Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Fetal origins hypothesis wikipedia , lookup
Compartmental models in epidemiology wikipedia , lookup
Patient safety wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Race and health wikipedia , lookup
Preventive healthcare wikipedia , lookup
Epidemiology wikipedia , lookup
Public health genomics wikipedia , lookup
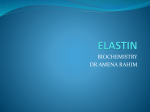
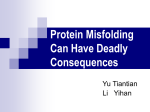
CONTINUING EDUCATION Special Needs Populations: Perioperative Care of the Patient With Creutzfeldt-Jakob Disease MARK KARASIN, BSN, BA, RN 2.6 www.aorn.org/CE Continuing Education Contact Hours Accreditation indicates that continuing education (CE) contact hours are available for this activity. Earn the CE contact hours by reading this article, reviewing the purpose/goal and objectives, and completing the online Examination and Learner Evaluation at http://www.aorn.org/CE. A score of 70% correct on the examination is required for credit. Participants receive feedback on incorrect answers. Each applicant who successfully completes this program can immediately print a certificate of completion. AORN is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. Event: #14540 Session: #0001 Fee: Members $20.80, Nonmembers $41.60 The CE contact hours for this article expire October 31, 2017. Pricing is subject to change. Purpose/Goal To provide the learner with knowledge specific to caring for the surgical patient who has or is suspected of having Creutzfeldt-Jakob disease (CJD). Approvals This program meets criteria for CNOR and CRNFA recertification, as well as other CE requirements. AORN is provider-approved by the California Board of Registered Nursing, Provider Number CEP 13019. Check with your state board of nursing for acceptance of this activity for relicensure. Conflict of Interest Disclosures Mark Karasin, BSN, BA, RN, has no declared affiliation that could be perceived as posing a potential conflict of interest in the publication of this article. The behavioral objectives for this program were created by Rebecca Holm, MSN, RN, CNOR, clinical editor, with consultation from Susan Bakewell, MS, RN-BC, director, Perioperative Education. Ms Holm and Ms Bakewell have no declared affiliations that could be perceived as posing potential conflicts of interest in the publication of this article. Sponsorship or Commercial Support No sponsorship or commercial support was received for this article. Objectives 1. 2. 3. 4. 5. Describe prions as they relate to CJD. Discuss the etiology of the types of CJD. Discuss the symptoms of CJD. Compare the different methods for diagnosing CJD. Describe perioperative considerations for a patient who has or is suspected of having CJD. Disclaimer AORN recognizes these activities as CE for RNs. This recognition does not imply that AORN or the American Nurses Credentialing Center approves or endorses products mentioned in the activity. http://dx.doi.org/10.1016/j.aorn.2014.06.018 390 j AORN Journal October 2014 Vol 100 No 4 Ó AORN, Inc, 2014 Special Needs Populations: Perioperative Care of the Patient With Creutzfeldt-Jakob Disease 2.6 MARK KARASIN, BSN, BA, RN www.aorn.org/CE ABSTRACT Creutzfeldt-Jakob disease (CJD) is a rare but lethal prion disease. The worldwide mortality rate of CJD is 1.67 per one million people, although 90% of cases will lead to death within one year of symptom onset. Rapid, progressive dementia is the cardinal sign of CJD. Other early symptoms include deterioration of muscle coordination, memory, judgment, and vision, as well as personality changes, insomnia, and depression. It occurs in two types, classic and new variant, and classic CJD can be further divided into three subtypes: sporadic, familial (ie, genetic), and iatrogenic (ie, health care associated). Surgery often requires using instruments that come in contact with high-infectivity tissue, especially during neurosurgical procedures and diagnostic biopsies. To reduce the risk of disease transmission, infection control practices should include identification of the risk of infection, implementation of safety protocols (eg, use of personal protective equipment), proper selection and use of instrumentation, and adequate disinfection and sterilization practices. Silent carriers, risks of iatrogenic infection, and the possibility of inadvertent exposure of healthy patients may carry great liability to public health and hospital stability. AORN J 100 (October 2014) 391-407. Ó AORN, Inc, 2014. http:// dx.doi.org/10.1016/j.aorn.2014.06.018 Key words: Creutzfeldt-Jakob disease, CJD, prion, neurosurgery, diagnostic biopsy, infection prevention, disinfection and sterilization. C reutzfeldt-Jakob disease (CJD) occurs in approximately one out of every one million people in the general worldwide population every year.1 The rarity of this condition, however, should not permit health care providers to underestimate the magnitude of the problems that CJD poses because of its distinguishing infection control resistance, modes of transmission, and invariable lethality. The uncommonness of the disease and its associated stigma and fears have created a knowledge gap among health care providers that can lead to inadequate care of patients http://dx.doi.org/10.1016/j.aorn.2014.06.018 Ó AORN, Inc, 2014 October 2014 Vol 100 No 4 AORN Journal j 391 October 2014 Vol 100 No 4 who are diagnosed with or suspected of having CJD.2,3 The purpose of this article is to close this gap by exploring the pathophysiology, varieties, symptoms, and incidence of CJD as well as focusing on the perioperative implications of caring for patients with CJD who are undergoing surgery and examining unique perspectives of infection control practices specific to CJD. PATHOPHYSIOLOGY In 1997, Stanley B. Prusiner received the Nobel Prize in Physiology or Medicine for his discovery of prions, which represented a new biological principle of infection.4 Prusiner coined the term prion to denote proteinaceous infectious particles that lack nucleic acid and therefore cannot reproduce, which separates this type of infection from other pathogens (eg, bacteria, viruses).5 A prion is a form of protein found throughout the body, with the highest concentration in the central nervous system.6 Normal cellular configuration of this protein, referred to as PrPC, does not cause pathology; although its function is not completely understood, researchers believe that PrPC plays a role in copper ion management of nerve transmissions and in protecting the brain from degenerative diseases of old age, such as dementia.5 When PrPC misfolds (ie, changes shape) as a result of genetic or external variables, the prion’s secondary and tertiary structures change into an abnormal form called the scrapie isoform (PrPSc) of the prion protein.5,7 Instead of reproducing, this malformed prion multiplies by acting as an infectious agent that binds itself to nearby normal proteins and converting them into the abnormal form. Accumulation of these malformed proteins leads to degeneration of neural tissue. Although researchers do not completely understand this mechanism of neuron damage, referred to collectively as transmissible spongiform encephalopathies (TSEs), it causes fatal prion diseases among animals and humans.7,8 The genetic variability of the prion protein gene (ie, PRNP) is what leads to diversity in phenotypic expression that in turn results in a variety of 392 j AORN Journal KARASIN abnormal prions and their associated diseases. Figure 1 provides a diagram of human and animal prion diseases that are currently known.9 Each of the listed diseases is clinically important; however, it is essential to focus on those that health care providers in the developed world are more likely to encounter. The sporadic form of the prion diseases accounts for 90% of all cases of human prion disease.10 Thus, this article focuses on CJD, the most common form of the sporadic prion diseases. TYPES OF CJD AND ETIOLOGY There are two types of CJD: classic or new variant (vCJD). Together, they account for a worldwide mortality rate of 1.67 per one million