45
Measure fluorescence(meanof three readings:R2)
OC
140
40
60
180
a The assay l done in two parts. The initial reactionin part lis donein 16 x 100 mm glass tubes. In the second part, the pyrophosphate buffer, sample from
part I, and NAD are mixed directly In a precision cell (NSGPrecision Cells, Farmingdale,NY). Fluorescence
is then read In these cells by thefluorometer.
5Glutamlnase (1-glutamineaminohydrolase; EC 3.5.1.2) from Escherichia coIl, 10 U in 1.0 mL of acetate buffer.
Additionof glutaminaseafterthe Incubation(1-4)and coldTCA (1-5)was demonstratedto have noeffectonthe results; giutaminasewas thereforenot added
to thustobe.
d Glutamate dehydrogenase I.-glutamate:NAD(P)
oxidoreductase(EC 1.4.1.3)).
TCA, trichioroaceticacid.
1060 CLINICAL CHEMISTRY, Vol. 39, No. 6, 1993
was assayed immediately (day 0). The remainder of each
solution was then separated, stored at -70 #{176}C,
and
assayed at various intervals until a significant decrease
in the glutamine concentration was observed.
Biological Samples
Plasma. Blood from a healthy
evaluate the assay in plasma.
volunteer was used to
Increasing
glutamine
concentrations were added to aliquots of plasma and
assayed immediately. Fresh blood from three healthy
volunteers was drawn into heparini.zed tubes and the
plasma separated by centrifugation
at 4#{176}C;
all procedures were done with the tubes on ice. Glutamine and
glutamate were assayed immediately.
Aliquots of each
plasma sample were stored at -70 #{176}C
and assayed at
intervals as indicated in the text. Samples were kept
frozen until the respective time of assay.
Tissues. Lund (18) suggested that deproteinization of
plasma with perchloric acid should be followed by immediate
neutralization
with
potassium
hydroxide;
Se-
bolt and Weber (20) and Quesada et al. (21) utilized this
concept for tissue extractions. Results reported by Shih
(16), however, suggested that glutamine was more stable at pH <2. The stability decreased as pH increased,
and the acid hydrolysis product-pyroglutamic
acidbegan to appear. Initially,
homogenization
with 40 gIL
sulfosalicylic
acid (SSA; Sigma Chemical Co.) was used
because of its successful utilization
for extraction of
tissues for determination
of other amino acids and
polyamines for HPLC analysis. The fluorescence background was high, however, and we attempted no stability studies with samples so treated. We then tried
homogenizing
tissues in 50 g/L cold TCA (6 mLfg tissue), using a Polytron tissue homogenizer (Brinkmann
Instruments,
Westbuiy, NY). The homogenate was then
centrifuged at 100 000 x g for 45 mm at 4#{176}C,
and the
clear supernate was assayed as described in Table 1.
This procedure was repeated with the initial precipitate
and then repeated a second time; the glutainine concentration in the clear supernate was determined to evaluate the recovery
of glutamine
50
40
>..
0
30
0
20
Cs
Cs
10 -
ever, the glutamine
concentration (91.12% ± 1.72% of
Aqueous
0
5%TCA
0
0.0
0.5
1.0
1.5
Glutamine concentration (mmol/L)
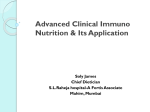
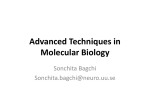
Fig. 1. Unearityofglutammneconcentrationwhenformulatedin sterile
water or a 50 g/L TCA solution on detectionby fluoromettic analysis
The detection of glutammnewas linear up to 0.8 mmol/L for the aqueous
solution (r2 = 98.7, p = 0.0001)
wIth
a mean ± SD CVof 2.41% ± 0.79%.
Dissolvingglutamine in 50 g/L TCA had no effect on assay values
the initial concentration) was significantly (P = 0.0009)
lower than that of the respective aqueous solution.
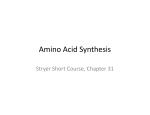
The expected and observed concentrations
in plasma
when increasing amounts of glutamine were added are
shown in Figure 3. Glutamine assayed in plasma was
equal to that expected from the sum of the original
plasma concentration
and the amount added (r2 =
0.99975).
