Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
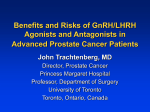
VOLUME 25 䡠 NUMBER 3 䡠 JANUARY 20 2007 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Adjuvant Chemotherapy Followed By Goserelin Compared With Either Modality Alone: The Impact on Amenorrhea, Hot Flashes, and Quality of Life in Premenopausal Patients—The International Breast Cancer Study Group Trial VIII From the International Breast Cancer Study Group (IBCSG); IBCSG Coordinating Center, Swiss Group for Clinical Cancer Research (SAKK), Department of Medical Oncology, Bern; Bürgerspital and Kantonsspital, St Gallen; Oncology Institute of Southern Switzerland, Bellinzona, Switzerland; IBCSG Statistical Center, Dana-Farber Cancer Institute, Frontier Science and Technology Research Foundation, Harvard School of Public Health, Boston, MA; Australian New Zealand Breast Cancer Trials Group and Newcastle Mater Misericordiae Hospital, Newcastle; Department of Surgery, The Royal Melbourne Hospital, Melbourne; the University of Sydney, Sydney, Australia; Groote Schuur Hospital and University of Cape Town, South Africa; and the European Institute of Oncology, Milan, Italy. Submitted October 8, 2005; accepted October 17, 2006; published online ahead of print at www.jco.org on December 11, 2006. Supported by Swiss Group for Clinical Cancer Research (SAKK), Frontier Science and Technology Research Foundation, The Cancer Council Australia, Australian New Zealand Breast Cancer Trials Group, Australian National Health and Medical Research Council (project 920876), National Cancer Institute Grant No. CA-75362; Bethesda, MD, Swedish Cancer Society, Cancer Association of South Africa, and Foundation for Clinical Research of Eastern Switzerland (OSKK). Astra-Zeneca provided the Zoladex free of charge. Authors’ disclosures of potential conflicts of interest and author contributions are found at the end of this article. Address reprint requests to Jürg Bernhard, PhD, International Breast Cancer Study Group Coordinating Center, Effingerstr 40, 3008 Bern, Switzerland; e-mail: juerg.bernhard@ ibcsg.org. © 2007 by American Society of Clinical Oncology 0732-183X/07/2503-263/$20.00 DOI: 10.1200/JCO.2005.04.5393 Jürg Bernhard, David Zahrieh, Monica Castiglione-Gertsch, Christoph Hürny, Richard D. Gelber, John F. Forbes, Elizabeth Murray, John Collins, Stefan Aebi, Beat Thürlimann, Karen N. Price, Aron Goldhirsch, and Alan S. Coates A B S T R A C T Purpose The purpose of this article is to compare quality of life (QOL) and menopausal symptoms among premenopausal patients with lymph node-negative breast cancer receiving chemotherapy, goserelin, or their sequential combination, and to investigate differential effects by age. Patients and Methods We evaluated QOL data from 874 pre- and perimenopausal women with lymph node-negative breast cancer who were randomly assigned to receive six courses of classical cyclophosphamide, methotrexate, and fluorouracil (CMF) chemotherapy, ovarian suppression with goserelin for 24 months, or six courses of classical CMF followed by 18 months of goserelin. We report QOL data collected during 3 years after random assignment in patients without disease recurrence. Results Overall, patients receiving goserelin alone showed a marked improvement or less deterioration in QOL measures over the first 6 months than those patients treated with CMF. There were no differences at 3 years after random assignment according to treatment except for hot flashes. As reflected in the hot flashes scores, patients in all three treatment groups experienced induced amenorrhea, but the onset of ovarian function suppression was slightly delayed for patients receiving chemotherapy. Younger patients (⬍ 40 years) who received goserelin alone returned to their premenopausal status at 6 months after the cessation of therapy, while those who received CMF showed marginal changes from their baseline hot flashes scores. Conclusion Age-adjusted risk profiles that consider patient-reported outcomes enable patients to adapt to their disease and treatment, such as considering the trade-offs between delayed endocrine symptoms, but higher risk of permanent menopause with chemotherapy, and immediate but reversible endocrine symptoms with goserelin, in younger premenopausal patients. J Clin Oncol 25:263-270. © 2007 by American Society of Clinical Oncology INTRODUCTION The International Breast Cancer Study Group (IBCSG) trial VIII for pre- and perimenopausal women with lymph node-negative breast cancer compared sequential chemotherapy followed by the gonadotropin-releasing hormone agonist goserelin with either modality alone. Disease-related outcomes have been reported.1 Patients with estrogen receptor (ER) -negative tumors achieved better disease-free survival (DFS) if they received treatments that included cyclophosphamide, methotrex- ate, and fluorouracil (CMF) than if they received goserelin alone. In contrast, for patients with ER– positive