people.11 Table 1 describes the three subtypes of classic CJD: sporadic (sCJD), familial or genetic (fCJD), and iatrogenic (iCJD).7,12 sCJD The majority of CJD cases are sCJD, and the cause remains unknown. Hans Gerhard Creutzfeldt, MD, and Alfons Maria Jakob, MD, first recognized the disease in the 1920s. Since then, there has been no evidence of human-to-human transmission.13 The disease is the result of spontaneous conversion of the normal prion protein into its abnormal form. The average age at onset of sCJD is between 50 and 70 years, although there are recorded cases of patients as young as 21 years of age and as old as 80 years of age.13-15 Although the disease can be present but silent for decades, most people with sCJD die within one year of symptom onset. fCJD The familial component of fCJD is misleading because more than 50% of patients with fCJD report no family history of the disease. Therefore, the new term genetic CJD (gCJD) is being used with this subtype of CJD, although it has yet to become official.16 The condition arises from a mutation in the PRNP gene, and its occurrence is clustered in European countries, Japan, Libya, Israel, and Chile.17-19 The National Prion Disease SPECIAL NEEDS POPULATIONS: CJD www.aornjournal.org Figure 1. A diagram showing the disease names and abbreviations of spongiform encephalopathies. Pathology Surveillance Center reports that the median age at death of people with fCJD depends largely on the type of mutation but tends to range from 35 to 55 years. The time frame of the illness is more extended than that of sCJD, ranging from a few months to up to five years (e-mail communication, Katie Glisic, executive assistant to Pierluigi Gambetti, MD, professor and director, National Prion Disease Pathology Surveillance Center, Case Western Reserve University, March 25, 2014). iCJD Prion resistance to routine sterilization methods has led to transmission of CJD via medical interventions (ie, health care associated), which is classified as iCJD. The Centers for Disease Control and Prevention (CDC) reports that iCJD has affected more than 250 patients worldwide.20 Of those, only six cases have been linked to contaminated neurosurgical instrumentation and stereotactic electroencephalography depth electrodes. The AORN Journal j 393 October 2014 Vol 100 KARASIN No 4 TABLE 1. Subtypes of Classic Creutzfeldt1 Jakob Disease Subtype Occurrence Sporadic 85% to 90% Familial 10% to 15% Iatrogenic < 1% Cause/transmission Idiopathic Familial (ie, genetic) Medical interventions (ie, health care associated) 1. Belay ED, Blase J, Sehulster LM, Maddox RA, Schonberger LB. Management of neurosurgical instruments and patients exposed to Creutzfeldt-Jakob disease. Infect Control Hosp Epidemiol. 2013;34(12):1272-1280. rest were linked to human growth hormone, dura mater, and corneal graft implants that were derived from infected cadavers.21 It is also important to note that anyone with LyoduraÒ dural products that were implanted before May 1987 may be at risk for iCJD throughout their life.12 Furthermore, in the past 15 years, nearly 5,000 patients have been informed of possible exposure to CJD because the same surgical instruments that were used in their procedure were previously used in infected patients.22-24 Despite such events, there are still conflicting data about previous surgery being a risk factor for iCJD, possibly because the incubation period (ie, time from infection to onset of symptoms) can range from one year to 30 years or longer.25,26 Adding to this challenge is that iCJD can strike anyone exposed to contaminated instruments and can vary in its presentation, depending on the source of the original infection and route of transmission, making it difficult to assess patients’ survival time frame and their age. It does, however, currently hold a world record among all iatrogenic diseases for incubation period, which can be as long as 42 years.27,28 vCJD It is important to differentiate classic CJD with its three subtypes from vCJD, a condition that was first reported in 1996 and has since claimed the lives of 228 people worldwide.29 This disease develops 394 j AORN Journal from consumption of meat that is contaminated with bovine spongiform encephalopathy (BSE), a cattle form of the prion disease commonly referred to as “mad cow disease.” The median age at death of patients with vCJD in the United Kingdom is 28 years.30 Worldwide efforts at curbing the BSE epidemic of the 1990s led to numerous laws and regulations that control cattle feed and processing, which are aimed at eliminating the chance of acquiring vCJD.31 Despite such interventions, one study has recognized that one in 2,000 people in the United Kingdom may still be silent carriers of the disease.32 In the United States, the latest case of vCJD was confirmed in June 2014 in Texas.33 In the same month, 4,000 lb of beef were recalled because of a remote risk of CJD contamination as a result of paperwork irregularities.34 Furthermore, there are data showing transmission of vCJD through blood product transfusion.32 Although researchers have developed a prototype blood test for symptomatic vCJD, there are no such methods for detecting it in asymptomatic populations.35 This shortcoming has pushed a global movement to protect the blood supply, resulting in more rigorous screening practices for high-risk donors. Some of these include exclusion of anyone who has lived in or traveled to the United Kingdom during the BSE epidemic, anyone who has received pituitary growth hormone or dura mater transplants, and anyone with a family history of CJD.36 CLINICAL PRESENTATION The cardinal sign of CJD is rapidly progressive dementia. Other early symptoms include deterioration of muscle coordination, memory, judgment, and vision, which may accompany personality changes, insomnia, and depression. Late symptoms include myoclonus, blindness, aphasia, ataxia, and coma. Different types of CJD may present a variety of symptoms and survival rates; however, 90% of cases will lead to death within one year of onset of symptoms.37 SPECIAL NEEDS POPULATIONS: CJD DIAGNOSIS Diagnosis of CJD is not without complexities because of how closely it may mimic Alzheimer or Huntington disease.37 When a patient presents with rapidly progressive dementia, the diagnostic process typically starts with identification of one of several differential diagnoses. Other reversible conditions are ruled out first and may include a wide spectrum of “neurodegenerative, autoimmune, infectious, and toxic-metabolic etiologies.”38(p47) Most important to this process is for health care professionals to obtain a detailed history from the patient and his or her family members and to perform a physical examination, because an inaccurate history, especially relating to the time frame of symptoms, may lead to misdiagnosis (eg, viral encephalitis).38 Although tissue biopsy or autopsy remains the gold standard for definitive diagnosis, minimally invasive methods with proper interpretation have been quite effective. In reporting on diagnostic criteria, Zerr et al39 found that changes in the patient’s magnetic resonance imaging scan were accurate in 81% of patients with sCJD, identification of the presence of 14-3-3 protein in the patient’s cerebrospinal fluid resulted in sensitivity of 86%, and the presence of specific peaks on electroencephalography readings, although significantly lower, resulted in sensitivity of 38%. However, combining the three diagnostic results proved to be 99% sensitive for a correct diagnosis.39 Although studies have described a blood-based assay test for vCJD, there are no definitive screening methods for asymptomatic populations.35,37 TREATMENT There has been a remarkable increase in scientific contributions to CJD research, yet its treatment remains elusive and the illness is still invariably fatal. Doxycycline has proven effective in prolonging CJD survival in vitro and in vivo, but these results were not found to be reproducible in a randomized, double-blind, placebo-controlled study.40 Recently, there has been progress in the treatment of CJD in