The stability of glutammne in plasma from three
normal male volunteers
was evaluated
(data not
shown). Although the initial concentration varied
among individuals
(785, 636, and 809 A.moI/L), the
glutainmne concentrations
measured in stored plasma
(as a percentage of the initial value) were stable for >1
year at -70#{176}C
(data not shown).
The recovery of glutamine from tumor (n = 8) and
liver (n = 3) tissue after extraction with 50 g/L TCA (6
mL/g) was evaluated as well as the effect of storage of
C
0
125
Aque
-0-rCA
C)
...0
of 2.41% ± 0.79%. Assaying glutamine dissolved in 50
g/L TCA solution did not change the results.
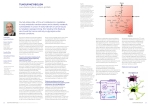
The effect of storage conditions (time and diluent) on
the stabifity of the solutions (as a percentage of day 0
concentration) is shown in Figure 2. Glutamine formulated as an aqueous solution and stored at -70 ‘C was
stablefor at least 16 days (97.94% ± 2.14% of the initial
concentration). When formulated in the TCA solution,
the glutamine concentration was stable for 6(98.64% ±
1.86%) and 8 days (96.34% ± 2.72%). By day 16, how-
a
LJ
in 50 g/L TCA.
Results
The effect of increasing glutamine concentrations in
aqueous and 50 g/L TCA solutions on the relative
intensity is shown in Figure 1. The amount of glutamine
detected was linear up to 0.8 mmoIJL for the aqueous
solution (r2 = 0.987, P = 0.000 1) with a mean (± SD) CV
I1
-
to
100 1
wE
ace
:i1
‘
ab
75
0
10
20
Days of storage
FIg. 2. Effectof storagetime on the stabilityof glutammne
formulated
in sterilewater (n = 5) or 50 g/L TCA (n = 5)
The respectivesolutions wereformulatedandassayedimmediatelyor stored
at -70 ‘C for the indicated number of days. The percentage of Initial
concentrationremainingat eachtimepointwascalculated;the mean ± SD Is
reported.(a) The glutamlne concentration of the aqueous solution differs
significantly (P = 0.015) fromthat in TCA solution on day 14 afterformulation.
( The glutammne
concentrationofthe TCA solutiondifferssignificantlyfrom
thatin the aqueous solutionon day 16 after formulation (P = 0.0009) andfrom
the initial glutamineconcentration
formulatedin TCA (P = 0.0011).
The
concentrationof glutamine formulated in sterile water at day 16 was equal to
that at day 0(P= 0.13)
CLINICALCHEMISTRY, Vol. 39, No. 6, 1993
1061
tered by Khan et al. (22), who demonstrated that the
absorbance of SSA was significant at 340 nm, the
maximum
wavelength of absorbance for NADH. These
authors demonstrated that, although this problem could
1.5
-J
0#{176}
1.0
Cs
0“-C
0.5
too
00
0.0
0.0
1.0
0.5
Expected
1.5
Iutamlne
concentration
(mmol/L)
Fig.. 3. EffIciencyof the determination of glutamine in plasma
Increasing concentrations of glutamine were added to a plasmasample of
known glutamineconcentration and assayed spectrofiuoiometrIcalIy. The
glutamine
assayed Inplasma
was 97% of that expected (r2 = 0.99975)
the supernate at -70 ‘C for 7 days; the results are
shown in Table 2. The mean recovery of glutamine from
the first of three extractions was 88.6 1% from tumor and
90.20% from liver. Glut.amine was stable at -70#{176}C
in
the tumor tissue extract for at least 7 days. The pH of
the initial supernate from the homogenization of liver
and tumor was 1.53.
Discussion
The importance of glutamine as a nutrient for parenteral and enteral formulas has been shown repeatedly
(1-3). Our results (4) show that when arginine in total
parenteral nutrition is replaced with ornithine the
plasma concentrations of glutamine will increase; replacing arginmne with citrulline
has no effect. The ability to efficiently determine glut.ainine concentrations in
plasma and tissues is, therefore,
important
to the understanding of the effects of nutritional manipulations.