disease, chemotherapy alone and goserelin alone provided similar outcomes, whereas sequential therapy provided a statistically nonsignificant benefit compared with either modality alone, due largely to the results for the younger patients. In this report, we compare the impact of the randomized treatments on quality of life (QOL). Similar adjuvant trials have been reported.2,3 The trade-offs between early (first 6 months), intermediate (months 6 to 24), and late (month 36) QOL effects require 263 Information downloaded from www.jco.org and provided by DANA FARBER CANCER INST on January 19, 2007 from 155.52.45.137. Copyright © 2007 by the American Society of Clinical Oncology. All rights reserved. Bernhard et al patients and physicians to balance different impacts of treatment at different time points, making individual decision making more challenging.4 However, minor differences in the toxicity profiles may be important for a patient’s choice.3,4 Age may influence a patient’s perception of fertility, body image, and sexuality. Younger women are especially vulnerable for physical and emotional sequelae of breast cancer, with an early menopause as a main concern.5-10 We expanded the QOL analysis by investigating the time course of amenorrhea and patient-rated hot flashes, a key symptom of estrogen deprivation, between treatments and by patient age. PATIENTS AND METHODS Trial From March 1990 through October 1999, 1,111 pre- and perimenopausal patients were randomly assigned to receive either no adjuvant systemic treatment, six 28-day courses of classical CMF chemotherapy (in which one course, every 28 days, consisted of cyclophosphamide at 100 mg/m2 on days 1 through 14, orally; methotrexate at 40 mg/m2 on days 1 and 8, intravenously; and fluorouracil at 600 mg/m2 on days 1 and 8, intravenously), 24 monthly subcutaneous implants of a gonadotropin-releasing hormone analog (goserelin at 3.6 mg every 28 days), or six 28-day courses of classical CMF followed by 18 implants of goserelin. Systemic adjuvant therapy was to begin within 6 weeks of primary surgery. For the sequential treatment arm, the first goserelin implant was scheduled to be given on day 28 of the sixth course of CMF. Informed consent was required according to the criteria established within the individual countries. The protocol was approved by institutional review boards as required by national and local law. The details of the trial protocol and conduct are described elsewhere.1 In April 1992, after accrual of 205 patients, random assignment to the noadjuvant treatment control arm (46 patients) was discontinued because of results from other trials. This report concerns QOL comparisons among the three active treatment arms. For the first 36 months of treatment, patients received a calendar to record their menses. These data were checked by the medical staff at visits and transmitted to the menstrual status form with 1 ⫽ normal; 2 ⫽ scanty; 3 ⫽ no menses. QOL Analysis The IBCSG QOL core questionnaire11-13 comprised single-item linear analog self-assessment (LASA) indicators for physical well-being, mood,14 coping effort,15 appetite, tiredness, hot flashes, nausea/vomiting, perceived social support, restrictions in arm movement, and subjective health estimation16 referring to the last 2 weeks. Patient self-assessments were obtained at the beginning of treatment (baseline), at month 3 (ie, day 1 of cycle 3 or 8 weeks after goserelin start), and at each 3 months for the first 2 years, and again at year 3. We report QOL data for the first 36 months in patients without recurrence within this time. The protocol required that all patients participate in the QOL study. As a primary hypothesis, based on experience in patients with node-positive disease11 we predicted worse QOL during chemotherapy (months 3 and 6) as compared with goserelin but no residual effects in treatment groups after completion of chemotherapy, using coping effort as primary end point. As a secondary hypothesis, we expected a smaller adverse effect of CMF on mood at baseline for patients with ER-negative tumors than for those with ER-positive tumors.17 We considered a change of 8 points or more on a scale of 0 to 100 as clinically significant.18 Of the 1,065 patients randomly assigned to one of the three adjuvanttreatment arms, 1,043 were deemed eligible and assessable. Of these, 874 patients were included in the QOL analysis (Table 1). We expected the QOL assessment at month 36 from all patients randomly assigned at a time point less than 3 years before June 1, 1995, resulting in a total of 746 (85%) of the 874 patients for this assessment. To identify reasons for the lower submission rate at month 36, we investigated the association between missing data and baseline 264 Table 1. Description of Patients Excluded From the QOL Analysis of Trial VIII No. of Patients Patient Group Goserelin CMF CMF Followed by Goserelin Total eligible and assessable patients Exclusions from