Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
ADVANCED CLINICAL BRAIN IMAGING AT 3 T
SNR and Parallel Imaging Improvements
Offered by a 32 Channel Head Coil Design
Val M. Runge • Scott and White Clinic and Hospital
Bodie J. Correll • Texas A&M University Health Science Center
Ervin L. Lowther • Texas A&M University Health Science Center
Frederik L. Giesel • German Cancer Research Center (DKFZ)
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
ABSTRACT
BACKGROUND INFORMATION - Advanced head coil design with
3 T imaging substantially improves the available signal-to-noise ratio
(SNR), making possible a significant reduction in scan time, the use of
advanced parallel imaging, high spatial resolution imaging (reduced voxel
size in 3D acquisitions, whether for imaging of the brain itself or the
vasculature) and implementation of innovative imaging techniques. The
use of higher parallel imaging factors in conventional diffusion-weighted
echoplanar imaging (EPI), together with the implementation of a fast spin
echo (FSE) based BLADE diffusion-weighted scan is illustrated in
patients with acute infarction (the latter free of bulk susceptibility artifact
and geometric image distortion).
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
ABSTRACT continued
With T1-weighted imaging, the 32 channel coil design permits a factor of
two reduction in scan time for 2D imaging, and enables the use of a T1weighted turboFLASH BLADE technique for motion robust imaging and
alternatively an ultra-high resolution 3D T1-weighted FLASH scan for
more cooperative patients.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
OBJECTIVE
The main objective of this exhibit is to demonstrate the potential for
improved clinical brain imaging at 3 T, afforded by the available increased
SNR due to the use of a FDA approved, commercially available, 32
channel coil, focusing on:
(1) decreased scan time,
(2) utilization of new advanced imaging sequences, and
(3) increased spatial resolution.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
ORGANIZATION
Applications employing the improved SNR and parallel imaging
capability are illustrated in patient exams at 3 T using:
> FSE BLADE DWI
> 2D T1-weighted FLASH
> T1-weighted turboFLASH BLADE
> FLAIR and T2-weighted BLADE
> SPACE
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
TEACHING POINTS
> To illustrate the potential of new advanced imaging sequences,
utilizing the SNR and parallel imaging capability of the 32 channel
coil, including a T1-weighted BLADE turboFLASH technique for
reduced motion artifacts and a diffusion weighted BLADE FSE
sequence for reduction of bulk susceptibility artifacts
> To review the use of BLADE (PROPELLER) in combination with
the 32 channel coil, illustrating the decrease in scan time that can be
achieved (to 2:06 min:sec for 4 mm sections with FLAIR BLADE and
0:56 with T2 BLADE), and the resultant image quality
Acknowledgment: The BLADE pulse sequences and associated image reconstruction software were developed by
Alto Stemmer from Siemens Medical Solutions.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
INTRODUCTION
Utilizing multiple institutional review board (IRB) approved protocols,
a 32-channel head coil (32-element design with 32 integrated
preamplifiers, now FDA approved) was evaluated on a Tim Trio 3 T MR
system (Siemens Medical Solutions) in 46 normal volunteers (60 separate
MR sessions) and 30 patients. In regard to the latter, the diagnostic exam
required by the IRB for clinical purposes was first acquired using the
standard 12-channel head coil (Head Matrix Coil - 12-element design
with 12 integrated preamplifiers, one ring of 12 elements each), and then
imaging was performed with the 32-channel head coil. The performance
of the 32-channel coil in contrast enhanced MRA using TWIST in
combination with low dose gadolinium chelate injection was also
evaluated.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FSE BLADE DWI
Twenty-two normal volunteers and five patients, the latter with acute to
early subacute ischemic infarcts, were studied with diffusion weighted
imaging (DWI), employing both the 12- and 32-channel head coils.
