Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
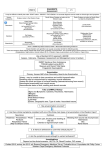
Environmental Medicine expert topics Heat related illness Epidemiology Equal male to female ratio Higher risk at extremes of age <4yrs and >75yrs Major risk factors include o In children – CNS or diarrheal disease o Alcoholics o Medications – antipsychotics, tranquilizers, anticholinergics, anti-parkinsonian drugs o Cardiovascular medications – β-blockers, CCB and vasodilators Other risk factors for exertional heat illness include o Obesity o Dehydration o Vigorous exertion in hot environment without acclimitisation o Rare disorders – absence of sweat glands, systemic scleroderma, hyperthyroidism and pheochromocytoma Mortality from heat stroke may range from 10-75% Mechanisms of heat transfer Body regulates heat content through four mechanisms: Radiation – o Primary mechanism of heat loss when environmental temperature is lower than body temperature. o Radiative loss occurs through the infrared range of electromagnetic spectrum o Accounts for 60% of body cooling in colder conditions o When surrounding environment is hot, heat will be gained by radiation o Direct sunlight accounts for 100-250 kcal/h of heat burden Conduction – o Kinetic energy from warm surface directly transferred on to less active surface molecules of cooler surface o Usually accounts for <3% of total heat loss of body Convection o Heat transfer to air or fluid around the body e.g. thin air layer between body and clothes, use of fans and cooler layer of air around skin o Can along with conduction be responsible for up to 15% of heat loss Evaporation o Primary heat loss mechanism of the body in higher temperatures o Each gram of water evaporating from skin and lungs removes about 0.58kcal of heat o Even in the absence of sweating, a basal level of skin and respiratory evaporation (insensible loss) accounts for about 600 mL of water daily and 12 to 16 kcal of heat loss per hour. o Evaporation accounts for over 25 percent of the heat lost in cooler settings and virtually 100 percent at high environmental temperatures. o Each 1 percent decrease in body weight from dehydration results in a core temperature increase of 0.1°C to 0.3°C (0.18°F to 0.54°F). o Highly acclimatized humans can achieve sweating rates that exceed gastric emptying rates. Such sweating rates outstrip the ability of the gastrointestinal tract to absorb water and result in dehydration and eventual hyperpyrexia. o Sweating rates faster than 1L/hr are not sustainable with oral hydration alone Response to heat stress Body tends to maintain its core temperature between 36 – 38˚C. native thermal regulation mechanisms begin to fail at core temperatures below 35˚C and above 40˚C. Physiologic response to heat stress occurs through four primary methods: o Dilatation of blood vessels o Increased seat production o Decreased heat production and o Behavioral heat control The primary function of heat regulation mechanisms in the human body seems to be for prevention of heat loss in the cold environments. It is by the release or reversal of these heat conserving mechanisms that heat loss or gain is achieved. Skin blood flow can be increased from basal level of 0.2L/min to 8L/min in response to heat stress. Cardiac output will thus increase by 3L/min for each 1˚ increase in core temperature Any patient with impaired CV status or medications that prevent this increase, may not be able to maintain this output. Heat stress thus may also result in arrhythmias, ischemia and exacerbation of CCF. Classification of heat-related illnesses Minor syndromes o Heat edema o Prickly heat o Heat cramps o Heat exhaustion Major syndromes o Heat stroke Heat stroke The classic definition of heatstroke includes: presence of temperature >40˚C, CNS dysfunction and anhidrosis. Lack of sweating may not be present and is not a absolute criterion for diagnosis. Therefore anyone with temperature and CNS dysfunction should be considered to have a heatstroke, which is a medical emergency with multiple organ system involvement and high mortality rate requiring immediate intervention. Clinical features CNS symptoms – Very variable from irritability, confusion to seizures and coma. Cerebellum very sensitive