mouse models. New bioengineered www.aornjournal.org antibodies against prions have shown positive results in the early stages, which provides direction for future research.41 What makes the fight against CJD even more challenging is that its prolonged incubation period can be up to 50 years before symptoms appear. INFECTION CONTROL PRACTICES Considering that the pathology of CJD prions is always fatal, there is a need for proper infection control practices.42 The components are identifying the risk of infection, implementing safety protocols to include use of personal protective equipment, proper selection and use of instrumentation, and adequate disinfection and sterilization practices. Risk of Infection In March 1999, the World Health Organization (WHO) published guidelines for infection control of TSEs. Although more than a decade has passed since then, the latest reports on health care practices relating to patient care, disinfection, and sterilization align for the most part with the WHO guidelines.42-44 One update that calls for closer examination, however, is the 2006 WHO report on TSE tissue infectivity ratings. This report categorized tissues by high infectivity, low infectivity, and no detectable infectivity (Table 2).45 Safety Protocols Selection of proper personal protective equipment depends on the type of care being provided and the kind of tissue and fluid (eg, pituitary gland tissue versus uterine tissue) that is being handled. According to the WHO, isolation of patients who have or are suspected of having CJD is not required and only standard universal precautions have to be maintained during routine nursing care.43 Special provisions have to be taken, however, when handling high-infectivity tissues and cerebrospinal fluid. Therefore, if a patient with CJD or a suspected diagnosis of CJD arrives in the preoperative AORN Journal j 395 October 2014 Vol 100 KARASIN No 4 TABLE 2. Levels of Tissue Infectivity in Transmissible Spongiform Encephalopathies High infectivity n n n n n n n n Brain Spinal cord Retina Optic nerve Spinal ganglia Trigeminal ganglia Pituitary gland Dura mater Low infectivity n n n n n n n 1 No detectable infectivity Peripheral nervous system Lymphoreticular tissues Alimentary tract Placenta Other (eg, lung, liver, kidney, pancreas, bone marrow, skeletal muscle, tongue, blood vessels, nasal mucosa, salivary gland, cornea) Cerebrospinal fluid Blood n n n n Reproductive tissues (ie, except placenta) Musculoskeletal tissues (ie, except skeletal muscle) Other (eg, trachea, skin, adipose, thyroid, mammary) Bodily fluids (ie, except blood, cerebrospinal fluid) 1. WHO Guidelines on Tissue Infectivity Distribution in Transmissible Spongiform Encephalopathies. Geneva, Switzerland: World Health Organization; 2006. http://www.who.int/bloodproducts/TSEPUBLISHEDREPORT.pdf. Accessed May 12, 2014. or postoperative areas with a cranial or lumbar drain in place, the health care provider should n use appropriate personal protective equipment and n dispose of dressings and linens appropriatelyd that is, any item that comes in contact with high-infectivity tissue or cerebrospinal fluid should be placed in biohazard bags processed for incineration. No special handling is required, outside of standard precautions, for items that come in contact with bodily fluids (except cerebrospinal fluid and blood) or excretions or any tissue that has no detectable presence of prions.46 It is also important to note that, according to the WHO, there has not been a single case of CJD as a result of occupational accident or injury.3 These findings are supported by reports from the European Creutzfeldt Jakob Disease Surveillance Network that there is no increased risk of sCJD in health professionals, and analytical studies do not show a clear excess risk for health-related professions.47 Instrumentation, Disinfection, and Sterilization Frequently, surgery requires the use of instruments that come in contact with high-infectivity tissue, especially during neurosurgical procedures and 396 j AORN Journal diagnostic biopsies. The Joint Commission encourages administrators at health care facilities to implement the evidence-based sterilization guidelines as outlined by the CDC, the WHO, the American National Standards Institute, or the Association for the Advancement of Medical Instrumentation.48 In 2000, the WHO reported on prion decontamination protocols for reusable surgical instruments and surfaces43; the CDC has since updated these protocols to reflect the most current evidence (Table 3).44 Recently, there have been exciting developments in materials used to make surgical instruments that, similar to nickel, may significantly decrease the level of protein absorption and residue.49 For example, doped diamond-like carbon coatings may offer potential antifouling surfaces against microbial and protein attachment, which may reduce the risk of patients acquiring iCJD and lead to new instrument manufacturing.49 Until such time, the most effective approach for minimizing prion residual on surgical instruments before thorough disinfection and sterilization is to not allow them to dry for any length of time. Presoaking instruments has been shown to reduce prion-infected tissue contamination by up to 96%.50 The challenge with prion decontamination is that prions are resistant to conventional methods of SPECIAL NEEDS POPULATIONS: CJD www.aornjournal.org TABLE 3. Prion Decontamination Protocols for Reusable Surgical Instruments and Surfaces 1 Three recommended options for decontamination of surgical instruments Surgical instruments should be 1. immersed in 1N or 2N sodium hydroxide (NaOH), placed in an appropriate container, and heated in a gravity-displacement autoclave at 121 C (250 F) for 30 minutes. Clean and sterilize by conventional means. 2. immersed in 1N NaOH or sodium hypochlorite (NaOCl) 20,000 parts per million (ppm) for 1 hour and then rinsed with water, placed in an appropriate container, and heated in a gravity-displacement autoclave at 121 C (250 F) for 1 hour. Clean and sterilize by conventional means. 3. immersed in 1N NaOH or NaOCl 20,000 ppm for 1 hour, rinsed with water, transferred to an appropriate container, and heated in a gravity-displacement autoclave at 121 C (250 F) or, if in a porous load, heated at 134 C (274 F) for 1 hour. Clean and sterilize by conventional means. Recommendations for decontamination of surfaces Surfaces should be n reduced in their gross contamination as a first step because the presence of excess organic material will lessen the strength of either the NaOH or NaOCl solution. n treated with 2N NaOH or NaOCl 20,000 ppm for 1 hour. n monitored to ensure they remain wet for the entire duration of the treatment and then rinsed well with water. Warnings n Do not autoclave NaOH in aluminum containers or in a container that is in contact with aluminum. n Be aware that exposure to NaOH solution may corrode some poor-quality stainless steel instruments. n Be aware that exposure to NaOCl solution corrodes many metal instruments. n Ensure that autoclave containers have rims and lids designed to allow NaOH condensates to collect and drip back into the pan. n Allow the NaOH solution to cool down to ambient temperature before handling using appropriate precautions because NaOH solution is very caustic when hot. 1. Belay ED, Blase J, Sehulster LM, Maddox RA, Schonberger LB. Management of neurosurgical instruments and patients exposed to Creutzfeldt-Jakob disease. Infect Control Hosp Epidemiol. 