Diffusion-weighted echoplanar images were acquired in both the axial
(n=12) and coronal (n=10) planes, comparing scans without parallel
imaging to those with parallel imaging factors (IPAT) of 2 and 4. These
results were compared to scans acquired using a fast spin echo (FSE)
BLADE diffusion weighted technique (Figure 1). Higher IPAT factors
were evaluated due to an interest in further reducing bulk susceptibility
artifacts (Figure 2). These are prominent in echoplanar DWI at interfaces
between air-filled sinuses and the brain, and are substantially greater at
3 T as opposed to 1.5 T.
Click Figure Callout to View Figure
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FSE BLADE DWI continued
The FSE BLADE DWI approach was evaluated, although intrinsically
of lower signal-to-noise ratio (SNR) than echoplanar DWI, due to the
interest in providing images with little if any degradation due to bulk
susceptibility artifact. BLADE (PROPELLER) represents an innovative
imaging approach, in which k-space is sampled by multiple echo trains in
a rotating, partially overlapping, fashion (like the rotation of a propeller),
rather than in the standard rectilinear fashion. Each scan was performed
twice to enable the determination of SNR measurements, since parallel
imaging was employed. Region of interest measurements were performed
in two different anatomical areas (cerebral white matter and peripheral
cerebellum). In normal volunteers, the 32-channel head coil demonstrated
an improvement in SNR in both anatomic regions as compared to the
12-channel coil. With echoplanar based DWI (and no IPAT), the
improvement in the SNR was 43% for cerebral white matter and 67%
for peripheral cerebellum.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FSE BLADE DWI continued
Increasing the IPAT factor lead to a decrease in SNR in both the 32- and
12-channel coils. SNR remained however increased in each region of
interest with the 32- vs. 12-channel coil with the implementation of
parallel imaging. The use of an IPAT factor of 4, permitted by the 32channel coil, substantially reduced bulk susceptibility artifact from airbrain interfaces, and was demonstrated in axial, coronal, and sagittal
imaging (Figure 3). Diffusion weighted imaging was possible with the
BLADE FSE sequence in a reasonable scan time (3:48 min:sec) by use
of the 32-channel coil (Figure 4). Three scan trace diffusion weighted
imaging (BLADE FSE), using a 192 x 192 matrix, was performed in
patients in all three orthogonal planes, with equivalent depiction of acute
to early subacute infarcts to echoplanar based DWI, but with elimination
of bulk susceptibility artifacts.
Click Figure Callout to View Figure
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
2D T1-weighted FLASH
A comparison of T1-weighted imaging using the 12- and 32-channel coils
was performed in 10 normal volunteers and 6 patients. T1-weighted axial
and sagittal 2D short TE gradient echo (GRE) images were acquired using
both the 12- and 32-channel coils. Two acquisitions (averages) were
employed for the 12-channel coil scans, and one acquisition for the 32channel coil scans (Figure 5). Scan times were 2:10 and 1:52 min:sec for
the sagittal and axial scans using the 12-channel coil, and 1:12 and 0:56
min:sec for the 32-channel coil. This work was performed specifically to
evaluate the capability of the 32-channel coil using approximately half
scan time.
Click Figure Callout to View Figure
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
T1-weighted turboFLASH BLADE
Additional T1-weighted axial 2D BLADE turboFLASH (0.9 x 0.9 x 4
mm3 voxel dimension, scan time = 2:45 min:sec) scans were acquired
using the 32-channel coil only. Despite the almost 2-fold reduction in
scan time used with the 32-channel coil, on short TE GRE T1-weighted
imaging, there was a 26% increase in SNR in cerebral white matter and
a 10% increase in the cerebellum. Acquisition of the 2D BLADE
turboFLASH scan using the 32-channel coil led to very reproducible,
motion insensitive T1-weighted scans of high image quality with
improved gray-white matter contrast when compared to the short TE GRE
sequence (Figure 6).
Click Figure Callout to View Figure
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
TWIST (Time-resolved Angiography With Interleaved Stochastic Trajectories)
TWIST was evaluated for its performance in visualization of the arterial
and venous vasculature, in 22 exams (in an experimental animal model),
using a scan with voxel dimensions of 1.2 x 1 x 1 mm3, IPAT=3, and
acquisition time of 1.95 sec ("3-D multiphasic low dose contrast enhanced
MR angiography using TWIST on a 32-channel head coil at 3 Tesla:
Comparison of a conventional gadolinium chelate with a high relaxivity
agent", European Congress of Radiology 2008, Giesel F et al). Excellent
visualization in particular of the arterial system was demonstrated, despite
use of almost 1/3rd the normal contrast dose (0.04 mmol/kg, MultiHance).