QOL analysis Relapsed or died within first 3 years Completed no QOL assessments Completed assessments in multiple languages Undefined culture Included in the QOL analyses 341 350 352 1,043 45 46 28 119 9 10 16 35 4 4 6 14 0 283 0 290 1 301 1 874 Total Abbreviations: QOL, quality of life; CMF, cyclophosphamide, methotrexate, and fluorouracil. characteristics, treatment assignment, participating center, and toxicity, and fit a logistic regression model to examine the relative importance of these factors. For a sensitivity analysis, two imputation techniques were used. Missing values at month 36 were replaced by the previous assessment score, and the lower quartile from the compliant cases at month 36 was applied to the noncompliant cases. The indicators were scored between 0 and 100 and analyzed separately; higher values represented better QOL or less severe symptoms/adverse effects. QOL scores were transformed to reduce skewing. The statistical significance of treatment differences at each time point was assessed with analysis of variance, adjusting for country/language group.11 The figures show the results in the original scores from 0 to 100. We also tested for differences in QOL scores between baseline and month 3 of the within patient changes in an analysis of variance model that included assigned treatment and country/language group. Similarly, we analyzed changes from baseline to month 6 and month 36. Differential treatment effects by age were analyzed post hoc using the hot flashes indicator with the anchors of none and a lot, with age categorized as 39 years or younger and 40 years or older. Treatment-covariate interactions were studied by use of the nonparametric Subpopulation Treatment Effect Pattern Plot (STEPP) methodology.19,20 STEPP involves defining overlapping subgroups of patients on the basis of a covariate of interest and studying the resulting pattern of the treatment effects estimated within each subgroup. Patient age at study entry was the covariate of interest. The treatment effects estimated within each subgroup were calculated as mean of the square root of the hot flashes scores, then transformed back for visual display. Probability values are two sided. P ⱕ .05 was deemed statistically significant. No adjustment was made for multiple testing. RESULTS The submission rates of the QOL forms were similar across treatment groups and decreased as follow-up went on, from 90% at baseline, to 77% at month 12, to 74% at month 24, and to 62% at month 36. Participants and nonparticipants at month 36 were similar regarding age, tumor size, tumor grade, and ER status at random assignment. The toxicity profile of participants and nonparticipants at month 36 within the goserelin (submission rate, 65%) and CMF (60%) arms was similar. Participating center was most strongly associated with missing data at month 36 (P ⫽ .02; data not shown). Table 2 presents characteristics of the 874 patients. Nineteen percent of the patients were age 39 years or younger. The median JOURNAL OF CLINICAL ONCOLOGY Information downloaded from www.jco.org and provided by DANA FARBER CANCER INST on January 19, 2007 from 155.52.45.137. Copyright © 2007 by the American Society of Clinical Oncology. All rights reserved. Amenorrhea and Quality of Life Table 2. Baseline Characteristics According to Treatment of the Patients Included in the QOL Analyses (N ⫽ 874) Patients Goserelin CMF Followed by Goserelin CMF Total Characteristic No. % No. % No. % No. % Total ER status Negative Positive Unknown Primary treatment Total mastectomy Breast conservation With RT With no RT Tumor size, cm ⱕ 1.0 1.1-2.0 ⱖ 2.1 Unknown Tumor grade 1 2 3 Unknown Age, years ⱕ 39 ⱖ 40 283 32 290 33 301 34 874 100 83 189 11 29 67 4 85 198 7 29 68 2 88 206 7 29 68 2 256 593 25 29 68 3 118 42 128 44 123 41 369 42 155 10 55 4 150 12 52 4 160 18 53 6 465 40 53 5 28 148 105 2 10 52 37 1 31 143 112 4 11 49 39 1 47 155 97 2 16 52 32 1 106 446 314 8 12 51 36 1 49 131 102 1 17 46 36 1 39 137 108 6 13 47 37 2 73 126 100 2 24 42 33 1 161 394 310 9 18 45 35 1 53 230 19 82 48 242 17 83 64 237 21 78 165 709 19 81 Abbreviations: QOL, quality of life; CMF, cyclophosphamide, methotrexate, and fluorouracil; ER, estrogen receptor; RT, radiation therapy. age within this cohort was 36 years (range, 22 to 39). The median age within the cohort of patients age 40 or older was 46 years (range, 40 to 58). Sixty-eight percent of patients had primary tumors classified as ER–positive, 29% of patients had primary tumors classified ER–negative, and 3% of patients had primary tumors classified ER– unknown. During the first 3, 6, and 36 months, we compared the change (mean, SE) in QOL scores from baseline between patients receiving Table 3. Changes in QOL Scores From Baseline to Months 3, 6, and 36 in Patients Receiving Goserelin Alone Versus CMF Change From Baseline to Month 3ⴱ Goserelin Alone CMF QOL Indicator Mean ⫾ SE Mean ⫾ SE Physical well-being Mood Coping effort Appetite