2013;34(12):1272-1280. Table adapted and printed with permission from the Centers for Disease Control and Prevention. disinfection and sterilization. Such methods are always scrutinized by researchers51 and often prove to be ineffective or to contradict previously published modes of disinfection; however, this scrutiny helps researchers discover new methods of prion decontamination efficacy. For example, the gas plasma of hydrogen peroxide and various enzyme solutions is a recently tested but not yet approved method of disinfection and sterilization.52-55 Another issue is that methods of decontamination are very extensive and therefore can degrade the instruments and produce harmful gases in the process.44 A solution to this may be single-use instruments. In fact, for optimal management of CJD procedures, the WHO recommends the use of disposable surgical instruments that are incinerated postoperatively.43 Although this approach is the most ensured method of reducing the risk of transmission of iCJD, it does not come without challenges. The most common complaint that I gathered through personal interviews with three neurosurgeons is that single-use instruments are of inferior quality (eg, not as sturdy) as nondisposable, reusable instruments. In addition, automated instruments and equipment (eg, drills) are not available as single-use items. Therefore, surgeons who wish to perform a procedure on a patient who has or is suspected of having CJD with single-use instruments must resort to the use of manual controlled drills. These instruments may be difficult to handle or require additional assembly. Furthermore, data from tonsil and adenoid procedures show a higher risk of certain complications (eg, hemorrhage) as a result of using disposable instruments.55,56 However, these barriers are not enough to discourage health care providers from AORN Journal j 397 October 2014 Vol 100 using disposable instruments. Ronald Benitez, MD, from Atlantic NeuroSurgical Specialists, Morristown, New Jersey, stated his agreement with this in a telephone interview (June 20, 2014). He has performed numerous CJD biopsy procedures and has observed an evolution of instrument sets from reusable to disposable and states that “you cannot justify the risk of reusing instruments” for such procedures. Figure 2 provides a sample list of a CJD disposable instrument set used at one neuroscience center. Finally, CDC infection control should involve implementing facility-specific methods for not mixing neurosurgical instruments with other specialty instruments and developing a tracking system for instrument trays used in case of a delayed postoperative CJD diagnosis.44 PERIOPERATIVE IMPLICATIONS Caring for a patient with CJD during all three phases of the perioperative processdpreoperative, intraoperative, and postanesthesia recoverydis complex and has specific implications for nursing. Table 4 describes common CJD symptoms and provides special nursing considerations for each phase of patient care relating to each symptom.57 Just as with any patient undergoing surgery, the perioperative nurse should provide individualized instruction that is dependent on the patient’s specific manifestations of CJD. Preoperative and Postoperative When it comes to perioperative patient-centered nursing care, it is important to learn from those who have experience working with terminally ill patients. Clarissa Rentz, MSN, APRN-BC, explored care of patients with CJD from a hospice and palliative perspective.57 Some of her findings can be translated and expanded on for the perioperative environment, particularly those aimed at patient safety and comfort by ensuring that the perioperative team is aware of the spectrum of possible symptoms and ready to manage them. Although the majority of patients with diagnosed CJD do not leave the hospital, it is not unrealistic 398 j AORN Journal KARASIN No 4 for a patient to decide to return home for the final stages of the disease or for the patient’s family members to make this decision. In this case, emphasis can be placed on patient and family education of prion infection prevention and standard precautions as well as the disease trajectory related to timeline and symptoms. As with any patient care for which family members are at the patient’s bedside, it is imperative to take the holistic approach and not discount psychosocial aspects of family involvement. This approach is even more central to caring for patients with CJD because of the possibility of a diagnosis of fCJD or gCJD. This means that children or other family members of the patient may already know, or will know, that they themselves can develop the disease later in life. Their perception of health care provided to their loved one will form a model of what may be facing them in the future and potentially affect their development and coping mechanisms.58 Intraoperative The WHO43,45 and the CDC8,20 have issued specific and extensive guidelines for decontamination of prion-infected surfaces. The following are intraoperative recommendations and practices reported by some neurosurgical facilities that were shown to significantly lessen the time required for OR personnel to perform proper postoperative cleaning: n Allow only essential items in the room, such as the anesthesia machine, one suction unit, one monopolar/bipolar electrosurgical unit, one back table, one Mayo stand, one sharps container, and one biohazard garbage bag.59 n Cover all pedals and cords with plastic bags and secure them in place.59 n Cover all other equipment, the walls, the bed, and the floor of the working area with sheets of polyvinyl chloride (Figure 3).59,60 Another neuroscience center has used disposable liquidrepellent sheets (eg, surgical drapes and heavyduty surgical table covers) to achieve the same goal. SPECIAL NEEDS POPULATIONS: CJD www.aornjournal.org Figure 2. A sample count list showing a disposable neurosurgical instrument set for treating patients with Creutzfeldt-Jakob disease. AORN Journal j 399 October 2014 Vol 100 KARASIN No 4 TABLE 4. Perioperative Nursing Implications for Patients With Creutzfeldt-Jakob Disease Symptom Aphasia and akinetic mutism Nursing consideration n n Ataxia, abnormal posturing, and rigidity n n n Cortical blindness Dementia syndrome n n n n n n n Dysphagia n Heightened startle reflex, myoclonus, delusions, hallucinations, paranoia, and seizures n n n Incontinence n n Infectivity n n n n n n n n 400 j AORN Journal 1 Speak directly to the patient. Use simple, verbal, step-by-step commands with prompts and visual cues. Maintain the patient’s proper body alignment when transferring and positioning the patient. Communicate to team members that the patient may not be able to cooperate because of the feeling of falling. Sacral dressing for pressure ulcer prevention. Approach the patient from the front and maintain eye contact. Maintain patient dignity by using a holistic team approach when providing care for the patient and his or her family members. Obtain a detailed history from the patient, including information about the patient’s level of physical and mental disabilities, symptoms, and when or if a diagnosis was made. Include the patient’s family members during assessments to help ensure that the patient’s information is accurate. Take into account the psychosocial aspects of family involvement, particularly because children or other family members of the patient may already know, or will know, that they themselves can develop the disease later in life. Obtain test results, including tissue biopsies, magnetic resonance imaging scans, cerebrospinal fluid tests, and electroencephalography. Review the patient’s consents, do-not-resuscitate status, living wills, and powers of attorney. Assist the anesthesia professional with securing an airway and be prepared for airway emergencies. Minimize touching and moving the patient as much as possible. Decrease stimulation by controlling lights, noise, commotion, and frequency and limiting the number of interventions. Maintain patient safety by ensuring that bedside rails are up, providing adequate padding, and keeping safety straps secure. Insert an indwelling urinary catheter if clinically indicated. Use linens and pads as needed. Obtain the surgeon’s completed risk assessment of the patient. Identify the level of tissue infectivity (ie, high infectivity, low infectivity, no detectable infectivity) of the tissue that will be handled during the procedure. Schedule procedures as the last case of the day to allow adequate time for terminal cleaning of the OR postoperatively. Obtain and use the proper personal protective equipment based on the type of care being provided and the kinds of tissue and fluid