With the recognition of nephrogenic systemic fibrosis, gadolinium chelate
administration in patients with renal failure has become a major concern,
and in particular accumulated dosage. The 32-channel coil should allow
low dose contrast enhanced MR angiography with high temporal and
spatial resolution of both the arterial and venous systems of the brain.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FLAIR and T2-weighted BLADE; SPACE
Patient studies included, in addition to the results previously discussed
(such as application in T1-weighted imaging, figures 5, 6), acquisition
of half scan time sequences (with the 32-channel coil) using FLAIR and
T2-weighted BLADE (Figure 7). Image quality was equivalent to scans
with twice the acquisition time using the 12-channel coil in the cerebral
hemispheres, with slightly degraded image quality in the posterior fossa.
Additional scan sequences evaluated in patients included 3D MP-RAGE,
FLAIR SPACE, T2-weighted SPACE, and double inversion recovery. The
32-channel coil was employed in these 3D scan acquisitions to provide
higher voxel resolution within a reasonable scan time (Figure 8).
After review of Figure 7& 8 this concludes the main exhibit. You may click
here to jump to the Conclusion and Author Correspondence Information slides.
or click elsewhere to review Figures 1-8 once more prior to the Conclusion.
Click Figure Callout to View Figure
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 1
Diffusion weighted scans are illustrated in a normal volunteer, all acquired with
the 32-channel head coil at 3 T. The first three images are with echoplanar
diffusion weighted imaging, comparing (A) the use of no parallel imaging, to
implementation of parallel imaging factors (IPAT) of (B) 2 and (C) 4. Bulk
susceptibility artifacts become less evident as IPAT is increased. The pons is
relatively poorly depicted with an IPAT of 4, due to lower SNR. (D) illustrates the
equivalent BLADE fast spin echo (FSE) diffusion weighted
A
B
scan, with no bulk susceptibility artifacts evident. The high
SNR of the 32-channel coil makes acquisition of this scan
possible within a reasonable time (3:48 min:sec). All scans
C
D
were acquired with a b value of 1000.
Click on thumbnails
for a larger view.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 2
The same four scan types are illustrated as in Figure 1, in a different
normal volunteer, with acquisition in the sagittal (A-D) and coronal (E-H)
planes (A & E no IPAT, B & F IPAT 2, C & G IPAT 4).
A
B
The capability of the 32-channel coil to perform well
(in all planes) with high IPAT values (=4, in C & G)
is noted, together with the advantage of (D & H) the
C
D
BLADE FSE diffusion weighted scan (made possible
by the SNR of the 32-channel coil) for elimination of
bulk susceptibility artifacts. All scans were acquired
F
E
with a 192 matrix.
G
Click on thumbnails
for a larger view.
H
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 3
A patient with multiple punctate acute infarcts is illustrated in (A) with
echoplanar diffusion weighted imaging using the 12-channel coil and an
IPAT factor of 2. The capability of the 32-channel coil for higher IPAT
factors, and thus less bulk susceptibility artifact, in all planes is illustrated
in (B-D) with IPAT 4 scans in the axial, sagittal, and coronal planes.
Click on thumbnails
for a larger view.
A
B
C
D
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 4
Diffusion weighted scans in a patient with an acute thalamic infarct are
compared. (A) was acquired with the 12-channel coil and an IPAT of 2.
(B-D) were acquired with the 32-channel coil. (B) and (C) are echoplanar
technique, with an IPAT of 4, while (D) is the BLADE FSE diffusion
weighted scan. Note the reduction in susceptibility artifact with IPAT 4 in
(B) as compared to (A), and the viability of IPAT
A
B
4 scans in both the axial and coronal planes
with the 32-channel coil. Note also the elimination
of bulk susceptibility artifact (seen in B, arrow,
in this instance originating from the frontal sinus)
C
D
using the BLADE FSE diffusion weighted
approach.
Click on thumbnails
for a larger view.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 5
A scan acquired with the 12-channel coil using a short TE 2D T1weighted FLASH scan with 2 averages and an acquisition time of 1:52 is
compared with scans acquired with the 32-channel coil using the same
FLASH scan but with 1 average and an acquisition time of 0:56, together
with a 2D BLADE turboFLASH scan with acquisition time of 2:45. All
scans are in a normal volunteer.
