Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
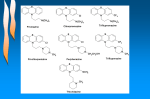
Medicines Q&As Q&A 309.3 What is Neuroleptic Malignant Syndrome? Prepared by UK Medicines Information (UKMi) pharmacists for NHS healthcare professionals Before using this Q&A, read the disclaimer at www.ukmi.nhs.uk/activities/medicinesQAs/default.asp Date prepared: 3rd February 2014 Background Neuroleptic Malignant Syndrome (NMS) is a serious and unpredictable idiosyncratic drug reaction. It is characterised by four groups of symptoms; altered mental state, fever, extrapyramidal symptoms, and autonomic instability (1). The exact cause of NMS is as yet unknown, but it is postulated that dopamine blockade or depletion can lead to abnormal regulation of body temperature and Parkinsonian-like symptoms (2,3). The majority of cases are caused by antipsychotic agents but other drugs with a dopaminergic action may also be implicated. For more detailed information on drugs which may cause NMS, please refer to Medicines Q&A number 324 ‘Which drugs can cause Neuroleptic Malignant Syndrome?’ Answer NMS is a rare but serious idiosyncratic drug reaction which is potentially severe, unpredictable, and may lead to significant adverse effects for the patient (1). NMS generally develops within the first two weeks of an antipsychotic drug being initiated or after a change of dose (1). Incidence rates have decreased from 3% since it was first described in 1960 to around 0.01-0.02% in patients treated with antipsychotics (4). It is thought this decrease is due to increased awareness of the syndrome amongst clinicians leading to earlier diagnosis and a shift to prescribe atypical rather than typical antipsychotics (4). Diagnosis There are many proposed diagnostic criteria available describing NMS, but there is currently no consensus on which set to use (2,5). Generally, either International Classification of Disease (ICD) or Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria are accepted for definitions of mental and neurological diseases. However, although NMS is listed in the DSM, this criteria has not been universally adopted as it has been suggested that if patients present with atypical symptoms, NMS may be missed using this diagnostic tool (5). Diagnosis is therefore symptom-based, and relies on considering and excluding differential diagnoses, which include the following: Serotonin Syndrome (see Medicines Q&A no. 219) Malignant hyperthermia Drug-induced catatonia Infection Heat stroke Toxicity/overdose of other drugs (monoamine oxidase inhibitors, lithium) Drugs of abuse (cocaine, amphetamines, and CNS stimulants) Alcohol or sedative withdrawal(2,3) A 61 year old patient who died due to suspected NMS was found to have high levels of dopamine and its metabolites in her urine. This prompted the authors of a case report to consider whether levels of urinary catecholamines would be helpful to distinguish NMS from serotonin syndrome, although further investigation is required. This approach may be particularly useful in patients who present with an atypical syndrome (6). A number of risk factors have been identified which may predispose patients to developing NMS. These include male sex, mental retardation, iron deficiency, high ambient temperature, depot antipsychotic injections, alcoholism, exhaustion, and dehydration (1, 2). However, NMS is Available through NICE Evidence Search at www.evidence.nhs.uk 1 Medicines Q&As unpredictable and should be considered in any patients in whom symptoms arise, especially since manifestations of agitation or delirium may be difficult to differentiate from escalation of psychosis (7). Symptoms Onset is abrupt and symptoms generally progress rapidly over 24- 72 hours (2). The symptom groups and their main signs are summarised in table 1. Following withdrawal of the causative drug, most patients recover within 7 to 10 days, and virtually all patients recover within 30 days, but symptoms may be prolonged when long-acting depot injections are implicated (3,4). A significant minority of patients may suffer long-term sequelae, including neurological impairment, muscle contraction, and cognitive deficits (1) Table 1: Groups of symptoms and signs of Neuroleptic Malignant Syndrome (2, 3, 8) Altered Hyperthermia Autonomic Instability Muscle Rigidity consciousness Drowsiness Temperature of Fluctuating Blood Creatinine kinase >38.5°C Pressure markedly raised Confusion Tachycardia Extrapyramidal symptoms Stupor Diaphoresis Parkinson-like symptoms Coma Incontinence Trismus (jaw contraction) Delirium Tachypnoea ‘Lead pipe’ rigidity Grand mal High arterial pressure Rhabdomyolysis seizures Opisthotonus (spinal contraction) Babinski’s sign (abnormal flexion of the toes) Chorea Laboratory findings Creatinine kinase is markedly increased, usually between 1,000IU/ml and 100,000IU/L (3). Leukocytosis is present in up to 75% of cases (3). Impaired liver function tests, ECG abnormalities, and electrolyte disturbances may also be present (1). Cerebral CT scans and lumbar punctures are usually normal (2). Temperatures above 104°F (40°C) or renal failure secondary to rhabdomyolysis are indicators of severe NMS and are associated with a poorer prognosis. Further complications can include seizures, disseminated intravascular coagulation, respiratory failure, and aspiration pneumonia (3, 9). Much controversy remains in the literature regarding the causes, diagnosis, and treatment of NMS, and clinical practice appears to vary widely. More research in this field is needed to resolve some of the remaining disparities in understanding of the condition (10). Summary Neuroleptic Malignant Syndrome is a rare but serious idiosyncratic drug reaction. An awareness of the risk factors, causative agents, and symptoms is essential as NMS is a potentially fatal condition. Early recognition of the syndrome may improve management and decrease mortality, so clinicians should be aware of which drugs can cause NMS and how diagnosis is made Symptoms include hyperthermia, autonomic instability, altered consciousness, and muscle rigidity. Laboratory findings include elevated creatinine kinase, leukocytosis and impaired liver function tests NMS is a diagnosis of exclusion, so differential diagnoses must be ruled out. Available through NICE Evidence Search at www.evidence.nhs.uk 2 Medicines Q&As Limitations This Q&A provides only a quick reference guide to the diagnosis and symptoms of neuroleptic malignant syndrome. It does not detail treatment or causative agents. NMS in children is not considered. Both reviews and case reports were used in compiling this Q&A. Further details regarding differential diagnoses were not within the scope of this document. Quality Assurance Prepared by Hayley Johnson, Regional Drug & Therapeutics Centre Date Prepared 3rd February 2014 Checked by Sarah Smith, Regional Drug & Therapeutics Centre Date of check 12th February 2014 Search strategy EMBASE: Neuroleptic Malignant Syndrome + Antipsychotics Neuroleptic Malignant Syndrome + [Amantadine OR Bromocriptine OR levodopa] + Parkinson’s Disease Neuroleptic Malignant Syndrome + Neuroleptic Agents. Limit to 2012-Current MEDLINE: Neuroleptic Malignant Syndrome + Antipsychotics Neuroleptic Malignant Syndrome + [Amantadine OR Bromocriptine OR levodopa] + Parkinson Disease Neuroleptic Malignant Syndrome + Antipsychotics. Limit to 2012-Current Neuroleptic Malignant Syndrome Information Service. www.nmsis.org In-house resources References 1. Troller JN, Chen X, and Sachdev PS. Neuroleptic Malignant Syndrome Associated with Atypical Antipsychotic Drugs. CNS Drugs 2009; 23(6): 477-492. 2. Adnet P, Lestavel P, and Krivosic-Horber R. Neuroleptic Malignant Syndrome. British Journal of Anaesthesia 2000; 85(1): 129-135. 3. Maule E. Management of Neuroleptic Malignant Syndrome. Clinical Pharmacy 2009; 1(7): 203-205. 4. Strawn J, Keck P, and Caroff S. Neuroleptic Malignant Syndrome. The American Journal of Psychiatry 2007; 164(4): 870-876. 5. Pandya M and Pozuelo L. A Malignant Neuroleptic Spectrum: Review of Diagnostic Criteria and treatment implications in three case reports. International Journal of Psychiatry In Medicine 2004; 34(3): 277-28 6. Sokoro AA. Zivot J, and Ariano RE. Neuroleptic malignant syndrome versus serotonin syndrome: the search for a diagnostic tool. Annals of Pharmacotherapy 2011; 45(9): e50 7. Seitz DP and Gill SS. Neuroleptic Malignant Syndrome Complicating Antipsychotic Treatment of Delirium or Agitation in Medical and Surgical Patients: Case Reports and a Review of the Literature. Psychosomatics 2009; 50(1): 8-15. 8. Lader M. Lethal Complications of Antipsychotic Drugs. Clinical Risk 2006; 12(3): 113-117 9. Caroff S. Neuroleptic Malignant Syndrome: Still a Risk, but Which Patients May Still Be in Danger? Neuroleptic Malignant Syndrome Information Service. www.nmsis.org Accessed 03/02/2014. 10. Margetic B, Aukst-Margetic B. Neuroleptic malignant syndrome and its controversies. Pharmacoepidemiology and Drug Safety 2010; 19(5): 429-435. Available through NICE Evidence Search at www.evidence.nhs.uk 3