to heat and ataxia can be early neurologic finding The distinction between exertional and non-exertional heatstroke is not clinically important since signs, symptoms and management are the same. Definitive diagnosis is of exclusion and once made should be aggressively treated. System effects of hyperthermia Cardiovascular o Tacyarrhythmias and hypotension – may be hyperdynamic or hypodynamic depending on patient’s baseline health status Neurological o Due to metabolic disarray, cerebral edema or ischemia o Symptoms as above Rhabdomyolysis o Direct injury to cells with leaking of calcium and phosphate o o Hyperphosphatemia and hypercalcemia Hypokalemia due to Direct catecholamine effect Associated with hyperventilation and respiratory alkalosis Sweat losses and renal wasting from physiological hyperaldosteronism Late hyperkalemia worsened by ARF and hypocalcemia Hyperuricemia from release of purines from muscle breakdown o o Renal o Renal failure Direct thermal injury Pre-renal insults from volume depletion, renal hypoperfusion, Rhabdomyolysis and DIC Hematological o Petechial hemorrhages, ecchymoses due to direct thermal injury and DIC from consumptive coagulopathy Immunological o Release of inflammatory mediators due to direct thermal injury and tissue injury with a SIRS response GIT o Blood redistribution from splanchnic circulation to periphery causing gut ischemia and diarrhea with further fluid loss and poor absorption Differential Diagnosis of Heatstroke Drug toxicity: anticholinergic toxicity, stimulant toxicity (phencyclidine, cocaine, amphetamines, ephedrine), salicylate toxicity Drug withdrawal syndrome: ethanol withdrawal Serotonin syndrome Neuroleptic malignant syndrome Generalized infections: bacterial sepsis, malaria, typhoid fever, tetanus Central nervous system infections: meningitis, encephalitis, brain abscess Endocrine derangements: diabetic ketoacidosis, thyroid storm Neurologic: status epilepticus, cerebral hemorrhage Investigations Bedside BSL – may be elevated in 70% of patients ABG – if significant metabolic and respiratory compromise suspected ECG – evidence of primary arrhythmia due to hyperthermia or secondary to electrolyte abnormalities Urinalysis – may show false positive blood due to myoglobinuria Laboratory EUC – o Hypokalemia o Hyperphosphatemia o Hypercalcemia o Hyperkalemia and hypocalcemia o Renal impairment Raised serum Uric acid level LFT – may be deranged in severe cases with multi-organ dysfunction CK – usually elevated severely Coagulation studies – may be deranged with impending DIC CXR – signs of aspiration, ARDS Toxicology screen – to rule out suspected causes Lumbar puncture and CT brain as indicated by clinical features Management Supportive care and monitoring Mortality approaches 100% if prompt and effective treatment not instigated Rapid cooling associated with improved outcomes Goals of treatment – rapid colling and supporting organ function adequacy of airway, breathing, and circulation; initiation of high-flowoxygen; use of continuous cardiac monitoring and pulse oximetry; and intravenous access central venous access and invasive arterial blood pressure monitoring indicated if elderly patient requiring close monitoring of fluid status Comparison of Cooling Techniques Technique Advantages Disadvantages Evaporative Simple and readily available Shivering Spraying with tepid water and Difficult to maintain monitoring fanning electrodes in position Noninvasive, easy patient access Relatively effective Immersion Noninvasive Shivering Relatively effective Cumbersome More rapid than evaporative Poorly tolerated Logistically difficult to access Difficult to maintain monitoring electrode and temperature probes Ice packing Noninvasive Shivering Readily available Poorly tolerated Strategic ice packs Noninvasive, readily available Shivering, poorly tolerated Can be combined with other Medium efficiency techniques 1˚ every 10minutes Cold gastric lavage Generally available Invasive Labor intensive Potential for water intoxication May require airway protection Limited human experience Cold peritoneal Theoretically beneficial Invasive lavage Limited human experience Body cooling units Accelerated evaporative losses Same as evaporative Cardiopulmonary