that are being handled. Enforce practice guidelines for governing infection control and prevention and implementing standard precautions. Implement prion decontamination protocols for equipment and environmental surfaces. Evaluate the pros and cons of using disposable, single-use instruments and equipment. Implement neurosurgical protocols and protocols for other specialties when Creutzfeldt-Jakob disease is suspected or confirmed. If suspected, quarantine the used surgical instruments until a diagnosis is determined for n disinfection or disposal of instruments or SPECIAL NEEDS POPULATIONS: CJD www.aornjournal.org TABLE 4. (continued ) Perioperative Nursing Implications for Patients With Creutzfeldt-Jakob 1 Disease Symptom Nursing consideration n n n n n n n n n n Pyrexia n n n quarantine of reusable equipment for reuse exclusively on the same patient. Implement instrumentation management algorithms for n preventiondthe patient is identified preoperatively to be at high risk for having Creutzfeldt-Jakob disease, n containmentdthe patient is identified intraoperatively to be at high risk for having Creutzfeldt-Jakob disease, and n contingencydthe patient is identified postoperatively to be at high risk for having Creutzfeldt-Jakob disease. Dispose of linens, patient clothing, and wound dressings appropriately (ie, any item that comes in contact with high-infectivity tissue or cerebrospinal fluid should be placed in biohazard bags and processed for incineration). Other than standard precautions, no special handling is required for items that come in contact with bodily fluids (except for blood and cerebrospinal fluid) or excretions and any tissue with no detectable prion presence. Provide transfer-of-care reports at every personnel change to communicate the patient’s diagnosis and care requirements. Perform a time out, during which team members discuss logistics and infection control practices, and assign a facilitator who can be a liaison between the OR suite and other facility departments and address perioperative needs (eg, anesthesia equipment, sterile surgical supplies). Assign the minimum number of team members needed to work on the procedure. Lessen the time required for OR personnel to perform proper postoperative cleaning by n allowing only essential items in the room (eg, the anesthesia machine, one suction unit, one monopolar/bipolar electrosurgical unit, one back table, one Mayo stand, one sharps container, and one biohazard garbage bag); n covering all pedals and cords with plastic bags and securing them in place; and n covering all other equipment, the walls, the OR bed, and the floor of the working area with polyvinyl chloride.2 Obtain and use additional labeling and double bagging to alert those handling specimen containers of its contents and avoid any potential for spillage (eg, prion specimen). Obtain and use disposable laryngoscope blades because of the risk of dormant Creutzfeldt-Jakob disease and the potential for the presence of infective prions in the patient’s salivary glands and tonsils. Provide safe, thorough postoperative care by using all necessary personal protective equipment and infection control practices. Provide discharge planning, if appropriate, that accounts for the transmissibility of infectious prions and provides family or caregivers with education about providing care that reduces the risk of infection and a possible timeline of the disease and its associated symptoms. Monitor room temperature. Use warming or cooling devices as needed. 1. Rentz C. Nursing care of the person with sporadic Creutzfeldt-Jakob Disease. J Hosp Palliat Nurs. 2008;10(5):272-282. 2. WHO Manual for Surveillance of Human Transmissible Spongiform Encephalopathies Including Variant Creutzfeldt-Jakob Disease. Geneva, Switzerland: The World Health Organization; 2003. http://whqlibdoc.who.int/publications/2003/9241545887.pdf. Accessed June 27, 2014. AORN Journal j 401 October 2014 Vol 100 No 4 KARASIN Figure 3. Sheets of polyvinyl chloride should be used to cover the walls of an OR that is prepped for a procedure that will be performed on a patient who has or is suspected of having Creutzfeldt-Jakob disease. These efforts have been shown to facilitate relatively easy disposal of potentially contaminated material.53 Specimen handling for a CJD biopsy does not require special considerations and can follow hospital protocols for routine care.59 Additional labeling and double bagging can be used to alert those handling the container of its contents and avoid any opportunity for spillage.61 Processing of the specimen has to be performed by a trained specialist, usually at the National Prion Disease Pathology Surveillance Center, a hub for all prionassociated diseases and a great resource for health care providers (R. Benitez, verbal communication, June 20, 2014). Anesthesia Anesthesia professionals are challenged when providing anesthesia for a patient who has a diagnosis of CJD or who is suspected of having CJD because of the variety of recommendations from professional organizations. The American Society 402 j AORN Journal of Anesthesiologists recommends using standard precautions and single-use equipment during procedures on such patients.61 A neurosurgical anesthesia publication supports this and suggests that modern disposable instruments and equipment (eg, laryngoscope blades, Magill forceps, dilators, laryngeal mask airways) are just as effective as nondisposable items.28 An important development during the past decade is that ventilators do not need to be quarantined,7 as previously recommended by Farling and Smith.62 Health care providers are challenged when there is a need to use a video laryngoscope, fiberscope, or endoscope during procedures for patients with or suspected of having CJD, especially for difficult intubations. Although the WHO recommends processing such items according to heatsensitive instrumentation methods, a more recent publication from the UK Department of Health dictates that these materials should be destroyed after a single use or quarantined for reuse exclusively on the same patient.42,63 Abnormal prions SPECIAL NEEDS POPULATIONS: CJD have been found in the olfactory epithelium; therefore, nasal fiber-optic intubation would fall into the category of single use.63 Regardless of the approach taken to administer anesthesia, a variety of sources suggest having a system in place to track the use of equipment so that it can be traced in case of future outbreaks of CJD.28,64,65 FACILITY PROTOCOLS FOR CJD Although CJD is a rare condition, the unique set of issues that it poses for infection preventionists and health care providers requires a close examination of any neurosurgical facility’s protocols. Silent carriers, risks of iatrogenic infection, and the possibility of inadvertent exposure of healthy patients may carry great liability to public health and hospital stability. A review of the literature from around the world (especially from Europe and Canada, where vCJD is more prevalent) provides a set of recommendations that may be helpful in managing a confirmed or potential case of CJD. Evaluation of current protocols is of the essence in ensuring that facilities are up to date with current evidence-based practices. A Joint Commission Sentinel Event Alert66 supports this and recommends establishing policies for n disinfection or disposal of instruments used in neurosurgery in general and when CJD is suspected or confirmed and n quarantine of such surgical instruments until an unclear diagnosis or biopsy is clarified. Because of the incubation period and often ambiguous presentation of CJD, it is not always possible to know that the surgical patient has the disease. This brings up the need for contingency management plans. One Canadian health system has provided a summary of necessary actions and instrumentation management algorithms for each scenario: n preventiondthe patient is identified preoperatively to be at high risk for having CJD, n containmentdthe patient is identified intraoperatively to be at high risk for having CJD, and www.aornjournal.org n contingencydthe