Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
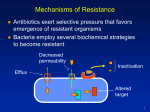
ANTIBIOTIC RESISTANCE LauraLe Dyner MD Pediatric Infectious Disease Fellow June 2009 Antibiotic Resistance Relative or complete lack of effect of an antimicrobial agent n An organism is able to grow in readily achievable serum concentrations of the antibiotic in question n n Increase in MIC/Decrease in disk diffusion Minimum Inhibitory Concentration (MIC) Lowest concentration of antimicrobial that inhibits the growth of the organism after an 18 to 24 hour incubation period n Interpreted in relation to the specific antibiotic and achievable drug levels n Can not compare MICs between different antibiotics n Discrepancies between in vitro and in vivo n MIC/Disk Diffusion Antibiotic Resistance n Intrinsic resistance Occurs naturally in all or most strains of that species q Chromosomally encoded q Gramnegatives are resistant to Vancomycin q n Acquired resistance q Results from a mutation in the existing DNA of an organism or acquisition of new DNA Timeline of Antibiotic Resistance Factors That Promote Resistance Exposure to suboptimal levels of antimicrobials n Exposure to broadspectrum antibiotics n Exposure to microbes carrying resistant genes n Lack of hygiene in clinical environments n Use of antibiotics in foods/agriculture n Inappropriate Antimicrobial Use Prescriptions not taken for a total duration of therapy n Antibiotics for viral infections n Antibiotics sold without medical supervision n CDC Estimates Consequences of Increased Resistance Infections that are difficult to treat n Increased mortality n Increased cost of therapy n MDRTB q Cost per tablet q n n n PCN $0.24 Linezolid $86.90 360 x as much Genetic Basis of Resistance n Chromosomal n n n Mutation Chromosomally mediated inducible enzymes Plasmid n n n n Most common genetic basis of resistance Genetic determinants can spread laterally through a population without cell division Interspecies lateral transfer of plasmids Resistance usually involves antibiotic inactivating enzymes (many encoded by transposons) Selection of Resistant Bacteria Mechanisms of Resistance Enzymatic Inactivation** n Decreased permeability n Efflux n Alteration of target site n Overproduction of target n Decreased Permeability n Outer membrane permeability Gramnegative bacteria q Impedes the entry of hydrophobic antibiotics (nafcillin/erythromycin) q Porins q q n Loss of porins leads to increased resistance to blactams Inner membrane permeability q Altered proton motive force leading to aminoglycosideresistance after long term use Efflux n Tetracyclines q Energydependent transporter system Fluoroquinolones n Chloramphenicol n Macrolides n mef gene (macrolide efflux) q S pneumo, S aureus, S epidermidis q Target Sites 1955 1962 1985 1940 1990 2000 1959 1950 1962 1955 1948 1944 1947 1963 Altered target sites n Cell wall PBPs: S pneumo, N meningitidis, MRSA q DAlaDAla target: VRE q n VanA, VanB, VanC, VanD Cell membrane changes n Ribosomal alterations n Tetracyclines, macrolides, lincosamides, aminoglycosides q Failure of the antibiotic to bind to the ribosome disrupts the ability to inhibit protein synthesis q Penicillin Binding Proteins (PBP) n More common resistance mechanism for grampositive organisms n Gramnegative access to PBPs is limited due to the outer membrane Target for all blactams n Found as membranebound & cytoplasmic proteins n Involved in the final stages of peptidoglycan synthesis of cell walls n Inactivating enzymes blactamases** n Aminoglycoside modifying enzymes n Chloramphenicol acetyltransferase n Macrolide, Lincosamide, & Streptogramin inactivating enzymes n Tetracycline inactivation n tetX enzyme q Although most tetracycline resistance is mediated by efflux & ribosomal protection q b-lactamases Large, diverse family of enzymes n Wide range of activity n ESBLs q AmpC