bypass 2-3 times more effective than immersion Used for resistant cases with cardiac compromise Highly invasive Additional therapy: Cease cooling methods at 38.5 - 39˚ to avoid reverse hypothermia Diazepam 5-10mg IV to reduce shivering Chlorpromazine 25-50mg IV to inhibit shivering – second line Neuromuscular paralysis with non-depolarising agents if resistant to cooling Anti-pyretics not helpful Maintain urine output at 1 – 1.5ml/kg/hr with fluid boluses, diuretics Consider renal dialysis if anuria, hyperkalemia or sever metabolic acidosis Treat coagulopathy with FFP and platelets Complications of heatstroke CNS - Encephalopathy, edema, neuronal injury and hemorrhages Hepatic damage – hallmark of heatstroke Cardiac – myocardial injury Renal – ARF due to heat damage, Rhabdomyolysis and hypotension Respirator – ARDS GIT – pancreatitis Hematologic – DIC and thrombocytopenia Hypothermia Hypothermia is defined as a core temperature of less than 35˚C. Individuals at extremes of age and those with altered sensorium are at increased risk due to decreased ability to increase heat production and to conserve heat. Pathophysiology Heat loss from body occurs through: o Radiation o Conduction o Convection and o Evaporation Shivering increases metabolic rate by 2-5times and only maintained until glycogen stores last and temperatures of 30˚C. Cardiovascular effects o Initial tachycardia and peripheral vasoconstriction → increase in cardiac output o Subsequent bradycardia, hypotension and fall in CO o Loss of vascular tone at 24˚C o Osbourne J waves in ECG below 32˚C o Progressive bradycardia with progressive hypothermia due to decreased automaticity of pacemaker cells o Increased risk of VF at low temperatures o Antiarrhythmic therapy ineffective at temperatures <30˚C, so are inotropes CNS o Loss of fine motor and then gross motor skils o Progressive decline in consciousness o Cerebrovascular autoregulation lost at 24˚C o Rigidity, pupillary dilatation and areflexia as temperature falls below 28˚C o May simulate rigor mortis Respiratory system o Early stimulation followed by depression as metabolism slows o Significant fall in O2 consumption and CO2 production o Initial left shift of O2 dissociation countered by lactic acidosis, with severe hypothermia overall-right shift of O2 dissociation curve Renal system o Cold induced diuresis initially with drop in temperature o Further hypothermia causes reduced cardiac output and renal blood flow and thus reduced GFR o ARF develops in 40% patients Endocrine o BMR reduced to 50% by 28˚C o Hypoglyecemia in case of slow hypothermia and hyperglycemia with rapid cases o Hypokalemia due to EC K flow into cells o Hyperkalemia usually late from cell lysis GIT o Reduced GI motility with reduced temperature, ileus at 28˚ o Pancreatitis and mesenteric artery thrombosis from reduced flow may occur Hematological o ↑viscosity, fibrinogen and hematocrit o Hematocrit ↑2% for every 1˚C decline due to hemoconcentration o Coagulopathy may develop with thrombocytopenia and DIC reported Causes of hypothermia Accidental – environmental Metabolic Hypothalamic and CNS dysfunction Drug-induced Sepsis Dermal disease Acute incapacitating illness Iatrogenic – fluid resuscitation Classification on severity Mild (35-32˚C) o ↑BMR, maximum shivering and thermogenesis o Amnesia, dysarthria, ataxia, apathy o Respiratory stimulation o Normalblood pressure Moderate (32-28˚C) o Stupor o Shivering ceases o AF and other dysrhythmias o Poikilothermia – adopting temperature of surroundings o Reduced pulse and cardiac output – 2/3rd of normal o Progressive loss of consciousness, pulse and respiration, pupils dilated o Susceptible to VF Severe (<28˚C) o Loss of reflexes and voluntary motion o Major acid-base derangements o Pulmonary edema, significant hypotension may develop o ↓CBF and CO o Absent corneal and oculocephalic reflexes o Maximum risk of VF at 22˚C o Flat EEG at 19˚ and asystole at 18˚ Investigations Bedside BSL – hypo- or hyperglycemia ABG – reflecting metabolic state ECG – many sequential changes – discussed later Laboratory EUC – abnormal renal function, potassium disorders CK may be eleveated Pancreatitis – raised lipase and amylase FBC – raised hematocrit due to hemoconcentration