patient is identified postoperatively to be at high risk for having CJD.67 When deliberating revision of current policies or establishing new ones, it is important to customize them to individual facility needs, but even more imperative is to take a multidisciplinary approach in ensuring that all aspects of patient care, operations management, ethical and legal perspectives, and public health are addressed. This is especially critical in cases where CJD is diagnosed postoperatively in patients not previously known to be at risk. When proper protocols and policies are in place, orchestrating a successful CJD case is still a team approach. Ann Poggioli, RN, BA, CRNFA, is a neurosurgical coordinator at a neuroscience center in New Jersey with such experience. She claims that “communication is vital” when it comes to providing care during a CJD procedure, for which the biggest challenge is “getting all the players on the same page” (verbal communication, March 15, 2014). At Poggioli’s facility, the CJD procedure is not scheduled until the surgeon completes a risk assessment tool (Figure 4). After this tool is processed, the coordinator handles communication with personnel from the infection control, environmental services, central processing, anesthesia, and pathology departments. This aids in effective implementation of infection control practices across all departments and throughout the continuum of care. Preparation of personnel requires special attention. According to the UK Department of Health, “only trained staff, who are aware of the hazards, carry out invasive procedures that may lead to contact with medium- or high-risk tissue.”68 The WHO has expanded on this concept by advising that only the minimum number of people needed be present for the procedure.42 To that end, it may be prudent to hold a huddle meeting with all team members involved in the patient’s care; during this time out, the team should discuss logistics and infection control practices and assign a facilitator AORN Journal j 403 October 2014 Vol 100 KARASIN No 4 Figure 4. The surgeon should complete a Creutzfeldt-Jakob disease (CJD) risk assessment tool before surgery that is scheduled for a patient who has or is suspected of having CJD. who can be a liaison between the OR suite and other facility departments to obtain perioperative needs (eg, anesthesia equipment, sterile surgical supplies).58,69,70 Finally, when scheduling the surgery, the perioperative manager should consider the time required for postoperative terminal cleaning, which may render the OR unavailable. Thus, it may be advisable to schedule CJD cases as the last procedure of the day.70 this article can provide current guidance when facing this scenario and may pose providerreflecting questions, such as the following: CONCLUSION Prion diseases pose complex concerns for all health care professionals and should be approached with caution. Despite the rarity of CJD, it is very likely that members of a neurosurgical team will care for a patient with CJD at some point in their career. When that happens, it is critical to adhere to the most up-to-date, evidence-based practices to ensure proper infection control, operations management, and patient-centered care. Information covered in Perhaps the only clear answer to these questions is that the scientific community is still in the developmental stages related to aspects of CJD, such as screening, ease of disinfection, and types of treatment options. Furthermore, future approaches to surgical procedures are bound to change and will require consistent reevaluation of up-to-date research to ensure proper nursing interventions when caring for a patient diagnosed with or suspected of having CJD. 404 j AORN Journal n Are there systems and policies in place for managing logistics, instrumentation, disinfection, and exposure to prions? n Is the specialty team well educated on the disease process, proper infection control, symptoms, and accompanying nursing considerations? SPECIAL NEEDS POPULATIONS: CJD Acknowledgments: The author thanks Beth Karasin, BSN, RN, CNOR, RN first assistant, for providing the topic and the courage to write about it; Pat Regenberg, librarian at Overlook Medical Center, Summit, NJ, for her help in gathering literature; Katie Glisic, National Prion Disease Pathology Surveillance Center, Cleveland, OH, for her content input; and Ermias Belay, MD, associate director for epidemiologic science, Division of High-Consequence Pathogens and Pathology, National Center for Emerging and Zoonotic Infectious Diseases, Centers for Disease Control and Prevention, Atlanta, GA, for publishing the most current prion guidelines and allowing their distribution. Editor’s note: Lyodura is a registered trademark of B. Braun Melsungen AG, Melsungen, Germany. References 1. CJD (Creutzfeldt-Jakob Disease, Classic). Centers for Disease Control and Prevention. http://www.cdc.gov/ ncidod/dvrd/cjd/index.htm. Accessed May 12, 2014. 2. D’amour R, Guimond P. An experiential learning model applied to nurses working with patients with CreutzfeldtJakob disease. Can J Neurosci Nurs. 2010;32(2):34-39. 3. Collins SJ, Athan E, Koehler AP. Updated CreutzfeldtJakob disease infection control guidelines: sifting facts from fiction. Med J Aust. 2013;199(8):535-536. 4. The Nobel Prize in Physiology or Medicine 1997. Nobel Prize.org. http://www.nobelprize.org/nobel_prizes/ medicine/laureates/1997. Accessed May 12, 2014. 5. Sharma S, Mukherjee M, Kedage V, Muttigi MS, Rao A, Rao S. Sporadic Creutzfeldt-Jakob diseaseda review. Int J Neurosci. 2009;119(11):1981-1994. 6. Prusiner SB. Prions. Proc Natl Acad Sci U S A. 1998; 95(23):13363-13383. 7. Porter MC, Leemans M. Creutzfeldt-Jakob disease. Cont Educ Anaesth Crit Care Pain. 2013;13(4):119-124. http://ceaccp.oxfordjournals.org/content/early/2013/02/ 24/bjaceaccp.mkt002.full. Accessed May 12, 2014. 8. Prion diseases. Centers for Disease Control and Prevention. http://www.cdc.gov/ncidod/dvrd/prions/index.htm. Accessed May 12, 2014. 9. Head MW, Ironside JW. Review: Creutzfeldt-Jakob disease: prion protein type, disease phenotype and agent strain. Neuropathol Appl Neurobiol. 2012;38(4):296-310. 10. Puoti G, Bizzi A, Forloni G, Safar JG, Tagliavini F, Gambetti P. Sporadic human prion diseases: molecular insights and diagnosis. Lancet Neurol. 2012;11(7): 618-628. 11. Ladogana A, Puopolo M, Croes EA, et al. Mortality from Creutzfeldt-Jakob disease and related disorders in Europe, Australia, and Canada. Neurology. 2005;64(9): 1586-1591. www.aornjournal.org 12. Blossom DB, Maddox RA, Beavers SF, et al. A case of Creutzfeldt-Jakob disease associated with a dura mater graft in the United States. Infect Control Hosp Epidemiol. 2007;28(12):1396-1397. 13. Stride P, Hunter J, Bailey M. Nursing patients with Creutzfeldt-Jakob disease. Are you at risk? Aust Nurs J. 2009;17(1):30-32. 14. Kozubski W, Wender M, Szczech J, Lenart-Jankowska D, Liberski PP. Atypical case of sporadic Creutzfeldt-Jakob disease (CJD) in a young adult. Folia Neuropathol. 1998; 36(4):225-228. 15. Johnson RT, Gonzalez RG, Frosch MP. Case records of the Massachusetts General Hospital. Case 27-2005. An 80-year-old man with fatigue, unsteady gait, and confusion. N Engl J Med. 2005;353(10):1042-1050. 16. Imran M, Mahmood S. An overview of human prion diseases. Virol J. 2011;24(8):559. 17. Nozaki I, Hamaguchi T, Sanjo N, et al. Prospective 10year surveillance of human prion diseases in Japan. Brain. 2010;133(10):3043-3057. 18. Kovacs GG, Majtenyi K. Creutzfeldt-Jakob disease in Hungary. Folia Neuropathol. 2005;43(4):279-285. 19. Brown P, Galvez S, Goldfarb LG, et al. Familial Creutzfeldt-Jakob disease in Chile is associated with the codon 200 mutation of the PRNP amyloid precursor gene on chromosome 20. J Neurol Sci. 1992;112(1-2):65-67. 20. How should surgical instruments used on suspected or confirmed CJD patients be reprocessed? Centers for Disease Control and Prevention. http://www.cdc.gov/ncidod/ dvrd/cjd/qa_cjd_infection_control.htm#reprocessed. Accessed June 12, 2014. 