Our original objective was to evaluate the effect of
different acids for tissue homogenization and to determine the best neutralization method for efficient analysis of glut.amine in plasma and tissues. For tissues, we
first used a 40 gIL SSA solution because of its wide use
in the determination
of other amino acids. However,
SSA resulted in a high fluorescence background, and its
use was discontinued.
This problem was also encoun-
be reduced by increasing the measurement wavelength
to 355 nm, the sensitivity for detection of NADH was
also decreased. The spectrum for SSA was not established for our conditions, but the problem of decreased
sensitivity would be critical. Given the interference of
SSA at 340 nm and the probable decreased sensitivity
for glutamine at 355 nm, we used TCA in subsequent
experiments for tissue extraction.
An important observation was that neutralization
after TCA extraction of tissues was not necessary. This
significantly
decreased the processing time for each
sample and also reduced the overall error contributed by
dilution. The pH of the supernate from the TCA extraction of liver and tumor was lower than previously
reported, suggesting
that glutamine is stable under
acidic conditions. The present results are in agreement
with Herskowitz et al. (15) and Shih (16), who showed
that glutamine is stable under acidic conditions for 5
days if stored at -70 ‘C. Khan et al. (22) demonstrated
that glutamine was stable for -8 days after extraction
of plasma with SSA (40 g/L).
The plasma concentrations for male volunteers as
determined by our assay, as well as the accuracy of the
assay, correspond well with those reported
for other
methods of glutamine analysis (15, 16, 23). Our results
suggest that glut.amine in plasma is stable for at least
12 months when stored at -70 ‘C. The glutamine
concentrations in rat liver (Table 2) are lower than those
reported by Sebolt and Weber (20), whereas the concentrations in the sarcoma (Table 2) correspond with the
values reported (20) for medium to rapidly growing
hepatomas.
The sarcoma used was a transplantable
tumor, which grows exponentially
(24).
The results in this report, therefore, suggest that
glutamine is stable when appropriate, well-defined storage conditions are used. Tissues may be extracted for
glutamine
analysis with 50 g/L TCA without subsequent neutralization.
The spectrofluorometric analysis
of glutamine allows analysis of a small amount of
plasma (25 L) and tissue (200 mg) with acceptable
accuracy.
Table 2. EfficIency of ExtractIonof Glutamlne from Rat
Tumor and Uver TlssuV
Mean ± SD after extraction
s-i
&mol/gtissue
Tumor (n = 8)
1.37 ± 0.44
(1.38 ± 0.42)0
Liver (n = 3)
3.41
±
0.20
References
p-i
Sot total
88.6
(89.4
±
±
1.9
2.2)
90.2
±
0.4
pmoi/g tissue
S of total
0.18 ± 0.05
(0.17 ± 0.06)
11.4
0.37
±
0.40
±
1.9
(10.7 ± 2.2)
9.8
±
0.4
OnIy results for the initial supemate (S-i) and pellet (P-i) are shown.
Subsequent extractions of pellet yielded negligible glutamine concentration.
0The concentrations assayed after 7-10 daysof storage at -70#{176}C
are
listed in parentheses.
1062 CLINICAL CHEMISTRY, Vol. 39, No. 6, 1993
Supported by grants from Clintek Technologies, DeerfIeld, IL,
and the Department of Health and Human Services, NCI CA34465.
1. Klimberg VS, Souba WW, Salloum EM, Plumley DA, Cohen
FS, Dolson DJ, et al. Glutamine-enriched diets support muscle
glutamine
metabolism without stimulating tumor growth. J Surg
Res 1990;48:319-23.
2. Chance ‘NT, Can L, Fischer JE. Response of tumor and host to
hyperaliment.ation and antiglutamine treatments. J Parent Ent
Nutr 1990;14:122-8.
3. Hammarqvist F, Wernerman J, All R, von der Decken A,
Vinnars E. Mdition of glutamine to total parenteral nutrition
after elective abdominal surgery spares free glutamine in muscle,
counteracts the fall of protein synthesis,and improves nitrogen
balance. Ann Surg 1989;209:455-61.
4. Grossie VE Jr, Nishioka K, Ajani JA, Ota DM. Substituting
ornithine for arginine in total parenteral nutrition eliminates
enhanced tumor growth. J Surg Oncol 1992;50:161-7.