ECG Changes in Hypothermia T-wave inversions PR, QRS, QT prolongation Muscle tremor artifact Osborn (J) wave- J wave seen in inferior leads, may be seen with SAH, CHI and MI Dysrhythmias: Sinus bradycardia Atrial fibrillation or flutter Nodal rhythms AV block PVCs Ventricular fibrillation Asystole Management Supportive care and monitoring Airway must be secured in any patient with reduced level of consciousness, initial reports of increased risk of VF with intubation have not been confirmed Intubation and ventilation with warm humidified air may be an adjunctive treatment and improve hemodynamics Gain IV access since IM/SC routes not feasible since no peripheral blood usually present NGT, IDC insertion for monitoring and therapeutic use IV fluid therapy – warm fluids to correct dehydration and aid with temperature correction Antiarrhythmic drug and inotropes usually ineffective when <30˚C Defibrillation for VF also unlikely to succeed at low temperatures but should be tried initially if needed Specific management options Endogenous rewarming Ideal for mild hypothermia Rewarming of about 0.5 – 2.0˚ per hour possible, more if able to exercise Warm environment, warm clothing and insulation Passive external rewarming Suffiecent for stable patients with mild hypothermia Remove wet clothing, place in warm dry environment Cover with blankets Same as above Active external rewarming For moderate hypothermia External application of heat – warm blankets, radiant heat or forced heated air system Up to 2˚C per hr increase achievable Active core rewarming For severe hypothermia Warmed humidified inhaled oxygen o Prevent further heat loss o Modest heat gain Blood warmer for blood and IV fluids o Prevents further heat loss with therapy rather than increase temperature o Cardiopulmonary bypass or left pleural lavage – lifesaving in arrested hypothermics o Mediastinal, gastric, peritoneal and bladder lavage – less effective, more adjunctive Venomous bites and stings Snakes – refer to toxinology notes Spiders – refer to toxinology notes Hymenoptera – bees, wasps, ants Hymenoptera means membrane wings, and includes: Vespids (yellow jacket or European wasp and paper wasps) Aspids (honey bees) Ants Saw flies Bees can only sting once, wasps may sting multiple times. Stinging causes local pain and irritation. Reaction to a sting depends on prior exposure and sensitivity. Bee stings cause approximately one death per year in Australia. Nearly all deaths due to anaphylaxis Occasionally due to massive envenomation Anaphylactic reaction to insect venom is an absolute indication for venom immunotherapy, as this is protective against further severe reactions in >80-90% cases Bee swarming Venom contains Melittin Phospholipase A2 Hyaluronidase Assessment Vomiting, diarrhea, Shock Hemoglobinuria, rhabdomyolysis Multiple organ failure Signs of anaphylaxis if sensitive Prognosis 15% mortality with massive envenomation Death likely if >20stings/kg and mild illness if 1-4stings/kg. Wasp stings European wasp lives on ground, earth banks and walls Attracted to sweet food, so tendency for oral stings Does not leave sting behind like bees, so can sting multiple times Most serious reactions due to allergic reactions Life threatening envenomation occurs when attacked by swarms and >50stings Death usually due to anaphylaxis as massive envenomation rare Massive envenomation Hemolysis, myocarditis, hepatitis Management Ice, analgesia, management of anaphylaxis if present Supportive management for all other manifestations Ticks Most fatalities from tick paralysis were recorded before 1945. Neuromuscular paralysis and death from ticks is unique to Australia. 