blactamases q Carbapenemases q n Widely dispersed Grampositive q Gramnegative q n q Major mechanism of resistance in gramnegatives Anaerobes b-lactam Mechanism of Action blactam antibiotic binds to PBP n Inhibition of peptidoglycan synthesis n q n Inhibits synthesis of crosslinks Cell death b-lactamases q Split the amide bond of the blactam ring b-lactamases: Structural Classes n n n n Class A n Plasmid mediated n Serine residue at the active site n Preferentially hydrolyze penicillins Class B n Chromosomal n Metalloenzymes; zincbinding thiol group n Hydrolyze carbapenems, penicillins, & cephalosporins Class C n Chromosomal n AmpC n Mainly active against cephalosporins Class D n Plasmid mediated n Oxacillinhydrolyzing enzymes b-lactamases: Classification AmpC n Confers resistance to Cephamycins (cefotetan, cefoxitin) q Oxyiminoblactams (ceftriaxone, cefotaxime, ceftazidime) q Chromosomal in SPACE organisms & are inducible n Plasmid mediated in other gramnegatives & usually not inducible n Not inhibited by blactamase inhibitors n AmpC Carbapenemases n n Can hydrolyze penicillins, cephalosporins, monobactams, & carbapenems. Groups q Metallo blactamases (MBLs) n n q Confer a high level of resistance Pseudomonas, Acinetobacter, Enterobacter Serine blactamases n Oxacillinases or D blactamases (OxaA) q q q n Not as diverse Acinetobacter Another resistance is usually necessary to raise the MIC Class A Carbapenemases q q Pseudomonas & Enterobacter Klebsiella: predominant type (plasmid) ESBL Mediated Resistance n Contain a number of mutations that allow them to hydrolyze expandedspectrum βlactam antibiotics n Derived from older antibiotichydrolyzing b lactamase enzymes (TEM1, TEM2, SHV1) q q q q n A single amino acid substitution can give rise to new ESBLs Not as catalytically efficient Inhibited by βlactamase inhibitors Susceptible to cefoxitin and cefotetan in vitro only 10%–40% of K pneumoniae, E coli express ESBLs Distinction between AmpC & ESBL n The AmpC b Lactamases are encoded by genes located on chromosomes q q q n n n Often inducible Commonly found in Enterobacter sp, Citrobacter freundii, Morganella morganii, Serratia marcescens, and Pseudomonas aeruginosa. The genes are not easily transferable to other bacterial species ESBLs are encoded by genes located on plasmids, resulting in easy transfer to other bacterial species. AmpC b Lactamases are weakly inhibited by b Lactamase inhibitors (clavulanic acid) and usually confer resistance to cephamycins In contrast, ESBLs are generally well inhibited by b Lactamase inhibitors and usually retain sensitivity to the cephamycins (in vitro) Resistance Against Specific Antibiotics Betalactams β lactamases Alteration of PBPs Aminoglycosides Enzyme modification of the drug common Ineffective transport Altered ribosomal binding site (30S) – rare Macrolides Decreased permeability of cell wall to drug Alteration in the 50S ribosomal binding site Inactivation by enzymatic hydrolysis (esterase) Efflux pump Sulfonamides Overproduction of PABA Trimethoprim Plasmid mediated dehydrofolate reductases Vancomycin Low frequency of resistance Resistance Against Specific Antibiotics Cephalosporins Extended Spectrum Beta Lactamases (ESBL) Chromosomal cephalosporinases bLactamase Inhibitors Hyperproducers of blactamases New blactamases resistant to inhibitors Chromosomal cephalosporinases Carbapenems Porin mutations Efflux pump overproduction (excluding Imipenem) Zinc Metalloenzymes and other blactamases Fluoroquinolones Decreased number of porins in target cells Efflux mechanisms Mutations in DNA gyrase & topoisomerase) Specific Organisms n Staphylococcus aureus n n n MRSA VISA VRSA Group A (betahemolytic) Strep n Streptococcus pneumoniae n Enterococcus n n n VRE “SPACE” (Serratia, Pseudomonas, Proteus, Acinetobacter, Citrobacter, Enterobacter) Staph Aureus n Produce blactamases Preferentially