Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac surgery wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Myocardial infarction wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Drug-eluting stent wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Coronary artery disease wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
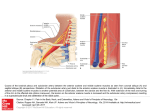
Rom J Leg Med [19] 303-305 [2011] DOI: 10.4323/rjlm.2011.303 © 2011 Romanian Society of Legal Medicine Thrombosis of aberrant right subclavian artery co-existing with infarction of left cerebellar hemisphere: Case report Ivan Stojanović1*, Goran Ilić2, Radovan Karadžić3, Aleksandra Antović4, Miroslav Milić5 _________________________________________________________________________________________ Abstract: Anomalies of the aortic arch and its main branches are rare; estimations from autopsy series indicate a frequency of 3%. The incidence of an aberrant right subclavian artery is up to 0.5% of the population. A putrefied corpse of 59-year old women was found in her locked apartment seating in armchair. The autopsy as a direct cause of death revealed chronic heart failure. The autopsy also revealed aberant right subclavian artery occluded by thrombosis and acute infarction of the left cerebellar hemisphere. The purpose of this report is to describe an unusual case involving acute ischemia of the right upper extremity due to extensive thrombosis of a retroesophageal right subclavian artery (RSA) in a 59-year-old woman. In literature was described clinical presentation left hemiparesis caused by right subclavian artery thrombosis and retrograde embolization of thrombus via the common carotid artery to the right middle cerebral artery distribution. In our case, right subclavian artery thrombosis was co-existing with acute encephalomalation of the left cerebellar hemisphere. This may be result of retrograde embolization of thrombus via the left vertebral artery or hypercoagulability of blood with co-existing thrombosis of this two arteries. At autopsy we exclude existance of paradoxal thrombosis via atrial or vetricular septal defect or arterio-venous fistula, and also exclude existance of a thrombosis od left atrial auricula. Key Words: aberrant right subclavian artery, thrombosis, brain infarction, autopsy A nomalies of the aortic arch and its main branches are rare; estimations from autopsy series indicate a frequency of 3%. One of the most common anomalies of the aortic arch is an aberrant right subclavian artery (ARSA). The incidence of an ARSA is up to 0.5% of the population [1]. While presenting different clinical manifestations, 75% of the patients remain asymptomatic [2]. In 80% of the cases, the ARSA runs between the spinal column and the esophagus, in 15% of the cases between the esophagus and the trachea, and in 5% of the cases ventrally of the trachea [2, 3, 4, 5, 6]. Compression of the esophagus due to a retroesophageal course of the ARSA may produce difficulty in swallowing. This phenomenon was termed dysphagia lusus naturae (“dysphagia by freak of nature”) by David Bayford in 1794 and has since come to be known as dysphagia lusoria [7, 8]. Other simtoms of ARSA are hoarseness, airway (trachea) obstruction, stridor, apnea, cyanosis, and recurring infection. 1)* Corresponding author: MD, student of post graduate studies on Medical Faculty of Nis; Institute of Forensic Medicine, Medical Faculty, University of Nis, Serbia, Address: Dr Zorana Đinđića blv. 81, 18000 Nis; Serbia; Phone: +381-63-8141172 and +381-18-4530824; E-mail: [email protected] 2) Professor, MD, PhD; Institute of Forensic Medicine, Medical Faculty, University of Nis, Serbia 3) Professor, MD, PhD; Institute of Forensic Medicine, Medical Faculty, University of Nis, Serbia 4) Associate Professor, MD, PhD; Institute of Forensic Medicine, Medical Faculty, University of Nis, Serbia 5) MD; Institute of Forensic Medicine, Medical Faculty, University of Nis, Serbia 303 Stojanović I et al Thrombosis of aberrant right subclavian artery co-existing with infarction of left cerebellar hemisphere Case report In the following we present the forensic investigations and technical examinations in chronological order. History: A putrefied corpse of 59-year old women was found in her locked apartment seating in armchair. Notable in the patient’s history was the fact that she had been previously diagnosed diabetes mellitus and arterial hypertension were reported. Simptoms as difficulty in swallowing, hoarseness or stridor was not documented. Autopsy: The autopsy as a direct cause of death revealed chronic heart failure (left ventricular hypertrophy with dilatation of the heart and cardiac fibrosis). The autopsy also revealed