Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
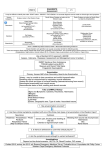
Snake Bite Management Dr Morné Strydom Department of Pharmacology University of Pretoria Who are the main culprits? Stiletto Snake • Most common dangerous bite in SA • Cytotoxic venom & Sarafotoxin • NOT INCLUDED in Polyvalent Antivenom Mozambique Spitting Cobra • Aggressive, bite without being provoked. • Cytotoxic venom • INCLUDED in Polyvalent Antivenom Puff Adder • Well camouflaged, may strike very rapid! • Cytotoxic venom • INCLUDED in Polyvalent Antivenom Snouted Cobra • Neurotoxic Venom • INCLUDED in Polyvalent Antivenom Stiletto Snake SAVP POLYVALENT ANTIVENOM 1 X Rinkhals • Rinkhals 2 X Adders • Puff Adder • Gaboon Adder 3 X Mambas • Black Mamba • Green Mamba • Jameson’s Mamba 4 X Cobras • Snouted Cobra • Forest Cobra • Mozambique Spitting Cobra • Cape Cobra Rinkhals Puff Adder Gaboon Adder Black Mamba Green Mamba Jameson’s Mamba Snouted Cobra Forest Cobra Cape Cobra Mozambique Spitting Cobra SAPV MONOVALENT ANTIVENOM BOOMSLANG IMMEDIATE FIRST AID Snake Transport Patient • • • • Do not attempt to catch or kill the offending snake Bystanders must contact a snake handler. Take a digital photo of the snake from a safe distance. If snake has already been killed: • Bite reflex may remain intact for several hours, handle dead snake with a long stick. • Transport to hospital in a safe rigid container for identification. • Immediately arrange transport to a medical facility. • Alert the hospital about the arrival of a snake bite victim, so that appropriate preparations can be made. • Arrangements should me made to have the SACP Polyvalent Antivenom ready in case it is needed. • • • • • Keep patient calm and reassured. Let the patient lie down and discourage any unnecessary movements. Remove any constricting rings, bracelets or clothing from the bitten limb. Allow the bitten limb to rest at a level at or slightly lower than the victim’s heart. Wrap a large crepe bandage snugly around the bitten limb starting at the site of the bite and working proximally up the full length of the limb. • Secure a splint to the bandaged limb as rigid and unmoving as possible. Avoid bending or moving the limb excessively while applying the splint. IMMEDIATE FIRST AID DO NOT remove the splint or bandages until the victim has reached the hospital and is receiving Antivenom if indicated. DO NOT cut or incise the bite site DO NOT apply ice to the bite site HOSPITAL MANAGEMENT BITES BY SNAKES WITH PREDOMINANTLY CYTOTOXIC VENOM • Medical emergency and can be fatal if not treated. • Envenomation may cause severe shock, as well as haemolytic, coagulopathy, haemorrhagic, and local reactions. • Death may ensure rapidly (within hours), but more commonly occurs in 12-24 hours. • Make sure at least 12 vials of SAVP Polyvalent Antivenom are present with the patient. • If the patient has been envenomated, the treatment is at least 6 vials of IV Antivenom (to start of with). IMPORTANT INFO REGARDING THIS TYPE OF BITE IS ORGANISED INTO THE FOLLOWING SECTIONS: 1. Signs and Symptoms of Envenomation 2. Medical Management 3. Other Considerations 1. SIGNS & SYMPTOMS OF ENVENOMATION PAINFUL PROGRESSIVE SWELLING LOCAL EFFECTS: CARDIOVASCULAR: Pain and swelling: onset almost immediately Blistering Haemorrhagic oedema Tissue necrosis: onset usually days after bite Ecchymosis HAEMATOLOGICAL: Coagulation defects Spontaneous bleeding: mucosal bleeding Thrombocytopenia: onset <4hours after bite Hematemesis, Epistaxis Ecchymoses / Petechiae GIT bleeding, Internal haemorrhage Anaemia: Secondary to bleeding & haemolysis RENAL / URINARY: Pulmonary oedema, Tachypnoea, Dyspnoea Haematuria, Haemoglobinuria, Myoglobinuria, Renal failure GENERAL: PULMONARY: Severe hypotension: onset often immediately Cardiac arrhythmias: Tachycardia Prolonged QT intervals Supraventricular tachycardia Inverted T waves Bradycardia Cardiac arrest (*Gaboon