Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
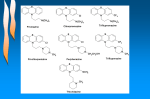
Neuroleptic Malignant Syndrome Synonyms of Neuroleptic Malignant Syndrome Drug-Induced Movement Disorder Hyperthermia Neuroleptic-Induced Acute Dystonia General Discussion Neuroleptic malignant syndrome is a rare but potentially life-threatening reaction to the use of almost any of a group of antipsychotic drugs or major tranquilizers (neuroleptics). These drugs are commonly prescribed for the treatment of schizophrenia and other neurological, mental, or emotional disorders. Several of the more commonly prescribed neuroleptics include thioridazine, haloperidol, chlorpromazine, fluphenazine and perphenazine. The syndrome is characterized by high fever, stiffness of the muscles, altered mental status (paranoid behavior), and autonomic dysfunction. Autonomic dysfunction alludes to defective operations of the components of the involuntary (autonomic) nervous system, leading to wide swings of blood pressure, excessive sweating and excessive secretion of saliva. A genetic basis for the disorder is suspected but not proven. It does appear to be clear that a defect in the receptors to dopamine (dopamine D2 receptor antagonism) is an important contributor to the cause of neuroleptic malignant syndrome. Signs & Symptoms Symptoms of neuroleptic malignant syndrome usually include very high fever (102 to 104 degrees F), irregular pulse, accelerated heartbeat (tachycardia), increased rate of respiration (tachypnea), muscle rigidity, altered mental status, autonomic nervous system dysfunction resulting in high or low blood pressure, profuse perspiration, and excessive sweating. Other symptoms may include liver or kidney failure, abnormally high potassium levels (hyperkalemia), major destruction of skeletal muscle tissue (rhabdo-myolysis) or blood clots in veins and arteries. Causes Neuroleptic malignant syndrome comes about, most likely, as a result of “dopamine D2 receptor antagonism”. Dopamine is a chemical substance (neurotransmitter) found in the brain and elsewhere in the central nervous system that acts to convey messages from one cell to another. In some way, the use of a particular drug blocks the receptor in the brain cell for dopamine. When the dopamine receptors in the hypothalamus or another bundle of nerve fibers (nigrostriatal pathways) and/or the spinal cord are blocked, increased muscle rigidity is the result. The interference with the dopamine receptors in the hypothalamus is also probably responsible for high body temperature, as well as the swings in blood pressure. Some clinicians believe that neuroleptic malignant syndrome may be related to malignant hyperthermia, a genetic disorder characterized by an abnormal reaction to anesthesia drugs. (See related disorders section for more information about malignant hyperthermia.) Affected Populations Neuroleptic malignant syndrome may affect any person taking neuroleptic drugs. Men appear to be at higher risk than women. Some clinicians believe that the stronger neuroleptic medications are more likely to precipitate an attack of NMS. Although two-thirds of cases are thought to occur within the first week of start of treatment, the syndrome may begin at any time during treatment. Recurrence of an attack of NMS is not uncommon. The risk of recurrence is closely related to the time elapsed between the end of the original episode of neuroleptic malignant syndrome and the beginning of renewed administration of an antipsychotic drug. If the waiting period is two weeks or less, about 63% will have a recurrence. If the waiting period is more than two weeks, the percentage of patients experiencing a relapse drops to about 30. Related Disorders Symptoms of the following disorders can be similar to those of neuroleptic malignant syndrome. Comparisons may be useful for a differential diagnosis: Anaphylaxis is an abnormally severe allergic reaction to a substance. Major symptoms may include severe itching, hives, flushing, swelling, vomiting, diarrhea, difficulty breathing and unconsciousness. High fever is not a symptom of this disorder. (For more information on this disorder, choose “Anaphylaxis” as your search term in the Rare Disease Database.) Lethal catatonia is a condition similar to NMS and not infrequently confused with it. A detailed history may indicate that the patient has endured catatonic states while not on neuroleptic medications. If so, the chances are that the presenting syndrome is NMS. A lethal catatonia patient will respond to the administration of neuroleptics. It is, however, almost impossible to predict whether the patient’s symptoms will worsen or improve. Patients with lethal catatonia almost invariably endure a period of agitation and excitement prior to the catatonia. This is in contrast to the patient with NMS in which the first symptom is usually muscular rigidity. Heat stroke is a very serious condition characterized by an abrupt and rapid increase in body temperature that may reach as high as 104 to 106 degrees F. Heat stroke usually results from exposure to an extremely hot environment. The skin may become hot, flushed and dry. Rapid loss of fluids may result in the inability to sweat. Sweating is necessary to cool the body. There may also be an increase in pulse rate and respiration. The affected individual may become disoriented and eventually experience convulsions or slip into unconsciousness. Measures such as wrapping the individual in cold, wet sheets should be taken immediately to lower body temperature. An individual suffering from heat stroke should be hospitalized as quickly as possible. (For more information on this disorder, choose “Hyperthermia” as your search term in the Rare Disease Database.) Malignant hyperthermia is a genetic disorder characterized by an abnormal response to muscle relaxants and general anesthesia drugs. Symptoms of Malignant Hyperthermia are apparent only after the patient has been placed under general anesthesia. Along with rapidly elevating body temperature that may rise as high as 