hydrolyze penicillins q Encoded for on bacterial plasmids or transposons q At LPCH approximately 18% of S aureus is susceptible to penicillin or ampicillin n Methicillin & nafcillin are resistant to penicillinase n Resistance has increased in recent years n Methicillin Resistant Staph Aureus (MRSA) 1959: n 1961: n 1968: n 1974: n 1981: n 2002: n n 2007: Methicillin introduced MRSA discovered in England MRSA found in the US (Boston) 2% of hospital staph infections MRSA acquired in the community Community & hospital acquired infections are found to be genetically different In the US: 94,000 severe infections/yr & 19,000 deaths/yr MRSA Most frequent nosocomial resistant pathogen n Acquired via MecA n Chromosomal mutation leading to the synthesis of a new penicillin binding protein n The protein is inducible & confers resistance to all beta lactam antibiotics n MecA n Encodes for PBP 2a q n n Weak affinity for methicillin & all βlactams Speculation that the origin was from coagulase negative Staph or E coli Mobile chromosomal element called staphylococcal cassette chromosome (SCCmec) n SCCmec types I, II, and III q q q n Multidrug resistant Large cassettes Healthcare associated SCCmec type IV and type V q q Not multidrug resistant Community associated Clindamycin Resistance: D-test n Resistance to macrolides (e.g. erythromycin) can occur by two different mechanisms Mechanism Clinda Efflux Gene msrA Ribosome Alt. erm erm Erythro R S R R S* R Clindamycin Resistance: D-test VISA/VRSA n VISA: Vancomycin Intermediate Staph Aureus q n VRSA: Vancomycin Resistant Staph Aureus q n MIC 48 ug/ml MIC > 16 ug/ml Glycopeptide resistance Group A Strep 100% susceptible to penicillin & other beta lactam antibiotics n Some are resistant to macrolides n q In a European surveillance, it has been found to be as high as 1/3 resistant Streptococcus pneumoniae n Resistance to penicillin due to stepwise mutations in penicillin binding proteins (PBP) q q q q n n Chromosomally mediated Decreased affinity to PBP Can be overcome with highdose penicillin Alterations in PBPs decrease susceptibility of the organism to other beta lactam antibiotics Macrolides q Genetic changes to binding target on ribosomehigh level can not be overcome = erm(B) q Efflux pumplower levelmay be overcome = mef (A) Vancomycin is used to treat penicillin & cephalosporin resistant infections Enterococcus n Intrinsic resistance q q q q n Chromosomal Less susceptible to penicillin & ampicillin than other streptococci (MIC 28 ug/ml) [by 101000 x] Low level of resistance to aminoglycosides Synergy between a cell wall agent & an aminoglycoside Acquired resistance q q Beta lactamase production High level of resistance to aminoglycosides n q Lose synergy ability as well Glycopeptide resistance (Vancomycin) Vancomycin Resistant Enterococci (VRE) n n First reported in 1988 Origins q q q q n n Normal fecal flora Food chain Selection by use of Vancomycin, Cephalosporins, Anaerobic Antibiotics Persontoperson spread Produce a new membrane protein to inhibit binding of vancomycin to DalanylD alanine terminus Lack of synergy with aminoglycosides Vancomycin Resistant Enterococci (VRE) “SPACE” Organisms Gramnegative bacteria have a chromosomal gene for the b lactamase, ampC n SPACE organisms can undergo singlestep mutations to constitutive, highlevel enzyme production n If enough ampC betalactamase is produced, resistance occurs n Conclusion n Combat Antibiotic Resistance! Narrow antibiotic coverage when possible n Restrict antimicrobial use n q At LPCH: Linezolid, Micafungin, Caspofungin Track resistance patterns n Direct Observed Therapy (TB) n Resources n n n n n n n Centers for Disease Control Johns Hopkins Antibiotic Guide UpToDate 2009 Nature The 2006 American Academy of Pediatrics Redbook Mandell’s Prober, Long, & Pickering. Principles & Practice of Pediatric Infectious Disease, 3 rd Edition