viper) N/V, Fever, Abdominal pain, Regional LA FANG MARKS: 1 or 2 punctures, scratches, small lacerations, no marks! Single vs. Multiple bites NB TO NOTE! 2. MEDICAL MANAGEMENT ADMISSION Admit to a Trauma Centre PRIMARY SURVEY Establish patent airway, WORK UP adequate breathing & O2, and Circulation Begin peripheral IV infusion (16G) of NS / Ringers Type & Cross Match 2X Units of Whole Blood. Obtain FFP. FBC & Diff Count + Platelets Clotting Profile: PT, PTT, INR If in shock, give fluid UKE bolus 20ml/kg, followed LDH (with isoenzyme up at rate of 125cc/hr Children: 4:2:1 Regime analysis) Urinalysis: Free protein, Hemoglobin, Myoglobin ECG Continuous Urine Output Monitoring Vitals should be monitored frequently over the first 48 hours after the bite TETANUS Tetanus Prophylaxis should be current Antibiotics are not recommended prophylactically OBSERVATION Observe for S&S of Envenomation: 15 minutes – 2 hours after bite. If NONE S&S noted after 2 Hours, most likely a dry bite (no venom injected). SLOWLY start to remove bandages and splints watching carefully for changes in the patient’s status. If ANY changes occur, assume envenomation and prepare to give AV stat. If S&S still fails to manifest, continue CLOSE observation of the patient for an additional 12-24 hours. 2. MEDICAL MANAGEMENT Severe swelling: Immediate swelling of more than half of the affected limb Swelling that progresses past one joint in < 1 hour Severe systemic signs of envenomation such as: Swelling that progresses past two joints in < 4 hours Any swelling affecting or reaching the trunk of the body Hypotension Shock Cardiac dysrrhythmias INDICATIONS FOR ANTIVENOM THERAPY ANTIVENOM ADMINISTRATION PREPARATION The patient should be on an ECG, BP & Saturation Monitor Large bore IV access should be secured All resus equipment for airway, ventilator and circulatory management should be prepared Patients at risk for anaphylactic reactions: Patients with atopic tendencies Bronchial asthma Previous exposure to equine products Should be pre-treated with 0.3ml of S/C ADRENALINE (1:1000 Sol) (Avoid Adrenalin pre-treatment in IHD, Uncontrolled HPT, and Arrythmias) All drugs should be ready for the treatment of anaphylaxis ADRENALINE 0.5ml (1:1000 Sol) should be drawn up and available for immediate IM administration in case of severe anaphylaxis. ANTIVENOM ADMINISTRATION ADMINISTRATION Dilute the contents of 6 vials of SAVP Polyvalent Antivenom in NS / Ringers solution to a total volume of 200ml. Administer the Antivenom IV over 30 minutes at a rate of 400ml/hour. Should any signs of ALLERGY / ANAPHYLAXIS develop, immediately discontinue the administration of the antivenom, and treat symptoms with ADRENALIN, CORTICOSTEROIDS, and ANTIHISTAMINES. As soon as the patient is stabilized, continue the antivenom infusion at a slower rate (100-200ml/hour). After 15 minutes of Antivenom administration, the splint and bandages may be removed – VERY SLOWLY over a period of 10 minutes to prevent a bolus release of venom. If patient’s condition worsens, reapply the crepe bandage, wait 10 minutes and release the bandage again slowly over 10 minutes while antivenom infusion is continuing. Antivenom Therapy is the mainstay of treatment of serious snake envenomation. Many of the symptoms are ameliorated or entirely eliminated by the antivenom alone. Other symptoms will require additional therapeutic modalities in order to be corrected. Additional Therapeutic Modalities: CARDIOVASCULAR STATUS: Gaboon Viper venom known to be cardiotoxic: causes arrhythmias & hypotension Cardiac arrhythmias, specifically prolonged QT intervals, inverted T waves, and SV Tachycardia my persist for days after the initial envenomation. Supportive Rx is indicated. Severe bradycardia may require a Temporary Pacemaker to ensure cardiac output and to prevent cardiac arrest. Additional Therapeutic Modalities: HEMATOLOGICAL SIGNS & SYMPTOMS: Gaboon Viper venom