21. Questions and answers: Creutzfeldt-Jakob disease infection-control practices. Centers for Disease Control and Prevention. http://www.cdc.gov/ncidod/dvrd/cjd/qa_ cjd_infection_control.htm. Accessed May 12, 2014. 22. Fuoco MA. Creutzfeldt-Jakob death prompts letters to UPMC neurosurgery patients. post-gazette.com. June 13, 2002. http://old.post-gazette.com/healthscience/20020613 disease0613p2.asp. Accessed May 12, 2014. 23. Emory Hospital suspects case of rare CJD: notifying surgical patients [news release]. Atlanta, GA: Woodruff Health Sciences Center, Emory University; October 1, 2004. http://whsc.emory.edu/press_releases2.cfm?announce ment_id_seq¼1760. Accessed June 30, 2014. 24. Craver R. Lawsuits common after discovery of brain disease mishap. Winston-Salem Journal. http://www .journalnow.com/business/business_news/local/lawsuits -common-after-discovery-of-brain-disease-mishap/article _5fd7a51f-8236-5fe0-9a93-3e341408a96c.htm. Published February 16, 2014. Accessed May 12, 2014. 25. Hamaguchi T, Noguchi-Shinohara M, Nozaki I, et al. Medical procedures and risk for sporadic CreutzfeldtJakob disease, Japan, 1999e2008. Emerg Infect Dis. 2009;15(2):265-271. 26. de Pedro-Cuesta J, Mahillo-Fernandez I, Rabano A, et al; EUROSURGYCJD Research Group. Nosocomial transmission of sporadic Creutzfeldt-Jakob disease: results from a risk-based assessment of surgical interventions. J Neurol Neurosurg Psychiatry. 2011;82(2):204-212. 27. Brown P, Brandel JP, Sato T, et al. Iatrogenic Creutzfeldt-Jakob disease, final assessment. Emerg Infect Dis. 2012;18(6):901-907. AORN Journal j 405 October 2014 Vol 100 No 4 28. Gupta A, Hirsch N. Prion diseases. Anaesth Int Care Med. 2013;14(9):407-409. 29. Draft quantitative risk assessment of vCJD risk potentially associated with the transfusion of red blood cells in the U.S. US Food and Drug Administration-Center for Biologics Evaluation and Research. http://www.fda.gov/ downloads/AdvisoryCommittees/CommitteesMeeting Materials/BloodVaccinesandOtherBiologics/Transmissible SpongiformEncephalopathiesAdvisoryCommittee/UCM 343264.pdf. Published March 4, 2013. Accessed June 13, 2014. 30. vCJD differs from classic CJD. Centers for Disease Control and Prevention. http://www.cdc.gov/ncidod/ dvrd/vcjd/factsheet_nvcjd.htm#cjdvsnvcjd. Accessed June 13, 2014. 31. vCJD (variant Creutzfeldt-Jakob disease). Centers for Disease Control and Prevention. http://www.cdc.gov/ ncidod/dvrd/vcjd/index.htm. Accessed May 12, 2014. 32. Biela C. New fears surrounding the spread of variant Creutzfeldt-Jakob disease. J Renal Nurs. 2014;6(1):45. 33. vCJD (variant Creutzfeldt-Jakob disease). Confirmed variant Cretzfeldt-Jakob disease (variant CJD) case in Texas. Centers for Disease Control and Prevention. http:// www.cdc.gov/ncidod/dvrd/vcjd/other/confirmed-case-in -texas.htm. Published June 2, 2014. Accessed June 27, 2014. 34. Young S. 4,000 pounds of rib-eyes, other beef recalled; mad cow disease a concern. CNN Health. http://www .cnn.com/2014/06/12/health/beef-recall-mad-cow-disease. Published June 13, 2014. Accessed June 27, 2014. 35. Edgeworth JA, Farmer M, Sicilia A, et al. Detection of prion infection in variant Creutzfeldt-Jakob disease: a blood-based assay. Lancet. 2011;377(9764):487-493. 36. Is Creutzfeldt-Jakob disease contagious? University of California Memory and Aging Center. http://memory .ucsf.edu/cjd/overview/contagion. Accessed June 27, 2014. 37. Creutzfeldt-Jakob disease fact sheet. National Institute of Neurological Disorders and Stroke. http://www.ninds .nih.gov/disorders/cjd/detail_cjd.htm. Accessed May 12, 2014. 38. Roohani P, Saha MK, Rosenbloom M. Creutzfeldt-Jakob disease in the hospital setting: a case report and review. Minn Med. 2013;96(5):46-49. 39. Zerr I, Kallenberg K, Summers DM, et al. Updated clinical diagnostic criteria for sporadic Creutzfeldt-Jakob disease. Brain. 2009;132(Pt 10):2659-2668. 40. Haı̈k S, Marcon G, Mallet A, et al. Doxycycline in Creutzfeldt-Jakob disease: a phase 2, randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2014;13(2):150-158. 41. Skrlj N, Dolinar M. New engineered antibodies against prions. Bioengineered. 2014;5(1):10-15. 42. Rutala WA, Weber DJ; Society for Healthcare Epidemiology of America. Guideline for disinfection and sterilization of prion-contaminated medical instruments. Infect Control Hosp Epidemiol. 2010;31(2):107-117. 43. WHO Infection Control Guidelines for Transmissible Spongiform Encephalopathies. Geneva, Switzerland: World Health Organization; 1999. http://www.who.int/ csr/resources/publications/bse/whocdscsraph2003.pdf? ua¼1. Accessed June 30, 2014. 406 j AORN Journal KARASIN 44. Belay ED, Blase J, Sehulster LM, Maddox RA, Schonberger LB. Management of neurosurgical instruments and patients exposed to Creutzfeldt-Jakob disease. Infect Control Hosp Epidemiol. 2013;34(12):1272-1280. 45. WHO Guidelines on Tissue Infectivity Distribution in Transmissible Spongiform Encephalopathies. Geneva, Switzerland: World Health Organization; 2006. http:// www.who.int/bloodproducts/TSEPUBLISHEDREPORT .pdf. Accessed June 30, 2014. 46. WHO Manual for Surveillance of Human Transmissible Spongiform Encephalopathies Including Variant CreutzfeldtJakob Disease. Geneva, Switzerland: World Health Organization; 2003. http://whqlibdoc.who.int/publications/2003/ 9241545887.pdf. Accessed June 30, 2014. 47. Alcalde-Cabero E, Almazan-Isla J, Brandel JP, et al. Health professions and risk of sporadic Creutzfeldt-Jakob disease, 1965 to 2010. Euro Surveill. 2012;17(15):1-10. http://www.eurosurveillance.org/ViewArticle.aspx?Article Id¼20144. Accessed May 12, 2014. 48. Addendum to Sentinel Event Alert #20: Exposure to Creutzfeldt-Jakob Disease, September 18, 2013. The Joint Commission. http://www.jointcommission.org/assets/ 1/18/SEA_20_CJD_Addendum091813.pdf. Accessed May 12, 2014. 49. Secker TJ, Herve R, Zhao Q, Borisenko KB, Abel EW, Keevil CW. Doped diamond-like carbon coatings for surgical instruments reduce protein and prion-amyloid biofouling and improve subsequent cleaning. Biofouling. 2012;28(6):563-569. 50. Lipscomb IP, Pinchin H, Collin R, Keevil CW. Effect of drying time, ambient temperature and pre-soaks on prioninfected tissue contamination levels on surgical stainless steel: concerns over prolonged transportation of instruments from theatre to central sterile service departments. J Hosp Infect. 2007;65(1):72-77. 51. Advisory Committee on Dangerous Pathogens: transmissible spongiform encephalopathy. GOV.UK. https:// www.gov.uk/government/groups/advisory-committee -on-dangerous-pathogens. Accessed May 12, 2014. 52. Yan ZX, Stitz L, Heeg P, Pfaff E, Roth K. Infectivity of prion protein bound to stainless steel wires: a model for testing decontamination procedures for transmissible spongiform encephalopathies. Infect Control Hosp Epidemiol. 2004;25(4):280-283. 53. Rogez-Kreuz C, Yousfi R, Soufflet C, et al. Inactivation of animal and human prions by hydrogen peroxide gas plasma sterilization. Infect Control Hosp Epidemiol. 2009;30(8):769-777. 54. Edgeworth JA, Sicilia A, Linehan J, Brandner S, Jackson GS, Collinge J. A standardized comparison of commercially available prion decontamination reagents using the Standard Steel-Binding Assay. J Gen Virol. 2011;92(Pt 3):718-726. 55. Tomkinson A, De Martin S, Gilchrist CR, Temple M. Instrumentation and patient characteristics that influence postoperative hemorrhage rates following tonsil and adenoid surgery. Clin Otolaryngol. 2005;30(4):338-346. 56. Nix P. Prions and disposable surgical instruments. Int J Clin Pract. 2003;57(8):678-680. 57. Rentz C. Nursing care of the person with sporadic Creutzfeldt-Jakob Disease. J Hosp Palliat Nurs. 2008; 10(5):272-282. SPECIAL NEEDS POPULATIONS: CJD 58. Morris C. Counselling people with Creutzfeldt-Jakob disease (CJD) and their families. Dementia. 2010;9(4):569-576. 59. Brendle TA. Reducing the risk of cross-contamination from transmissible spongiform encephalopathies. AORN J. 2005;82(3):442-446. 60. In CB, Choi YS, Park EY, et al. Anesthetic management in patients suspected of Creutzfeldt-Jakob diseaseda case report. Korean J Anesthesiol. 2011;61(3):262-264. 61. ASA Committee on Occupational Health Task Force on Infection Control. Recommendations for Infection Control for the Practice of Anesthesiology. 