3 of 19 Australian species known to secrete paralytic toxin Nearly all cases due to scrub tick (Ixodes holocyclus), found on eastern seaboard Only caused by the female tick Natural hosts – bandicoots and other mammals such as dogs Attaches to host via proboscis Attachment may cause local necrosis, tick digs further deeper to re-attach Larval forma may cause allergic reaction in infested host Tick venom Holocyclotoxin – slows action potential and has botulinum like effect on Ach release Effects of tick bites Local skin irritation, rash and tick paralysis Local and systemic allergic reaction Bite site infection and Tick borne diseases Tick paralysis Paralysis and fatality more common in children <5yrs Consider tick paralysis in any child with o ataxia or progressive weakness o ascending symmetrical paralysis local paralysis well documented – e.g. facial untreated can progress to full respiratory paralysis – cause for most deaths Assessment onset of symptoms 4-5 days after attachment longer the attachment – more likely the paralysis unsteady gait, ataxia, distal muscles first affected generalized weakness – unable to walk swallowing difficulties, Bell’s palsy ascending flaccid paralysis – GBS important DD paralysis may worsen for up to 48hrs after tick removal Management Tick removal unless removed intact, prolonged local inflammatory reaction is common don’t squeeze body many methods documented – knot method, forceps and other commercial devices do not crush or squeeze the tick’s body, do not apply heat or other substances to tick symptoms may improve immediately or worsen slightly after tick removal thus any symptomatic tick bite patient should be admitted for observation Tick antivenom indicated in severe envenomation may confer some benefit but not reverse established paralysis made from dog IgG – one vial contains 1000 units f neutralizing capacity dose of 1-2 ampoules depending on severity, slow IV infusion over 15-30 minutes serum sickness may occur Supportive management general supportive care and ventilatory support as indicated tetanus prophylaxis routine antibiotic prophylaxis not indicated Jellyfish envenomation Overview mixture of toxic and/or antigenic polypeptides and enzymes systemic or local reactions to venoms by humans envenomation on contact with jellyfish tentacle – release of venom coated tubule from nematocysts on tentacle suspect envenomation in o unexplained collapse in surf o diving accidents and o near drowning only available antivenom is for box jellyfish Local reactions most common; results in linear urticarial and painful eruptions kinin like substances in venom may release exogenous and endogenous mediators lesions of variable duration and may be vesicular, hemorrhagic, necrotizing or ulcerative localized sweating, lymphadenopathy, subsequent fat atrophy, vasospasm, limb necrosis, gangrene and contracture may develop – toxic reactions exaggerated reactions may last weeks with recurrent reactions or delayed persistent reactions up to months may occur contact dermatitis and urticaria Chronic or long term reactions keloids hyperpigmentation fat atrophy scarring vasospasm mononeuritis autonomic nerve paralysis ataxia Systemic reactions malaise, weakness local cramping and muscle spasm ataxia and paraesthesia fever, nausea and vomiting toxic reactions to venom Box-jellyfish Chironex fleckeri – most venomous sea creature and can cause death within 30 seconds Most stings are not life-threatening Found mainly off the coast of north Queensland and far west up to Darwin Venom Toxins not yet characterized Cardiac, skeletal and smooth muscle conduction pathways ± central neurological pathways affected Cardiotoxicity major concern – impaired cardiac contraction, hypertension then hypotension, arrhythmias and decreased coronary flow Assessment Sting intensely painful – victim screaming and irrational Toxic skin reaction – wheals, vesicles and red-brown whip like marks Hypertension and tachycardia Muscle spasms and paralysis Management Retrieve from water and call for help ABC – oxygen, CPR as indicated Immediately apply vinegar liberally over affected area to paralyze nematocysts and worsening of envenomation First aid o Protect yourself, do not touch stingers without gloves o Consider compression bandage in extensive limb stings – controversial o Dried nematocysts may reactivate with water so do not wash them If unconscious or life threatening envenomation – o Minimum 1 vial antivenom diluted 1 in 10 crystalloid as IV push up to 3 vials o Magnesium sulphate 0.2mmol/kg up to 10mmol as bolus over 5-10 minutes o Continue CPR until further antivenom available and o Repeat Mg and cardioactive drugs as needed Analgesia o Icepacks o Narcotic analgesia o MgSO4 and antivenom in lower doses than above for symptom relief – titrate to response