has a thrombin-like enzyme: quickly depletes serum fibrin levels – rendering the blood incoagulable. In addition, is has hemorrhagic activity, causes widespread damage to the microvasculature (lungs & GIT very sensitive). Puff Adder venom: Both Pro- and Anticoagulation activity. May show a variety of responses. Victims frequently develop thrombocytopenia, ↓Fibrinogen levels, spontaneous bleeding, DIC, and anaemia. Death = Internal haemorrhage & Circulatory Shock. Rx: Whole blood, Packed RBC’s, Platelets, Cryoprecipitate, FFP = Should be given when indicated! Additional Therapeutic Modalities: RENAL: The haemorrhagic activity of the venom may result in haematuria. In addition, haemoglobinuria & myoglobinuria may likewise affect renal function, and if severe (ARF), may necessitate peritoneal dialysis. KEEP VENOM NEUTRALIZATION CURRENT AND CONTINUOUS • Monitor patient’s status • If present condition does not improve, or worsen, additional antivenom should be administrated! • Give all additional antivenom in one vial increments. • Dilute antivenom as before and administer it IV over ± 15 minutes. BITES WITH ENVENOMATION REQUIRE AT LEAST 6 VIALS, BUT SEVERE ENVENOMATIONS MAY REQUIRE UP TO 12 VIALS OF ANTIVENOM OR EVEN MORE. • Patient should be observed in hospital for at least 24 hours after all symptoms abate. 3. OTHER CONSIDERATIONS PSEUDO-COMPARTMENT SYNDROME: • True fascial compartment syndromes in these bites are uncommon. • Limbs may swell significantly, but rarely involve specific fascial bound compartments. • If the bite raise a high index of suspicion for CS, monitoring with a Stryker needle or appropriate pressure device may be necessary. Fasciotomy is rarely, if ever, recommended in these patients. HOSPITAL MANAGEMENT BITES BY SNAKES WITH PREDOMINANTLY NEUROTIXIC VENOM • Bites by Mambas and Non-spitting Cobras • Leading to progressive weakness • A bite from one of these snakes with systemic envenomation can me rapidly fatal: Death in 30 – 120 minutes if untreated Progressive Weakness: Neurologic deterioration Drowsiness, neurological and neuromuscular weakness may develop early Paralysis Ventilatory failure leading to respiratory arrest Death (if not treated) TAKE THE FOLLOWING ACTIONS 1. Be prepared to provide respiratory support 2. Advanced airway management (intubation with mechanical ventilation) may be needed in severe cases 3. DO NOT remove crepe bandages & splints until patient is receiving antivenom, if indicated. 4. Make sure that no less than 8 vials of SAVP Polyvalent Antivenom are available for initial treatment of the patient. 5. Treatment of neurotoxic bites from snakes such as Black Mamba and Cape Cobra may require as many as 20 vials of Antivenom. ENVENOMATION IS DX BY THE PRESENCE OF CHARACTERISTIC SIGNS & SYMPTOMS IMPORTANT INFO IS GIVEN UNDER THE FOLLOWING HEADINGS: 1. Signs and Symptoms of Envenomation 2. Medical Management 3. Other Considerations 1. SIGNS & SYMPTOMS OF ENVENOMATION NEUROLOGICAL & NEUROMUSCULAR: Progressive weakness of skeletal muscles, including respiratory muscles. Usually, these symptoms manifest early. BE ON THE LOOKOUT FOR THE FOLLOWING: Respiratory paralysis or Dyspnoea Excessive salivation Drowsiness Restlessness Sudden LOC Ptosis Ophthalmoplegia Paresthesias Palatal paralysis Dysphasia Vertigo Fasciculations Limb paralysis Ataxia Head drooping Headache Incontinence Hyporefelxia or Areflexia Local pain or Numbness at bite site GENERAL: Onset of these symptoms manifest within 15 minutes to 4 hours following envenomation: Shock Hypotension Abdominal pain Nausea & Vomiting Regional LA Fever Epistaxis Flushing of the face Warm skin Increased sweating Pallor NEPHROTOXICITY: Acute renal failure has been recorded in a few cases of neurotoxic bites. Oliguria / Anuria, dialysis is advised. CARDIOTOXICITY: Changes in CVS status result primarily from the effects of Circulatory Collapse & Shock, as well as… Vagal blockade resulting in Tachydysrrhythmias. LOCAL SYMPTOMS: Local tissue damage may range from minor severity to moderate necrosis and swelling around the area of the bite site. FANG MARKS: Fang marks of these snakes are small. May be present as 1 or 2 well defined punctures, or there may not be any noticeable or obvious markings where the bite occurred. Single vs. Multiple bites (must be noted!) Probability of dry bites = small, especially in Black Mambas. 