3rd ed. Schaumburg, IL: American Society of Anesthesiologists; 2011. https://www.asahq.org/coveo.aspx?q¼Recommendations %20for%20Infection%20Control%20for%20the%20 Practice%20of%20Anesthesiology. Accessed June 30, 2014. 62. Farling P, Smith G. Anaesthesia for patients with Creutzfeldt-Jakob disease. A practical guide. Anaesthesia. 2003;58(7):627-629. 63. Transmissible spongiform encephalopathy agents: safe working and the prevention of infection: annex F. GOV. UK. https://www.gov.uk/government/uploads/system/ uploads/attachment_data/file/270734/Annex_F_Endoscopy .pdf. Updated January 2014. Accessed May 12, 2014. 64. Wilson AJ, Nayak S. Disinfection, sterilization and disposables. Anaesth Int Care Med. 2013;14(10):423-427. http://www.anaesthesiajournal.co.uk/article/S1472-0299 (13)00196-3/abstract. Accessed May 12, 2014. 65. Higgins DJ, Kinnear JA. Percutaneous tracheostomy and Creutzfeldt-Jakob disease. Anaesthesia. 2004;59(7): 722-723. 66. The Joint Commission. Sentinel Event Alert: exposure to Creutzfeldt-Jakob disease. http://www.jointcommission .org/assets/1/18/SEA_20.pdf. Published June 1, 2001. Accessed May 12, 2014. www.aornjournal.org 67. Saskatoon Health Region. Infection Prevention & Control Committee. Creutzfeldt Jacob Disease. Policies & Procedures number 40e40, CJD. https://www.saskatoon healthregion.ca/about/IPCPolicies/40-40.pdf. Published June 2003. Accessed May 12, 2014. 68. Transmissible spongiform encephalopathy agents: safe working and the prevention of infection: part 4: infection prevention and control of CJD, vCJD and other human prion diseases in healthcare and community settings. United Kingdom Department of Health. https://www.gov .uk/government/uploads/system/uploads/attachment_data /file/270732/Part_4_Infection_control_of_CJD__vCJD_ and_other_human_prion_diseases_in_healthcare_and_ community_settings.pdf. Published June 2003. Updated January 2014. Accessed May 12, 2014. 69. McNeil B. Management of a CJD case. Part 1. Preoperative organisation of the case. Br J Perioper Nurs. 2004; 14(4):164-167, 169-170. 70. McNeil B. Management of a CJD case. Part 2. The patient with CJD in the operating theatre. Br J Perioper Nurs. 2004;14(5):223-226. Mark Karasin, BSN, BA, RN, is an RN at Overlook Medical Center, Summit, NJ, and a DNP student at Rutgers, The State University of New Jersey, Piscataway Township. Mr Karasin has no declared affiliation that could be perceived as posing a potential conflict of interest in the publication of this article. AORN Journal j 407 EXAMINATION CONTINUING EDUCATION Special Needs Populations: Perioperative Care of the Patient With Creutzfeldt-Jakob Disease 2.6 www.aorn.org/CE PURPOSE/GOAL To provide the learner with knowledge specific to caring for the surgical patient who has or is suspected of having Creutzfeldt-Jakob disease (CJD). OBJECTIVES 1. 2. 3. 4. 5. Describe prions as they relate to CJD. Discuss the etiology of the types of CJD. Discuss the symptoms of CJD. Compare the different methods for diagnosing CJD. Describe perioperative considerations for a patient who has or is suspected of having CJD. The Examination and Learner Evaluation are printed here for your convenience. To receive continuing education credit, you must complete the online Examination and Learner Evaluation at http://www.aorn.org/CE. QUESTIONS 1. 2. Prions stand out from typical infectious agents such as bacteria or viruses because they a. have no nucleic acid and cannot reproduce. b. are only present in brain tissue. c. cannot be acquired by consuming contaminated foods. d. can affect all life forms, including invertebrates and fish. The majority of CJD cases are _______, but its cause remains unknown. a. familial b. iatrogenic c. sporadic d. new variant 408 j AORN Journal October 2014 Vol 100 No 4 3. Transmission of CJD via medical interventions is classified as a. familial. b. iatrogenic. c. sporadic. d. new variant. 4. The cardinal sign of CJD is a. blindness. b. deterioration of muscle coordination. c. personality changes. d. rapidly progressive dementia. 5. A diagnosis of CJD may be determined by 1. color Doppler ultrasound. 2. magnetic resonance imaging. Ó AORN, Inc, 2014 CE EXAMINATION 3. the presence of 14-3-3 protein in the patient’s cerebrospinal fluid. 4. the presence of specific peaks on electroencephalography readings. 5. tissue biopsy or autopsy. a. 4 and 5 b. 1, 2, and 3 c. 2, 3, 4, and 5 d. 1, 2, 3, 4, and 5 6. The incubation period for CJD can be as long as 50 years before symptoms appear. a. true b. false 7. According to the World Health Organization, ______________ have to be maintained when providing routine nursing care to a patient with suspected or confirmed CJD. a. airborne precautions b. contact precautions c. reverse precautions d. only standard precautions www.aornjournal.org 8. Certain materials used to make surgical instruments (eg, nickel) may significantly decrease the level of protein absorption and residue. a. true b. false 9. The CJD prions are susceptible only to conventional methods of disinfection and sterilization. a. true b. false 10. To lessen the time required to perform proper postoperative cleaning, OR personnel should 1. allow only essential items in the room. 2. allow only one of each instrument to be placed in the instrument tray. 3. cover all pedals and cords with a plastic bag and secure them in place. 4. cover equipment, the walls, the bed, and the floor of the working area with sheets of polyvinyl chloride. a. 1 and 3 b. 2 and 4 c. 1, 3, and 4 d. 1, 2, 3, and 4 AORN Journal j 409 LEARNER EVALUATION CONTINUING EDUCATION PROGRAM Special Needs Populations: Perioperative Care of the Patient With Creutzfeldt-Jakob Disease T his evaluation is used to determine the extent to which this continuing education program met your learning needs. The evaluation is printed here for your convenience. To receive continuing education credit, you must complete the online Examination and Learner Evaluation at http://www .aorn.org/CE. Rate the items as described below. OBJECTIVES To what extent were the following objectives of this continuing education program achieved? 1. Describe prions as they relate to Creutzfeldt-Jakob disease (CJD). Low 1. 2. 3. 4. 5. High 2. Discuss the etiology of the types of CJD. Low 1. 2. 3. 4. 5. High 3. Discuss the symptoms of CJD. Low 1. 2. 3. 4. 5. High 4. Compare the different methods for diagnosing CJD. Low 1. 2. 3. 4. 5. High 5. Describe perioperative considerations for a patient who has or is suspected of having CJD. Low 1. 2. 3. 4. 5. High CONTENT 6. To what extent did this article increase your knowledge of the subject matter? Low 1. 2. 3. 4. 5. High 7. To what extent were your individual objectives met? Low 1. 2. 3. 4. 5. High 410 j AORN Journal October 2014 Vol 100 No 4 2.6 www.aorn.org/CE 8. Will you be able to use the information from this article in your work setting? 1. Yes 2. No 9. Will you change your practice as a result of reading this article? (If yes, answer question #9A. If no, answer question #9B.) 9A. How will you change your practice? (Select all that apply) 1. I will provide education to my team regarding why change is needed. 2. I will work with management to change/ implement a policy and procedure. 3. I will plan an informational meeting with physicians to seek their input and acceptance of the need for change. 4. I will implement change and evaluate the effect of the change at regular intervals until the change is incorporated as best practice. 5. Other: ________________________________ 9B. If you will not change your practice as a result of reading this article, why? (Select all that apply) 1. The content of the article is not relevant to my practice. 2. I do not have enough time to teach others about the purpose of the needed change. 3. I do not have management support to make a change. 4. Other: ________________________________ 10. Our accrediting body requires that we verify the time you needed to complete the 2.6 continuing education contact hour (156-minute) program: _______________________________ Ó AORN, Inc, 2014