110 degrees, muscle rigidity and/or muscle twitching occurs. The patient may also exhibit a very rapid and irregular heartbeat, abnormally low blood pressure, sickly sweet breath, headache, nausea and vomiting. It is not known whether neuroleptic malignant hyperthermia is a variant form of Malignant Hyperthermia, but some researchers have suggested that these disorders may be related. (For more information on this disorder, choose “Malignant Hyperthermia” as your search term in the Rare Disease Database.) The serotonin syndrome mimics neuroleptic malignant hyperthermia. If the use of selective serotonin reuptake inhibitors (SSRIs) results in symptoms such as altered mental state, autonomic dysfunction (see above), and neuromuscular defects, then the condition is likely to be serotonin syndrome. Since SSRIs are being used in increasing amounts, it is not unreasonable to expect that the incidence of serotonin syndrome will increase as well. The serotonin syndrome may be distinguished from NMS in most cases by a detailed history in which any changes in medication and/or dosages are clarified. In addition, serotonin syndrome usually is not accompanied by severe muscle rigidity. The following disorder may be associated with the extended use of neuroleptic drugs. It is not necessary for a differential diagnosis: Tardive dyskinesia is a disorder that results from the long-term use of neuroleptic drugs and is characterized by involuntary and abnormal movements of the jaw, lips and tongue. Typical symptoms include grimacing, sticking out the tongue, and sucking or fishlike movements of the mouth. A high percentage of schizophrenic people who have spent long periods of time in mental hospitals taking neuroleptic drugs have a high risk of developing tardive dyskinesia. (For more information on this disorder, choose “tardive dyskinesia” for your search term in the Rare Disease Database.) Diagnosis The diagnosis of neuroleptic malignant syndrome is based on the presence of characteristics that include treatment with neuroleptic drugs within the past 1-4 weeks. high body temperature (greater than 38 degrees centigrade); muscle rigidity; and at least five of the following: Change in mental status Rapid heart beat (tachycardia) Low or high blood pressure (hypo- or hypertension) Excessive sweating (diaphoresis) Excessive saliva production (sialorrhea) Tremor Incontinence Increased creatine phosphokinase, or increased urinary myoglobin Increased number of white blood cells (leukocytosis) Increased concentrations of metabolic acids in blood and urine Exclusion of other drug-induced psychiatric or systemic illness. Standard Therapies Treatment Treatment of neuroleptic malignant syndrome consists of withdrawal of neuroleptic medications under a doctor's supervision, immediate measures to restore appropriate water and nutrient levels, and steps to lower the individual's body temperature. Medications prescribed as treatment may include skeletal muscle relaxants, such as dantrolene; stimulators of dopamine production and activity, such as bromocriptine; and/or continuous perfusion of central nervous system depressants, such as diazepam. Complications that may result from neuroleptic malignant syndrome, such as kidney (renal) insufficiency, deficiency of oxygen reaching the tissues (hypoxia), and/or decreased alkalinity of the blood and tissues (acidosis) can be extremely serious and must be treated immediately. Once patients have recovered from neuroleptic malignant syndrome, about 87% will be able to tolerate an antipsychotic at some point in the future. Physicians usually switch to a different antipsychotic class and to an atypical antipsychotic. Such patients must be carefully monitored since recurrences of neuroleptic malignant syndrome are not infrequent. Electroconvulsive treatments have been prescribed for patients with neuroleptic malignant syndrome with varied results. Investigational Therapies Information on current clinical trials is posted on the Internet at www.clinicaltrials.gov. All studies receiving U.S. government funding, and some supported by private industry, are posted on this government website. For information about clinical trials being conducted at the National Institutes of Health (NIH) in Bethesda, MD, contact the NIH Patient Recruitment Office: Tollfree: (800) 411-1222 TTY: (866) 411-1010 Email: [email protected] For information about clinical trials sponsored by private sources, contact: www.centerwatch.com Supporting Organizations Malignant Hyperthermia Association of the United States o o o o o o MedicAlert Foundation International o o o o o o 3803 N. Fairfax Drive Suite 100 Arlington, VA 22203Phone: (703) 524-7600 Toll-free: (800) 999-6264 Email: [email protected] Website: http://www.nami.org National Mental Health Consumers’ Self-Help Clearinghouse o o o o o o o 2000 N. Beauregard Street, 6th Floor Alexandria, VA 22314-2971 USA Phone: (703) 684-7722 Toll-free: (800) 969-6642 Email: [email protected] Website: http://www.mentalhealthamerica.net/ National Alliance on Mental Illness o o o o o o o 2323 Colorado Avenue Turlock, CA 95382 USA Phone: (209) 669-2401 Toll-free: (888) 633-4298 Email: [email protected] Website: http://www.medicalert.org Mental Health America o o o o o o 1 North Main St PO Box 1069 Sherburne, NY 13460 USA Phone: (607) 674-7901 Email: [email protected] Website: http://www.mhaus.org 1211 Chestnut Street Suite 1207 Philadelphia, PA 19107-6312 USA Phone: (215) 751-1810 Toll-free: (800) 553-4539 Email: [email protected] Website: http://www.mhselfhelp.org NIH/National Institute of Mental Health o o o o o o Health Science Writing, Press and Dissemination Branch 6001 Executive Boulevard Bethesda, MD 20892-9663 Phone: (301) 443-4513 Toll-free: (866) 615-6464 Email: [email protected] o Website: http://www.nimh.nih.gov/index.shtml North American Malignant Hyperthermia Registry o o o o o o o Penn State University Dept. of Anesthesiology Hershey, PA 17033-0850 USA Phone: (412) 692-6390 Toll-free: (888) 274-7899 Email: [email protected] Website: http://www.mhreg.org