Click on thumbnails for a larger view.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 6
Two scans are illustrated, both acquired with the 32-channel coil, in a
patient with enhancing (active) multiple sclerosis plaques. The first scan is
a short TE T1-weighted 2D FLASH, with voxel dimensions of 0.9 x 0.9 x
4 mm3, which is substantially degraded (by image blurring) due to patient
motion despite the very short scan time (0:56 min:sec) made possible by
use of the 32-channel coil. The second scan is a T1-weighted 2D
turboFLASH BLADE, with equivalent voxel dimension, acquired in 2:45
min:sec. Note the marked improvement in image quality on the BLADE
scan, with elimination of the blurring
noted in the first scan due to patient
motion.
Click on thumbnails
for a larger view.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 7
Scans are illustrated in a patient with brain metastases. (A, B) Short TE 2D
T1-weighted FLASH scans are presented, comparing a scan acquired (A) with
the 12-channel coil in a 1:52 min:sec scan time to that acquired (B) with the
32-channel coil in a 0:56 min:sec scan time. Image quality is equivalent for
depiction of the large enhancing parenchymal brain metastasis, as well as two
smaller metastases. (C, D) FLAIR and T2-weighted BLADE 2D axial scans
are also illustrated, both acquired with the 32-channel coil. An IPAT factor of
2 was used for both scans, with these scans typically performed when using
the 12-channel coil without IPAT, leading to almost
A
B
a 2 fold reduction in scan time. In this instance, the
scan times were 1:03*2 and 0:28*2 min:sec, with
both scans providing whole brain coverage using a
C
D
4 mm slice thickness.
Click on thumbnails
for a larger view.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 8
A .9 x .9 x .9 mm3 voxel size, 2:12 min:sec acquisition time, T2-weighted
SPACE scan is illustrated, acquired with the 32-channel coil. An
arteriovenous malformation is noted in the posterior fossa, illustrated with
high image quality on reformatted images in the sagittal, coronal, and
axial planes.
Click on thumbnails for a larger view.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
CONCLUSION
Overall the 32-channel coil represents a major
advance when compared to all previous FDA
approved 3 T head coil designs due both to improved
SNR and its parallel imaging capabilities. Additional
important applications, not discussed, include MR
spectroscopy and fMRI.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
Author Correspondence Information:
Val M. Runge, MD
Editor-in-Chief, Investigative Radiology
Robert and Alma Moreton Centennial Chair in Radiology
Scott and White Clinic and Hospital
Texas A&M University Health Science Center
Department of Radiology
2401 South 31st St.
Temple, TX 76508
(254) 724-2415
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 1
Diffusion weighted scans are illustrated in a normal volunteer, all acquired with
the 32-channel head coil at 3 T. The first three images are with echoplanar
diffusion weighted imaging, comparing (A) the use of no parallel imaging, to
implementation of parallel imaging factors (IPAT) of (B) 2 and (C) 4. Bulk
susceptibility artifacts become less evident as IPAT is increased. The pons is
relatively poorly depicted with an IPAT of 4, due to lower SNR. (D) illustrates the
equivalent BLADE fast spin echo (FSE) diffusion weighted
A
B
scan, with no bulk susceptibility artifacts evident. The high
SNR of the 32-channel coil makes acquisition of this scan
possible within a reasonable time (3:48 min:sec). All scans
C
D
were acquired with a b value of 1000.
CLICK TO RETURN TO PRESENTATION
Click on thumbnails
for a larger view.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 2
The same four scan types are illustrated as in Figure 1, in a different
normal volunteer, with acquisition in the sagittal (A-D) and coronal (E-H)
planes (A & E no IPAT, B & F IPAT 2, C & G IPAT 4).
A
B
The capability of the 32-channel coil to perform well
(in all planes) with high IPAT values (=4, in C & G)
is noted, together with the advantage of (D & H) the
C
D
BLADE FSE diffusion weighted scan (made possible
by the SNR of the 32-channel coil) for elimination of
bulk susceptibility artifacts. All scans were acquired
F
E
with a 192 matrix.
G
CLICK TO RETURN TO PRESENTATION
Click on thumbnails
for a larger view.
H
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 3
A patient with multiple punctate acute infarcts is illustrated in (A) with
echoplanar diffusion weighted imaging using the 12-channel coil and an
IPAT factor of 2. The capability of the 32-channel coil for higher IPAT
factors, and thus less bulk susceptibility artifact, in all planes is illustrated
in (B-D) with IPAT 4 scans in the axial, sagittal, and coronal planes.