Tiredness Hot flashes Nausea/vomiting Perceived social support Restrictions in arm movement Subjective health estimation ⫺1.4 ⫾ 3.5 ⫺3.0 ⫾ 3.5 5.2 ⫾ 3.4 ⫺1.2 ⫾ 3.3 ⫺8.2 ⫾ 4.0 ⫺43.8 ⫾ 4.5 ⫺6.6 ⫾ 4.2 0.6 ⫾ 2.4 ⫺1.6 ⫾ 3.3 1.5 ⫾ 3.2 1.4 ⫾ 3.2 ⫺4.2 ⫾ 3.1 ⫺12.2 ⫾ 3.5 ⫺12.7 ⫾ 4.0 ⫺22.5 ⫾ 3.8 0.8 ⫾ 2.1 8.7 ⫾ 3.7 13.4 ⫾ 3.3 ⫺0.6 ⫾ 3.5 ⫺4.1 ⫾ 3.1 Change From Baseline to Month 6ⴱ Goserelin Alone CMF P Mean ⫾ SE Mean ⫾ SE .90 .04 .08 .14 .15 ⬍ .0001 ⬍ .0001 .93 ⫺1.7 ⫾ 3.7 1.0 ⫾ 3.8 10.7 ⫾ 3.9 0.9 ⫾ 3.4 ⫺8.0 ⫾ 4.2 ⫺35.0 ⫾ 5.3 ⫺1.2 ⫾ 4.2 ⫺1.8 ⫾ 2.7 ⫺4.7 ⫾ 3.4 2.2 ⫾ 3.5 2.8 ⫾ 3.6 ⫺2.7 ⫾ 3.1 ⫺13.1 ⫾ 3.7 ⫺31.2 ⫾ 4.7 ⫺18.0 ⫾ 3.7 0.5 ⫾ 2.4 .06 11.2 ⫾ 4.0 .17 0.8 ⫾ 3.3 Change From Baseline to Month 36ⴱ Goserelin Alone CMF P Mean ⫾ SE Mean ⫾ SE P .20 .60 .001 .10 .08 .30 ⬍ .0001 .22 4.9 ⫾ 3.6 9.5 ⫾ 4.3 15.0 ⫾ 4.4 4.7 ⫾ 3.5 ⫺0.7 ⫾ 4.4 ⫺5.0 ⫾ 5.1 3.5 ⫾ 3.14 ⫺2.9 ⫾ 3.1 8.8 ⫾ 3.2 14.8 ⫾ 3.8 18.7 ⫾ 3.9 6.6 ⫾ 3.1 1.8 ⫾ 3.9 ⫺23.7 ⫾ 4.5 7.0 ⫾ 2.7 ⫺1.0 ⫾ 2.7 .12 .08 .24 .46 .42 ⬍ .0001 .11 .39 9.5 ⫾ 3.6 .54 13.1 ⫾ 4.6 13.1 ⫾ 4.0 0.99 ⫺4.2 ⫾ 3.0 .03 9.5 ⫾ 3.4 10.1 ⫾ 3.0 0.80 Abbreviations: QOL, quality of life; CMF, cyclophosphamide, methotrexate, and fluorouracil. ⴱ Mean changes in QOL scores between baseline and months 3, 6, and 36 were obtained from an ANOVA model that included assigned treatment and country/language group. Negative values indicate a worsening condition for all indicators. 265 www.jco.org Information downloaded from www.jco.org and provided by DANA FARBER CANCER INST on January 19, 2007 from 155.52.45.137. Copyright © 2007 by the American Society of Clinical Oncology. All rights reserved. Bernhard et al Median Hot Flashes Score Better Worse 100 90 80 70 60 50 40 Goserelin CMF CMF goserelin 30 20 0 3 6 9 12 15 18 21 24 27 30 33 36 QOL Assessments (months) No. of patients 570 518 511 494 489 446 464 465 471 P .86 <.01 .03 <.01 .04 .01 .25 .85 <.01 437 <.01 Fig 1. Median hot flashes scores by treatment group during the first 36 months for the 874 patients assessable for quality of life (QOL). The points indicate the assessments when the patients were undergoing chemotherapy. Higher values indicate fewer hot flashes. CMF, cyclophosphamide, methotrexate, and fluorouracil. 266 Better 100 90 Median Coping Score goserelin alone with patients receiving CMF (Table 3). Significant benefits were found for goserelin, with less impairment by nausea/ vomiting and an improvement in coping and subject health estimation. For the first 3 months, patients receiving goserelin reported a bigger increase in hot flashes and a worse mood. There were no differences at 36 months according to treatment in any of the indicators, except for hot flashes (Fig 1). The coping scores indicated a rapid, clinically significant improvement after completing chemotherapy (Fig 2). At baseline, patients receiving CMF reported more coping effort, although this difference was not statistically significant (P ⫽ .12). Of the patients who submitted a baseline QOL form, 43% completed the form before random assignment (45% goserelin; 42% CMF); thus up to 57% did so after knowing treatment assignment. When we excluded those patients who filled out their baseline assessment after random assignment, the results were similar but slightly more pronounced on average for each indicator. At month 36, the results of both imputation techniques were consistent with our main findings (data not shown). We tested for QOL differences among treatment groups at each time point separately for both the ER–negative and ER–positive cohorts. Results were similar within both cohorts (data not shown). Patients in all three treatment arms experienced induced amenorrhea, but the onset was delayed slightly for those patients who received chemotherapy relative to those patients who received initial goserelin—a pattern also reflected in the hot flashes scores (Fig 1). After cessation of goserelin treatment, patients who received goserelin alone indicated fewer hot flashes than those patients who had received CMF (P ⬍ .01 at months 24 and 36). The percentage of patients who reported no menses during each month after random assignment according to treatment group is shown separately for younger (age ⱕ 39; Fig 3A) and older patients (age ⱖ 40; Fig 3B). For younger patients, goserelin induced amenorrhea within 2 months of study entry for 90% of the patients and within 80 70 60 50 40 Goserelin CMF CMF goserelin 30 Worse 20 0 3 6 9 12 15 18 21 24 27 30 33 36 QOL Assessments (months) No. of patients 774 705 687 676 674 627 649 647 641 P .14 <.01 <.01 .44 .80 .93 .77 .38 .89 460 .57 Fig 2. Median scores of coping effort (Perceived Adjustment to Chronic Illness Scale [PACIS]) by treatment group during the first 36 months for the 874 patients assessable for quality of life (QOL). The points indicate the assessments when the patients were undergoing chemotherapy. Higher values indicate less effort to cope. CMF, cyclophosphamide, methotrexate, and fluorouracil. 