that a right subclavian artery was run between the spinal column and the esophagus figure 1 [6], and take retroesophageal course to the right arm. Aberant right subclavian artery (ARSA) was occluded by thrombosis. Autopsy determine that acute thrombosis of aberrant right subclavian artery - fig. 2 and acute infaction of the left cerebellar hemisphere was in a causal relationship with a direct cause of death. Examination od heart not revealed a atrial or vetricular septal defect or thrombosis od left atrial auricula. Microscopic findings: Pathohistology examination confirmed a acute Figure 1. Schematic drawing of the aortic arch, the ARSA, the trachea encephalomalation of the left cerebellar and the esophagus with a retroesophageal course of the ARSA. hemisphere and acute thrombosis of aberrant right subclavian artery. Toxicology findings: Determine a ethyl-alcohol in blood in concentracion of 0,30‰ (6,51 mmol/L). Figure 1. Acute thrombosis of ARSA - autopsy finding. Discussion Thrombosis of a subclavian artery is an uncommon cause of acute upper extremity ischemia in the elderly. Malformations of the aortic arch system are also rare [9]. The purpose of this report is to describe an unusual case involving acute ischemia of the right upper extremity due to extensive thrombosis of a retroesophageal right subclavian artery (RSA) in a 59-year-old woman, that was in a causal relationship with a direct cause of death. ARSA was run between the spinal column and the esophagus, as in maioriti of all cases [2, 3, 4, 5]. In literature was described clinical presentation left hemiparesis caused by right subclavian artery thrombosis and retrograde embolization of thrombus via the common carotid artery to the right middle cerebral artery distribution [10]. In our case, right subclavian artery thrombosis was coexisting with acute encephalomalation of the left cerebellar hemisphere. This may be result of retrograde embolization of thrombus via the left vertebral artery or hypercoagulability of blood [11] with co-existing thrombosis of this two arteries. In literature, if associated aneurysmal dilation exists of ARSA, it can present as localized pain in the shoulders, neck, and thorax. Ischemia of the upper left extremity secondary to thromboembolic events has also been described; this can cause rupture of the diverticulum, with fatal 304 Romanian Journal of Legal Medicine Vol. XIX, No 4(2011) consequences[12]. At autopsy we excluded existance of paradoxal thrombosis via atrial or ventricular septal defect or arterio-venous fistula. Autopsy also excluded existance of a thrombosis od left atrial auricula as a posible cause of dissemaned thrombosis of arteries. References 1. Stewart JR, Kincaid OW, Edwards JE. An atlas of vascular rings and related malformations of the aortic arch system. Springfield, MA: Charles C. Thomas, 1964, p 53. 2. Austin EH, Wolfe WG. Aneurysm of aberrant subclavian artery with a review of the literature. J Vasc Surg 1985; 2: 571–7. 3. Felson B. Ruptured anomalous right subclavian artery: aneurysm or diverticulum? Semin Roentgenol 1989; 24: 121–6. 4. Inzunza O, Burdiles A. Aberrant subclavian artery. International Journal of Morphology 2010 December; 28(4): 1215-9. 5. Fazan V.P.S., Ribeiro R.A., Ribeiro J.A.S., Rodrigues Filho O.A. Right retroesophageal subclavian artery. Acta Cirurgica Brasileira 2003; 18 suppl. 5: 54-6. 6. Stork T, Gareis R, Krumbholz K and Eichstadt H. Aberrant right subclavian artery (arteria lusoria) as rare cause od dysphagia and dyspnea in a 79-year old women with right mediastinal and retrotracheal mass, and co-existing coronary artery disease. VASA 2001; 30: 225-8. 7. Autenrieth D. Dysphagia lusoria. Arch Physiol 1807; 7: 145–88. 8. Bayford D. An account of a singular case of obstructed deglutition. Memoirs Med Soc London 1794; 2: 275–86. 9. Boas N, Desmoucelle F, Bernadet V, Franceschi JC. Rare cause of acute ischemia of the right upper extremity: thrombosis of a retroesophageal subclavian artery. Ann Vasc Surg. 2002 May;16(3):387-90. Epub 2002 May 22. 10. Lee TS, Hines GL. Cerebral embolic stroke and arm ischemia in a teenager with arterial thoracic outlet syndrome: a case report. Vasc Endovascular Surg. 2007 Jun-Jul;41(3):254-7. 11. Mary C Mancini, MD, PhD, Professor and Chief, Cardiothoracic Surgery, Department of Surgery, Louisiana State University Health Sciences Center-Shreveport. Subclavian Artery Thrombosis. eMedicine Specialties, Thoracic Surgery, Vascular. Updated: Jan 15, 2008. 12. Fernández-Lahera J, Gómez Mendieta MA, Mayoralas Alises S, and Díaz Lobatoa S. Aberrant Left Subclavian Artery Associated With Kommerell’s Diverticulum: Chance Finding in a 75-Year-Old Patient. Arch Bronconeumol. 2005;41(1):57-8. 305