CLICK TO RETURN TO PRESENTATION
Click on thumbnails
for a larger view.
A
B
C
D
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 4
Diffusion weighted scans in a patient with an acute thalamic infarct are
compared. (A) was acquired with the 12-channel coil and an IPAT of 2.
(B-D) were acquired with the 32-channel coil. (B) and (C) are echoplanar
technique, with an IPAT of 4, while (D) is the BLADE FSE diffusion
weighted scan. Note the reduction in susceptibility artifact with IPAT 4 in
(B) as compared to (A), and the viability of IPAT
A
B
4 scans in both the axial and coronal planes
with the 32-channel coil. Note also the elimination
of bulk susceptibility artifact (seen in B, arrow,
in this instance originating from the frontal sinus)
C
D
using the BLADE FSE diffusion weighted
approach.
CLICK TO RETURN TO PRESENTATION
Click on thumbnails
for a larger view.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 5
A scan acquired with the 12-channel coil using a short TE 2D T1weighted FLASH scan with 2 averages and an acquisition time of 1:52 is
compared with scans acquired with the 32-channel coil using the same
FLASH scan but with 1 average and an acquisition time of 0:56, together
with a 2D BLADE turboFLASH scan with acquisition time of 2:45. All
scans are in a normal volunteer.
Click on thumbnails for a larger view.
CLICK TO RETURN TO PRESENTATION
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 6
Two scans are illustrated, both acquired with the 32-channel coil, in a
patient with enhancing (active) multiple sclerosis plaques. The first scan is
a short TE T1-weighted 2D FLASH, with voxel dimensions of 0.9 x 0.9 x
4 mm3, which is substantially degraded (by image blurring) due to patient
motion despite the very short scan time (0:56 min:sec) made possible by
use of the 32-channel coil. The second scan is a T1-weighted 2D
turboFLASH BLADE, with equivalent voxel dimension, acquired in 2:45
min:sec. Note the marked improvement in image quality on the BLADE
scan, with elimination of the blurring
noted in the first scan due to patient
motion.
CLICK TO RETURN TO PRESENTATION
Click on thumbnails
for a larger view.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 7
Scans are illustrated in a patient with brain metastases. (A, B) Short TE 2D
T1-weighted FLASH scans are presented, comparing a scan acquired (A) with
the 12-channel coil in a 1:52 min:sec scan time to that acquired (B) with the
32-channel coil in a 0:56 min:sec scan time. Image quality is equivalent for
depiction of the large enhancing parenchymal brain metastasis, as well as two
smaller metastases. (C, D) FLAIR and T2-weighted BLADE 2D axial scans
are also illustrated, both acquired with the 32-channel coil. An IPAT factor of
2 was used for both scans, with these scans typically performed when using
the 12-channel coil without IPAT, leading to almost
A
B
a 2 fold reduction in scan time. In this instance, the
scan times were 1:03*2 and 0:28*2 min:sec, with
both scans providing whole brain coverage using a
C
D
4 mm slice thickness.
CLICK TO RETURN TO PRESENTATION
Click on thumbnails
for a larger view.
Advanced Clinical Brain Imaging at 3 T – SNR and Parallel
Imaging Improvements Offered by a 32 Channel Head Coil Design
FIGURE 8
A .9 x .9 x .9 mm3 voxel size, 2:12 min:sec acquisition time, T2-weighted
SPACE scan is illustrated, acquired with the 32-channel coil. An
arteriovenous malformation is noted in the posterior fossa, illustrated with
high image quality on reformatted images in the sagittal, coronal, and
axial planes.
Click on thumbnails for a larger view.
CLICK TO RETURN TO PRESENTATION
A
B
C
D
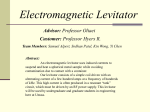
Figure 1 - Diffusion weighted scans are illustrated in a normal volunteer, all acquired with the 32-channel head coil at 3 T. The first three images are with
echoplanar diffusion weighted imaging, comparing (A) the use of no parallel imaging, to implementation of parallel imaging factors (IPAT) of (B) 2 and (C) 4.
Bulk susceptibility artifacts become less evident as IPAT is increased. The pons is relatively poorly depicted with an IPAT of 4, due to lower SNR. (D) illustrates
the equivalent BLADE fast spin echo (FSE) diffusion weighted scan, with no bulk susceptibility artifacts evident. The high SNR of the 32-channel coil makes
acquisition of this scan possible within a reasonable time (3:48 min:sec). All scans were acquired with a b value of 1000.