3 months for virtually all patients. Amenorrhea continued until the end of goserelin treatment, when menses resumed in all but a few patients. In contrast, chemotherapy-induced amenorrhea was achieved more slowly and was observed in approximately 50% of patients by the end of six courses of CMF. Among patients in whom goserelin was not given after CMF, menses resumed in approximately 15%, but amenorrhea continued in approximately 35% to 40% of such patients throughout the 36-month period of observation. Among patients who received goserelin after CMF, virtually all reported amenorrhea during the 18-month goserelin treatment period. Resumption of menses after cessation of goserelin was slower in patients who had received initial CMF than in those who did not. The pattern of incidence of amenorrhea over time was different for patients age ⱖ 40 (Fig 3B). Chemotherapy-induced amenorrhea was observed sooner and in a larger proportion of patients than was observed in the younger cohort. More than 90% of these patients who received six courses of CMF reported amenorrhea by the end of chemotherapy. Although menses resumed in a few patients who did not receive goserelin after chemotherapy, nearly all cases had amenorrhea during the entire 36-month follow-up period, regardless of whether goserelin was used. We analyzed the hot flashes scores according to the same age groups (Figs 4A and 4B). The same pattern seen for all patients across time was observed within the cohort of older patients. However, within the cohort of younger patients, patients on all three arms eventually returned to their initial status after completing treatment by CMF and/or goserelin, respectively. The patterns of changes were similar: goserelin was associated with greater early deterioration, which later recovered, whereas the effect of CMF, though slower in onset, was persistent, especially among older patients (data not shown). We performed a STEPP analysis at months 3, 6, and 36 for the hot flashes indicator to evaluate the differences in treatment effects according to age (Fig 5), limited to the 323 patients with complete JOURNAL OF CLINICAL ONCOLOGY Information downloaded from www.jco.org and provided by DANA FARBER CANCER INST on January 19, 2007 from 155.52.45.137. Copyright © 2007 by the American Society of Clinical Oncology. All rights reserved. Amenorrhea and Quality of Life Goserelin CMF CMF goserelin 0 10 Patients With Amenorrhea (%) 10 Patients With Amenorrhea (%) B Goserelin CMF CMF goserelin 0 20 30 40 50 60 70 80 90 20 30 Fig 3. Percentage of randomly assigned patients (n ⫽ 1,063) in the International Breast Cancer Study Group trial VIII with amenorrhea during each month from random assignment according to treatment. (A) Shows the results for patients age 39 years or younger, and (B) shows the results for patients age 40 years or older. CMF, cyclophosphamide, methotrexate, and fluorouracil. 40 50 60 70 80 90 100 100 0 6 12 18 24 30 36 0 Months From Random Assignment 6 12 18 24 30 36 Months From Random Assignment data for hot flashes at months 3, 6, and 36. For this sliding window analysis, each subpopulation contained approximately 70 patients, and each subsequent subpopulation was formed moving from left to right by dropping approximately 45 patients with the lowest age and adding approximately 45 patients with the next higher age. At month 3 (Fig 5A), significantly more hot flashes were observed at all ages for patients randomly assigned to goserelin alone compared with CMF (P ⬍ .01) and CMF followed by goserelin (P ⬍ .01). Patients in older cohorts who were assigned CMF and CMF followed by goserelin reported hot flashes scores similar to those for goserelin alone. By month 6 (Fig 5B), the youngest cohort receiving CMF reported fewer hot flashes than for patients assigned to goserelin alone, however, as age increased there was no clear pattern of treatment differences as all patients reported similar hot flashes scores. By month 36 (Fig 5C), when all patients were no longer receiving treatment, the youngest A patients returned to the low or absent hot flashes scores reported at baseline. This return to initial status was most striking in the goserelin alone group. As the median age increased, fewer patients randomly assigned to goserelin alone experienced hot flashes compared with those randomly assigned to CMF (P ⫽ .03) or to CMF followed by goserelin (P ⫽ .03). DISCUSSION We compared the impact of the goserelin, CMF, and CMF followed by goserelin on various QOL indicators measured during 3 years after beginning of adjuvant therapy according to age, specifically examining patient-rated hot flashes, a very common complaint of peri- and postmenopausal women.21 The patterns of amenorrhea B Median Hot Flashes Score Better 100 Better 90 80 70 60 50 40 Goserelin CMF CMF goserelin 30 Worse 20 Median Hot Flashes Score A 3 6 9 12 15 18 21 24 27 30 33 36 QOL Assessments (months) No. of patients 107 100 99 102 99 89 93 85 P .94 <.01 .07 <.01 <.01 <.01 <.01 .04 100 .01 90 80 70 60 50 40 Goserelin CMF CMF goserelin 30 Worse 0 100 20 0 3 6 9 12 15 18 21 24 27 30 33 36 QOL Assessments (months) 81 .04 No. of patients 463 418 412 392 390 357 371 380 371 P .77 <.01 .11 .05 .28 .07 .77 .49 <.01 356 <.01 Fig 4. Median hot flashes scores by treatment group during the first 36 months. (A) Shows the results for the 165 patients age ⱕ 39 years, and (B) shows the results for the 709 patients age ⱖ 40 years. The points indicate the assessments when the patients were undergoing chemotherapy. Higher values indicate fewer hot flashes. CMF, cyclophosphamide, methotrexate, and fluorouracil. 