Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
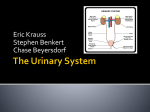
Chapter 45 Urinary Elimination Scientific Knowledge Base: Organs of Urinary Elimination Kidneys Ureters Remove waste from the blood to form urine Transport urine from the kidneys to the bladder Bladder Urethra Reservoir for urine until the urge to urinate develops Urine travels from the bladder and exits through the urethral meatus. Urinary System Urinary System Organs Renal Nephron Additional Kidney Functions Production of erythropoietin is essential to maintaining a normal red blood cell (RBC) volume. Erythropoietin stimulates bone marrow to produce RBCs and prolongs the life of mature RBCs. Production of renin, prostaglandin E2, and prostacyclin affects blood pressure. Renin starts a chain of events that cause water retention, thereby increasing blood volume. Prostaglandin E2 and prostacyclin aid vasodilation. Kidneys affect calcium and phosphate regulation Act of Urination Brain structures influence bladder function. Voiding: Bladder contraction + Urethral sphincter and pelvic floor muscle relaxation 1. Stretching of bladder wall signals the micturition center in the sacral spinal cord. 2. Impulses from the micturition center in the brain respond to or ignore this urge, thus making urination under voluntary control. 3. When a person is ready to void, the external sphincter relaxes, the micturition reflex stimulates the detrusor muscle to contract, and the bladder empties. Factors Influencing Urination Disease conditions Medications and medical procedures Socioeconomic factors (need for privacy) Psychological factors (anxiety, stress, privacy) Fluid balance Nocturia, polyuria, oliguria, anuria Diuresis Fever Disease Conditions Affecting Urination Prerenal, renal, postrenal classification Conditions of the lower urinary tract Diabetes mellitus and neuromuscular diseases such as multiple sclerosis Benign prostatic hyperplasia Cognitive impairments (e.g., Alzheimer’s) Diseases that slow or hinder physical activity Conditions that make it difficult to reach and use toilet facilities End-stage renal disease, uremic syndrome Medical Interventions Affecting Urination Surgical procedures Restriction of fluid intake lowers urine output. Stress causes fluid retention. Medications Some cause urinary retention and/or overflow incontinence. Some cause urgency and incontinence. Some change the color of urine. Diagnostic examinations Restriction of fluid intake lowers urine output. Direct visualization causes localized trauma and edema; patients may have difficulty voiding. Dialysis Renal Replacement Two methods Peritoneal Hemodialysis 10 Indications for Dialysis Renal failure that can no longer be controlled by conservative management (Conservative management would include dietary modifications and the administration of medications to correct electrolyte abnormalities.) Worsening of uremic syndrome associated with ESRD, which would include nausea, vomiting, neurological changes, and pericarditis) Severe electrolyte and/or fluid abnormalities that cannot be controlled by simpler measures (These abnormalities would include hyperkalemia and pulmonary edema.) by simpler measures Case Study Mrs. Vallero is a 65-year-old woman who has been in the hospital for 4 days with problems related to heart failure, fluid retention, and diabetes. She has a history of urinary retention secondary to neuropathy caused by her diabetes. Mrs. Vallero’s indwelling urinary catheter was removed 2 days ago and subsequently was replaced yesterday at 6 AM because of her inability to urinate more than 100 mL at a time, being incontinent of small amounts of urine, complaints of urinary urgency, and lower abdominal pain. Case Study (cont’d) Sandy notes that the urinary catheter was removed at 7 AM this morning, and the patient has no recorded urine output for the day. Mrs. Vallero verifies that she has only “dribbled” urine. While making rounds, Sandy talks with Mrs. Vallero, who says she is worried because “I thought this was all under control.” The health care provider is notified, and an order is obtained for an intermittent catheterization. The registered nurse on the day shift catheterizes Mrs. Vallero at 3 PM with a return of 600 mL of pale, clear yellow urine. Case Study (cont’d) As Sandy prepares to assess Mrs. Vallero again, she remembers that urinary