A
B
E
F
C
D
G
H
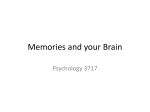
Figure 2 - The same four scan types are illustrated as in Figure 1, in a different normal volunteer, with acquisition in the sagittal (A-D) and coronal (E-H) planes
(A & E no IPAT, B & F IPAT 2, C & G IPAT 4). The capability of the 32-channel coil to perform well (in all planes) with high IPAT values (=4, in C & G) is
noted, together with the advantage of (D & H) the BLADE FSE diffusion weighted scan (made possible by the SNR of the 32-channel coil) for elimination of bulk
susceptibility artifacts. All scans were acquired with a 192 matrix.
A
B
C
D
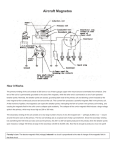
Figure 3 - A patient with multiple punctate acute infarcts is illustrated in (A) with echoplanar diffusion weighted imaging using the 12-channel coil and an IPAT
factor of 2. The capability of the 32-channel coil for higher IPAT factors, and thus less bulk susceptibility artifact, in all planes is illustrated in (B-D) with IPAT 4
scans in the axial, sagittal, and coronal planes.
A
B
C
D
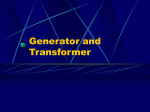
Figure 4 - Diffusion weighted scans in a patient with an acute thalamic infarct are compared. (A) was acquired with the 12-channel coil and an IPAT of 2. (B-D)
were acquired with the 32-channel coil. (B) and (C) are echoplanar technique, with an IPAT of 4, while (D) is the BLADE FSE diffusion weighted scan. Note the
reduction in susceptibility artifact with IPAT 4 in (B) as compared to (A), and the viability of IPAT 4 scans in both the axial and coronal planes with the 32channel coil. Note also the elimination of bulk susceptibility artifact (seen in B, arrow, in this instance originating from the frontal sinus) using the BLADE FSE
diffusion weighted approach.
Figure 5 - A scan acquired with the 12-channel coil using a short TE 2D T1-weighted FLASH scan with 2 averages and an acquisition time of 1:52 is compared
with scans acquired with the 32-channel coil using the same FLASH scan but with 1 average and an acquisition time of 0:56, together with a 2D BLADE
turboFLASH scan with acquisition time of 2:45. All scans are in a normal volunteer.
Figure 6 - Two scans are illustrated, both acquired with the 32-channel coil, in a patient with enhancing (active) multiple sclerosis plaques. The first scan is a short
TE T1-weighted 2D FLASH, with voxel dimensions of 0.9 x 0.9 x 4 mm3, which is substantially degraded (by image blurring) due to patient motion despite the
very short scan time (0:56 min:sec) made possible by use of the 32-channel coil. The second scan is a T1-weighted 2D turboFLASH BLADE, with equivalent
voxel dimension, acquired in 2:45 min:sec. Note the marked improvement in image quality on the BLADE scan, with elimination of the blurring noted in the first
scan due to patient motion.
A
B
C
D
Figure 7 - Scans are illustrated in a patient with brain metastases. (A, B) Short TE 2D T1-weighted FLASH scans are presented, comparing a scan acquired (A)
with the 12-channel coil in a 1:52 min:sec scan time to that acquired (B) with the 32-channel coil in a 0:56 min:sec scan time. Image quality is equivalent for
depiction of the large enhancing parenchymal brain metastasis, as well as two smaller metastases. (C, D) FLAIR and T2-weighted BLADE 2D axial scans are also
illustrated, both acquired with the 32-channel coil. An IPAT factor of 2 was used for both scans, with these scans typically performed when using the 12-channel
coil without IPAT, leading to almost a 2 fold reduction in scan time. In this instance, the scan times were 1:03*2 and 0:28*2 min:sec, with both scans providing
whole brain coverage using a 4 mm slice thickness.
Figure 8 - A .9 x .9 x .9 mm3 voxel size, 2:12 min:sec acquisition time, T2-weighted SPACE scan is illustrated, acquired with the 32-channel coil. An
arteriovenous malformation is noted in the posterior fossa, illustrated with high image quality on reformatted images in the sagittal, coronal, and axial planes.