2. MEDICAL MANAGEMENT ADMISSION Admit to a Trauma Centre PRIMARY SURVEY Establish patent airway, WORK UP adequate breathing & O2, and Circulation Type & Cross Match 2X If in respiratory distress, Units of Whole Blood. perform BM-Ventilation Obtain FFP. without delay. Consider FBC & Diff Count + intubation with Platelets mechanical ventilation. Clotting Profile: PT, PTT, Begin peripheral IV infusion (16G) of NS / Ringers INR UKE LDH (with isoenzyme analysis) Urinalysis: Free protein, If in shock, give fluid bolus 20ml/kg, followed Hemoglobin, Myoglobin up at rate of 125cc/hr ECG Children: 4:2:1 Regime Continuous Urine Output Monitoring Vitals should be monitored frequently over the first 48 hours after the bite TETANUS Tetanus Prophylaxis should be current Antibiotics are not recommended prophylactically OBSERVATION Observe for S&S of Envenomation: 15 minutes – 2 hours after bite. If NONE S&S noted after 2 Hours, most likely a dry bite (no venom injected). SLOWLY start to remove bandages and splints watching carefully for changes in the patient’s status. If ANY changes occur, assume envenomation and prepare to give AV stat. If S&S still fails to manifest, continue CLOSE observation of the patient for an additional 12-24 hours. 2. MEDICAL MANAGEMENT Respiratory compromise Declining Saturation levels or ABG Levels Progressive muscle paralysis INDICATIONS FOR ANTIVENOM THERAPY Difficulty in swallowing leading to salivation Declining respiratory effort Ptosis, covering more than one third of the eye ANTIVENOM ADMINISTRATION PREPARATION The patient should be on an ECG, BP & Saturation Monitor Large bore IV access should be secured All resus equipment for airway, ventilator and circulatory management should be prepared Patients at risk for anaphylactic reactions: Patients with atopic tendencies Bronchial asthma Previous exposure to equine products Should be pre-treated with 0.3ml of S/C ADRENALINE (1:1000 Sol) (Avoid Adrenalin pre-treatment in IHD, Uncontrolled HPT, and Arrythmias) All drugs should be ready for the treatment of anaphylaxis ADRENALINE 0.5ml (1:1000 Sol) should be drawn up and available for immediate IM administration in case of severe anaphylaxis. ANTIVENOM ADMINISTRATION ADMINISTRATION Dilute the contents of 8-10 vials of SAVP Polyvalent Antivenom in NS / Ringers solution to a total volume of 200ml. Administer the Antivenom IV over 30 minutes at a rate of 400ml/hour. Should any signs of ALLERGY / ANAPHYLAXIS develop, immediately discontinue the administration of the antivenom, and treat symptoms with ADRENALIN, CORTICOSTEROIDS, and ANTIHISTAMINES. As soon as the patient is stabilized, continue the antivenom infusion at a slower rate (100-200ml/hour). After 15 minutes of Antivenom administration, the splint and bandages may be removed – VERY SLOWLY over a period of 10 minutes to prevent a bolus release of venom. If patient’s condition worsens, reapply the crepe bandage, wait 10 minutes and release the bandage again slowly over 10 minutes while antivenom infusion is continuing. Antivenom Therapy is the mainstay of treatment of Mamba and Cobra envenomation. Many of the symptoms are ameliorated or entirely eliminated by the antivenom alone. Other symptoms will require additional therapeutic modalities in order to be corrected. Local symptoms may take several days to weeks to completely resolve; their progression, however, may be controlled with antivenom therapy. Patient should be observed in hospital for at least 24 hours after all symptoms abate. ADJUCTIVE THERAPIES • If severe muscle or respiratory paralysis persists, or antivenom is not immediately available, consider: • Atropine 0.5mg I.V., followed with • Neostigmine 1mg I.V. every 30 minutes for a maximum of 5 doses 3. OTHER CONSIDERATIONS • Berg Adder bites can present with a neurotoxic progressive weakness syndrome. Don’t give Antivenom for Berg Adder bites, it will not neutralize the venom. Rx: Supportive care in Highcare / ICU Setting. • Morphine is CONTRAINDICATED due to its respiratory suppression properties. Alcohol should also be avoided. 