267 www.jco.org Information downloaded from www.jco.org and provided by DANA FARBER CANCER INST on January 19, 2007 from 155.52.45.137. Copyright © 2007 by the American Society of Clinical Oncology. All rights reserved. Bernhard et al Better 100 Median Hot Flashes Score A Worse 80 60 40 20 Goserelin CMF CMF goserelin 0 37 42 44 46 48 50 52 70 53 Median Age (years) No. of patients 70 70 70 70 Better 100 Median Hot Flashes Score B 70 Worse 80 60 40 20 Goserelin CMF CMF goserelin 0 37 42 44 46 48 50 52 70 53 Median Age (years) No. of patients 70 70 70 70 Better 100 Median Hot Flashes Score C 70 Worse 80 60 40 20 Goserelin CMF CMF goserelin 0 37 42 44 46 48 50 52 70 53 Median Age (years) No. of patients 70 70 70 70 70 Fig 5. Subpopulation Treatment Effect Pattern Plots (STEPP) showing the median hot flashes scores in the original scale according to treatment and age subgroup (A) 3 months, (B) 6 months, and (C) 36 months after random assignment. Higher values indicate fewer hot flashes. CMF, cyclophosphamide, methotrexate, and fluorouracil. 268 and patient-reported hot flashes were strikingly similar over time. This correspondence supports the clinical validity of patientreported data by this type of simple single-item indicator. Baseline assessment was required before adjuvant treatment but allowed before or after random assignment. A substantial proportion of patients, similar between those with versus without chemotherapy, completed the QOL form after random assignment. To eliminate any differential anticipatory effects on baseline scores in future studies, we have since introduced a completed QOL form as an eligibility criterion. Firm conclusions at month 36 are hampered by incomplete participation of patients. Those who did participate, however, were representative of each treatment arm, and baseline characteristics were balanced according to participants and nonparticipants. Participating center, a stratification factor at random assignment, was the most important predictor of forms submission at 36 months. Because we recognize that missing data cannot be ignored in QOL studies, the IBCSG has introduced a missing QOL form to collect reasons for missing data. Overall, patients treated with goserelin alone showed a more pronounced improvement or less decline in various QOL indicators during the first 6 months than those with CMF. A similar early benefit in favor of goserelin was shown in the Zoladex Early Breast Cancer Research Association (ZEBRA) and the Zoladex in Premenopausal Patients (ZIPP) trials.2,3 In the ZEBRA trial, the same indicator for coping was used and showed the same pattern: patients with goserelin alone required less effort to cope reflecting less burden by adverse effects. In agreement with both trials, in our trial there was no difference in mood and in physical domains at 3 years. Peri- or postmenopausal status per se is not an independent predictor of lower QOL.22 The improvement of these QOL domains over time, in particular coping, confirms the pattern of adaptation described in our previous trials,11,23,24 pointing to the major importance of a patient’s psychological adaptation for her QOL. Patients can be supported in their adaptation by psycho-oncologic interventions. This is particularly relevant to the age group of our trial, given that younger women are more vulnerable for physical and emotional sequelae of a breast cancer diagnosis. Contrary to our hypothesis, patients’ QOL under chemotherapy was not affected by the ER-status of their tumor. Both CMF and goserelin induce amenorrhea. However, while it is reversible in the majority of patients after cessation of goserelin, it is often permanent after CMF. Patients in whom treatment results in permanent amenorrhea have the short and long-term effects of an early menopause. In the ZEBRA and the ZIPP trials, the hormonal symptoms were worse in the goserelin group during the 2-year goserelin treatment period compared with the CMF group. One year after the cessation of goserelin therapy, this trend was reversed. The same pattern was seen for patient-rated hot flashes. Patients randomly assigned to receive goserelin alone returned to baseline values at 3 years, while patients who received CMF underwent early menopause. However, there were substantial age-related differences among patients who received CMF. Younger patients (ⱕ 39 years) reported little change in hot flashes, while older patients (ⱖ 40 years) showed a delayed onset of considerable hot flashes and remained at this level. This differential effect by age was further illustrated by the STEPP analysis, which showed consistent patterns. This finding of differential symptom effects according to age underlines the importance of individual decision making. JOURNAL OF CLINICAL ONCOLOGY Information downloaded from www.jco.org and provided by DANA FARBER CANCER INST on January 19, 2007 from 155.52.45.137. Copyright © 2007 by the American Society of Clinical Oncology. All rights reserved. Amenorrhea and Quality of Life For patients with ER-positive disease, CMF alone and goserelin alone provided similar DFS outcomes.1 Hence, QOL considerations become even more relevant to treatment choice. They have to be balanced from patient’s individual perspective. In the younger patients, this includes trade-offs between the early and a lower risk of immediate symptoms but higher risk of permanent menopause by chemotherapy, and initially greater but reversible endocrine symptoms with 2 years of goserelin. In the ZIPP trial, the effects on sexuality of CMF were comparable with those of goserelin.25 After age 40, when fertility becomes less important for many women, the perspective of going once (chemotherapy) or twice (goserelin) through menopause is an additional issue to consider. Sequential therapy provided a statistically nonsignificant trend to benefit in DFS compared with either modality alone, due largely to the results among younger patients.1 CMF followed by goserelin showed the same effect on all QOL indicators as CMF alone. The effects of chemotherapy appear to mask those of endocrine therapy. This finding confirms those of the ZIPP trial, where no difference was found regarding physical symptoms or sexual dysfunction between corresponding groups.3,25 Endocrine therapy had differential effects on symptoms only in patients not treated with CMF. Those receiving tamoxifen indicated milder menopausal symptoms than those with goserelin, with the exception of vaginal discharge. Vasomotor symptoms and vaginal dryness were most troublesome. Differences in endocrine adverse effect profiles may assist in supportive care needs but do not necessarily impact overall QOL.26,27 REFERENCES 1. International Breast Cancer Study Group: Adjuvant chemotherapy followed by goserelin versus either modality alone for premenopausal lymph node-negative breast cancer: A randomized trial. J Natl Cancer Inst 95:1833-1846, 2003 2. de Haes H, Olschewski M, Kaufmann M, et al: Quality of life in goserelin-treated versus cyclophosphamide ⫹ methotrexate ⫹ fluorouracil-treated premenopausal and perimenopausal patients with node-positive, early breast cancer: The Zoladex Early Breast Cancer Res Association Trialists Group. J Clin Oncol 21:4510-4516, 2003 3. Nystedt M, Berglund G, Bolund C, et al: Side effects of adjuvant endocrine treatment in premenopausal breast cancer patients: A prospective randomized study. J Clin Oncol 21:1836-1844, 2003 4. Goodwin PJ: Reversible ovarian ablation or chemotherapy: Are we ready for quality of life to guide adjuvant treatment decisions in breast cancer? J Clin Oncol 21:4474-4475, 2003 5. Wenzel LB, Fairclough DL, Brady MJ, et al: Age-related differences in the quality of life of breast carcinoma patients after treatment. Cancer 86:17681774, 1999 6. Ganz PA, Rowland JH, Desmond K, et al: Life after breast cancer: Understanding women’s healthrelated quality of life and sexual functioning. J Clin Oncol 16:501-514, 1998 7. Broeckel JA, Jacobsen PB, Balducci L, et al: Quality of life after adjuvant chemotherapy for breast cancer. Breast Cancer Res Treat 62:141-150, 2000 8. King MT, Kenny P, Shiell A, et al: Quality of life three months and one year after first treatment for early stage breast cancer: Influence of treatment and patient characteristics. Qual Life Res 9:789-800, 2000 Thus, our trial shows patterns of QOL effects caused by adjuvant chemotherapy, goserelin, or their sequential combination similar with those described in previous trials in premenopausal patients. However, patternsofsymptomsdifferedsubstantiallybyage.Theriskofmenopause inducedbychemotherapywaslowinyoungerpatientsandincreasedwith age. Age-adjusted adverse effect risk profiles offer an opportunity to support patients’ in their adaptation to disease and treatment. AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST The authors indicated no potential conflicts of interest. AUTHOR CONTRIBUTIONS Conception and design: Jürg Bernhard, Christoph Hürny, Richard D. Gelber, Alan S. Coates Provision of study materials or patients: Elizabeth Murray, John Collins, Stefan Aebi Data analysis and interpretation: David Zahrieh, Richard D. Gelber Manuscript writing: Jürg Bernhard, David Zahrieh, Monica Castiglione-Gertsch, Christoph Hürny, Richard D. Gelber, John F. Forbes, Elizabeth Murray, John Collins, Stefan