5. Tachabana K, Mukai K, Moriguchi S, Takaina S, Kishino K.
Evaluation of the effect
of arginine-enrichedamino acid solutions
on tumor growth. J Parent Ent Nutr 1985;9:428-34.
6. GosekiN, Endo M, OnoderaT, Kosaki G. Influenceof L-methionine-deprived total parenteral nutrition on the tumor tissue and
plasma amino acids fraction and the host metabolism:experimental study with Sate lung carcinoma-bearing rats. Tohoku J Exp
Med 1989;157:251-60.
7. Martensson J, Larsson J, Schildt B. Metabolic effect of amino
acid solutions in severelyburned patients: with emphasison sulfur
amino acid metabolism and protein breakdown. J Trauma 1985;
25:427-32.
8. Tayek JA, Bistrian BR, Hehir DJ, Martin R, Moldawer LL,
Blackburn GL. Improved protein kinetics and albumin synthesis
by branched-chain amino acid-enriched total parenteral nutrition
in cancer cachexia. A prospective
randomized crossover trial.
Cancer 1986;58:147-57.
9. Mon E, Hasebe M, Kovayashi K Effect of total parenteral
nutrition enriched in branched-chain amino acids on metabolite
levels in septic rats. Metabolism 1988;37:824-30.
10. Hunter DC, Weintraub M, Blackburn GL, Bistrian BR.
Branched chain amino acidsas the protein component of parenteral nutrition in cancer cachexia. Br J Surg 1989;76:149-53.
11. Mon E, Hasebe M, Kobavashi K, Suzuki H. Immediate stimulation of protein metabolism in burned rats by total parenteral
nutrition enriched in branched chain amino acids.J Parent Ent
Nutr 1989;13:484-9.
12. Smith RJ. Glutamine
metabolism and its physiologicimportance. J Parent Ent Nutr 199o;14:40S-448.
13. Greenstein JP, Winitz M. Glutamic acid and glutamine. In:
Chemistry ofthe amino acids. New York: John Wiley & Sons,Inc.,
1961:1933-4.
14. Gilbert JB, Price YE, Greenstein JP. Effect of anions on the
nonenzymatic desanudation of glutamine. J Biol Chem 1949;180:
209-48.
15. Herskowitz K, Baumgartner TG, Austgen TB., Chen MK,
Souba WW. Stability and sterility of glutamine in solution [Abstract]. J Parent Ent Nutr 1990;14:198.
16. Shih FF. Analysis of glutamine, glutamic acid, and pyroglutamic acid in protein hydrolysates by high-performance
liquid
chromatography.J Chromatogr 1985;322:248-56.
17. RosenblumR. Stability of glutamine in vitro. Proc Soc Exp
Biol Med 1965;119:763-5.
18. Lund P. UV-method with glutaminase and glutamate dehydrogenase.In: BergmeyerHIJ, ed. Methods of enzymatic analysis,
Vol. 8, 3rd ed. New York: Academic Press, 1974:357-64.
19. Zar JR. Measure of dispersion and variability. In: Biostatistical analysis, 2nd ed. Princeton, NJ: Prentice-Hall, 1984:31-2.
20. Sebolt JS, Weber G. Negative correlation of L-glutamine
concentrations with proliferation rate in rat hepatomas. Life Sci
1984;34:301-6.
21. Quesada AR, Medina MA, Marques J, Sanchez-Jimenez FM,
de Castro JN. Contribution of host tissues to circulating glutamine
in mice inoculated with Erlich ascites tumor cells. Cancer Res
1988;48:1551-3.
22. Khan K, Blaak E, Ella M. Quantifying intermediate metabolites in whole blood after a simple deproteinization
step with
sulfosalicylic acid. Clin Chem 1991;37:728-33.
23. Stahl A, Frich A, Imier M, Schlienger J-L Enzymatic microassay for bloodglutamine. Clin Chem 1978;24:1730-3.
24. Grossie YB, Nishioka K, Ota DM, Martin RG. Relationship of
erythrocyte polyamines and the growth rate of transplantable
tumors in the rat. Cancer Res 1986;46:3463.-8.
CUNICAL CHEMISTRY, Vol. 39, No. 6, 1993
1063