3. OTHER CONSIDERATIONS MULTIPLE BITES: • Mambas & Cobras are prone to deliver multiple bites = INJECT A LARGER VOLUME VENOM • INITIAL dose = 12 Vials (Diluted to 200ml), infusion over 30 minutes under direct medical supervision. • WATCH CLOSELY for signs of allergic response. CLINICAL CONSIDERATIONS WITH NEUROTOXIC SNAKE BITES • Prompt administration of Antivenom has resulted in remarkably rapid recovery in many cases. • Delay in administration or insufficient dosages of antivenom may allow serious neurological symptoms and respiratory paralysis to manifest, which may be very difficult to reverse once established and clinical envenomation is often fatal. CLINICAL CONSIDERATIONS WITH NEUROTOXIC SNAKE BITES • Cape Cobras = Rapid onset in respiratory paralysis, and difficult to reverse once established even with large amounts of antivenom. • Since both antivenom & neostigmine may fail to reverse fully established paralysis, it is suggested that the toxin become fixed to a presynaptic target, is unavailable to bind with the antivenom, and that reversal occurs only after metabolic degradation has taken place. • Long-term intubation & ventilation as long as 7-8 days or more has been necessary in a number of cases. • Early administration of antivenom before the onset of respiratory impairment may allow for sufficient binding of the neurotoxic componants, and avoid the need for mechanical ventilation. • Modderfontein Road Sandringham Johannesburg South Africa (GPS co-ordinates: S26°07.892 E028°07.106) P.O Box 28999, Sandringham 2131 Johannesburg, South Africa After hours emergency Tel: +27(11) 386-6000 Business hours Tel: +27(11) 386-6063/2 • SAVP e - mail Fax: (011) 386-6016 References: 1. Marsh, N.A., Whaler, B.C., The Gaboon Viper (Bitis gabonica): its biology, venom components and toxinology, Toxicon 22, 669694, 1984. 2. Warrell, D.A., Ormerod, L.D., Davidson, N. NcD., Bites by Puff-Adder (Bites arietans) in Nigeria, and value of antivenom, British Medical Journal, 1975, 4:697. 3. Mebs, D., Pohlman, S., Von Tenspolde, W., Snake venom hemorrhagins: neutralization by commerical antivenoms, Toxicon, 1988, 26:453. 4. Brink, S., Steytler, J.G., Effects of Puff-Adder venom on coagulation, fibrinolysis and Platelet aggregation in the baboon, South African Medical Journal, 1974, 48:1205. 5. Homma, H., Tu, A.T., Morphology of local tissue damage in experimental snake envenomation, British Journal of Experimental Pathology, 1971, 52:538. 6. WARRELL, D.A., GREENWOOD, B.M., DAVIDSON, N.M., OMEROD, L.D., PRENTICE, C.R.M.: Necrosis, haemorrhage and Complement Depletion Following Bites by the Spitting Cobra (Naja nigricollis). Quart. J. Med., n.s., 45(177:1, 1976. 7. STROVER, H.M.: Observations on Two Cases of Snake-bite by Naja nigricollis ss mossambica. Cent. Afr. J. Med., 19(1):12, 1973. 8. South African Institute for Medical Research: Anti-Snakebite Serum. (Package Insert with Antivenom), 1980. 9. SAUNDERS, C.R.: Report on a Black Mamba Bite of a Medical Colleague. Cent. Afr. J. Med., 26:121, 1980. 10. BLAYLOCK, R.S.: (to the editor) Black Mamba Envenomation. S. Afr. Med. J., 68:293, 1985. 11. BLAYLOCK, R.S., LICHTMAN, A.R., POTGIETER, P.D.: Clinical Manifestations of Cape Cobra (Naja nivea) Bites. S. Afr. J. Med., 68:342, 1985. 12. CRISP, N.G.: (to the editor) Black Mamba Envenomation. S. Afr. Med. J., 68:293, 1985.