Aebi, Beat Thürlimann, Karen N. Price, Aron Goldhirsch, Alan S. Coates Final approval of manuscript: Jürg Bernhard, David Zahrieh, Monica Castiglione-Gertsch, Christoph Hürny, Richard D. Gelber, John F. Forbes, Elizabeth Murray, John Collins, Stefan Aebi, Beat Thürlimann, Karen N. Price, Aron Goldhirsch, Alan S. Coates 9. Ganz PA, Desmond KA, Beth L, et al: Quality of life in long-term, disease-free survivors of breast cancer: A follow-up study. J Natl Cancer Inst 94:3949, 2002 10. Ganz PA, Greendale GA, Petersen L, et al: Breast cancer in younger women: Reproductive and late health effects of treatment. J Clin Oncol 21: 4184-4193, 2003 11. Hürny C, Bernhard J, Coates AS, et al: Impact of adjuvant therapy on quality of life in women with node positive operable breast cancer: International Breast Cancer Study Group. Lancet 347:1279-1284, 1996 12. Bernhard J, Hürny C, Coates AS, et al: Quality of life assessment in patients receiving adjuvant therapy for breast cancer: The IBCSG approach: The International Breast Cancer Study Group. Ann Oncol 8:825-835, 1997 13. Bernhard J, Sullivan M, Huerny C, et al: Clinical relevance of single item quality of life indicators in cancer clinical trials. Br J Cancer 84:1156-1165, 2001 14. Hürny C, Bernhard J, Coates A, et al: Responsiveness of a single-item indicator versus a multiitem scale: Assessment of emotional well-being in an international adjuvant breast cancer trial. Med Care 34:234-248, 1996 15. Hürny C, Bernhard J, Bacchi M, et al: The Perceived Adjustment to Chronic Illness Scale (PACIS): A global indicator of coping for operable breast cancer patients in clinical trials: Swiss Group for Clinical Cancer Res (SAKK) and the International Breast Cancer Study Group (IBCSG). Support Care Cancer 1:200-208, 1993 16. Hurny C, van Wegberg B, Bacchi M, et al: Subjective health estimations (SHE) in patients with advanced breast cancer: An adapted utility concept for clinical trials. Br J Cancer 77:985-991, 1998 17. Bernhard J, Hurny C, Coates AS, et al: Factors affecting baseline quality of life in two international adjuvant breast cancer trials: International Breast Cancer Study Group (IBCSG). Br J Cancer 78:686693, 1998 18. Sloan JA, Dueck A: Issues for statisticians in conducting analyses and translating results for quality of life end points in clinical trials. J Biopharm Stat 14:73-96, 2004 19. Bonetti M, Gelber RD: A graphical method to assess treatment-covariate interactions using the Cox model on subsets of the data. Stat Med 19: 2595-2609, 2000 20. Bonetti M, Gelber RD: Patterns of treatment effects in subsets of patients in clinical trials. Biostatistics 5:465-481, 2004 21. Stearns V, Ullmer L, Lopez JF, et al: Hot flushes. Lancet 360:1851-1861, 2002 22. Avis NE, Assmann SF, Kravitz HM, et al: Quality of life in diverse groups of midlife women: Assessing the influence of menopause, health status and psychosocial and demographic factors. Qual Life Res 13:933-946, 2004 23. Bernhard J, Zahrieh D, Coates AS, et al: Quantifying trade-offs: Quality of life and qualityadjusted survival in a randomised trial of chemotherapy in postmenopausal patients with lymph node-negative breast cancer. Br J Cancer 91: 1893-1901, 2004 24. International Breast Cancer Study Group: Randomized controlled trial of ovarian function suppression plus tamoxifen versus the same endocrine therapy plus chemotherapy: Is chemotherapy necessary for premenopausal women with node-positive, endocrine responsive breast cancer? First results of International Breast Cancer Study Group Trial 11-93. Breast 10:130-138, 2001 (suppl 3) 269 www.jco.org Information downloaded from www.jco.org and provided by DANA FARBER CANCER INST on January 19, 2007 from 155.52.45.137. Copyright © 2007 by the American Society of Clinical Oncology. All rights reserved. Bernhard et al 25. Berglund G, Nystedt M, Bolund C, et al: Effect of endocrine treatment on sexuality in premenopausal breast cancer patients: A prospective randomized study. J Clin Oncol 19:2788-2796, 2001 26. Fallowfield L, Cella D, Cuzick J, et al: Quality of life of postmenopausal women in the Arimidex, Tamoxifen, Alone or in Combination (ATAC) Adjuvant Breast Cancer Trial. J Clin Oncol 22:4261-4271, 2004 27. Hunter MS, Grunfeld EA, Mittal S, et al: Menopausal symptoms in women with breast cancer: Prevalence and treatment preferences. Psychooncology 13:769-778, 2004 ■ ■ ■ Acknowledgment We thank the patients, physicians, nurses, and data managers who participate in the International Breast Cancer Study Group trials and Rita Hinkle for data management. Appendix The Appendix is included in the full-text version of this article, available online at www.jco.org. It is not included in the PDF version (via Adobe® Reader®). 270 JOURNAL OF CLINICAL ONCOLOGY Information downloaded from www.jco.org and provided by DANA FARBER CANCER INST on January 19, 2007 from 155.52.45.137. Copyright © 2007 by the American Society of Clinical Oncology. All rights reserved.