problems are common in patients who have diabetes and in older adults. Age alone does not cause incontinence. She recalls that patients with urinary retention sometimes leak or “dribble” urine and are then misdiagnosed as incontinent. She knows that patients generally void at least every 6 to 8 hours, and that Mrs. Vallero’s recent catheterization, her decreased mobility, and her history of diabetes make her more prone to urinary retention, incontinence of small amounts of urine, and urinary tract infection (UTI). Alterations in Urinary Elimination Urinary retention Urinary tract infection An accumulation of urine due to the inability of the bladder to empty Results from catheterization or procedure Urinary incontinence Urinary diversion Involuntary leakage of urine Diversion of urine to external source Types of Urinary Diversions Urinary Diversion 17 Nursing Knowledge Base & Assessment Infection control and hygiene Growth and development Muscle tone Psychosocial considerations Cultural considerations Urine Collection in Children Specimen collection from infants and children is often difficult. Adolescents and school-aged children usually are able to cooperate. Preschool children and toddlers have difficulty voiding on request. Physical Assessment Gather nursing history for the patient’s urination pattern and symptoms, and factors affecting urination. Conduct physical assessment of the patient’s body systems potentially affected by urinary change. Assess characteristics of urine. Assess the patient’s perception of urinary problems as it affects self-concept and sexuality. Gather relevant laboratory and diagnostic test data. Physical Assessment Skin and mucosal membranes Kidneys Assess hydration. Flank pain may occur with infection or inflammation. Bladder Urethral meatus Distended bladder rises above symphysis pubis. Observe for discharge, inflammation, and lesions. Assessment of Urine Intake and output Characteristics of urine Color Pale-straw to amber color Clarity Transparent unless pathology is present Odor Ammonia in nature Urine testing Specimen collection Urine Tests and Diagnostic Examinations Urinalysis Specific gravity Culture Noninvasive procedures Invasive procedures Case Study (cont’d) Sandy knows that she will need to assess whether Mrs. Vallero feels the urge to urinate. She determines that no one has taken Mrs. Vallero to the bathroom recently. Sandy also needs to find out more about her patient’s urination patterns at home because Mrs. Vallero has verbalized anxiety about her present voiding patterns. Previous clinical experience has taught Sandy that palpation of the abdomen over a distended bladder causes some discomfort, and that the patient often experiences an urge to urinate. Mrs. Vallero grimaces when her abdomen is palpated and says she has a little pain. Restorative Care Strengthening pelvic floor muscles Bladder retraining Habit training Self-catheterization Maintenance of skin integrity Promotion of comfort Evaluation Evaluate whether the patient has met outcomes and goals. Check how the patient reports progress made. Help the patient redefine goals if necessary. Revise nursing interventions as indicated. Case Study (cont’d) Sandy talks with Mrs. Vallero the next evening. The patient’s care plan incorporates scheduled voiding, oral fluids, and use of Credé’s method of manual compression during voiding. She palpates Mrs.Vallero’s bladder and then assists her to the toilet. After making sure she is comfortable and leaving the call light in place, Sandy instructs her to use Credé’s method of manual compression. She returns to measure Mrs. Vallero’s urinary output and evaluates for bladder residual using an ultrasound bladder scan. Case Study (cont’d) Ask Mrs. Vallero about her urge to void, sensation of bladder fullness, and dribbling episodes. Have Mrs. Vallero keep a log of her pattern of elimination, including urine output volumes with each voiding, during the 1-month period. Ask Mrs. Vallero if she continues to have lower abdominal pain. Case Study (cont’d) Mrs. Vallero is concerned about regaining her urinary function. Sandy develops the following outcome for her: At the end of the teaching session, Mrs. Vallero will be able to describe approaches to promote normal urinary elimination habits. What teaching strategies would you put into the plan? What evaluation strategies would you use?