Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
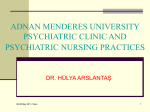
ULTRASOUND ARTICLE Pectoral Nerves I and II Blocks in Multimodal Analgesia for Breast Cancer Surgery A Randomized Clinical Trial Ghada Mohammad Nabih Bashandy, MD, and Dina Nabil Abbas, MD Background: The pectoral nerves (Pecs) block types I and II are novel techniques to block the pectoral, intercostobrachial, third to sixth intercostals, and the long thoracic nerves. They may provide good analgesia during and after breast surgery. Our study aimed to compare prospectively the quality of analgesia after modified radical mastectomy surgery using general anesthesia and Pecs blocks versus general anesthesia alone. Methods: One hundred twenty adult female patients scheduled for elective unilateral modified radical mastectomy under general anesthesia were randomly allocated to receive either general anesthesia plus Pecs block (Pecs group, n = 60) or general anesthesia alone (control group, n = 60). Results: Statistically significant lower visual analog scale pain scores were observed in the Pecs group than in the control group patients. Moreover, postoperative morphine consumption in the Pecs group was lower in the first 12 hours after surgery than in the control group. In addition, statistically significant lower intraoperative fentanyl consumption was observed in the Pecs group than in the control group. In the postanesthesia care unit, nausea and vomiting as well as sedation scores were lower in the Pecs group compared with the control group. Overall, postanesthesia care unit and hospital stays were shorter in the Pecs group than in the control group. Conclusions: The combined Pecs I and II block is a simple, easy-to-learn technique that produces good analgesia for radical breast surgery. (Reg Anesth Pain Med 2015;40: 68–74) B reast cancer is the most common cancer among women. In the United States, 1 in 8 women develop breast cancer during their lifetime.1,2 In Gharbiah, Egypt, increased breast cancer rates have been recorded from 1999 to 2008. According to a recent epidemiologic study, higher breast cancer rates were expected between 2009 and 2015.3 Acute postoperative pain is an integral risk factor in the development of chronic postmastectomy pain; 40% of women will have severe acute postoperative pain after breast cancer surgery, whereas 50% will develop chronic postmastectomy pain with impaired quality of life.4,5 Regional anesthesia techniques have provided better-quality acute-pain control and subsequently less chronic pain.5,6 Proposed mechanisms for decreased persistent pain include decreased central sensitization (wind-up) and lower incidence of opioid-induced hyperalgesia.7,8 Furthermore, effective acute pain control preserves immune From the Department of Anesthesia and Pain Management, National Cancer Institute, Cairo University, Cairo, Egypt. Accepted for publication August 20, 2014. Address correspondence to: Ghada Mohammad Nabih Bashandy, MD, National Cancer Institute, Cairo University, Fom Al-Khalij, KasrAleiny St, Cairo, Egypt (e‐mail: [email protected]). Funding from the National Cancer Institute, Cairo University, helped support this work. The work was presented as a poster at the WIP 2014 Congress at Maastricht, the Netherlands, May 7 to 10, 2014. The authors declare no conflict of interest. Copyright © 2014 by American Society of Regional Anesthesia and Pain Medicine ISSN: 1098-7339 DOI: 10.1097/AAP.0000000000000163 68 function, both by suppressing the surgical stress response and by decreasing the need for general anesthetics and opioids. Opioids, especially morphine, inhibit both cellular and humoral immune functions.9 This effect may be responsible for the higher rates of postsurgical local recurrence and/or metastasis.10 Thoracic epidural block, thoracic paravertebral block (TPVB), interpleural block, intercostal nerve block, interscalene block, and wound infiltration have all been used in anesthesia and/or analgesia in breast cancer surgery.11–16 Thoracic paravertebral block has been shown to provide superior analgesia, and there is some evidence suggesting decreased cancer recurrence rates with the use of TPVB.17,18 Nonetheless, not all anesthesiologists feel comfortable using such invasive techniques in breast cancer surgery. The pectoral nerve (Pecs) block, a less invasive novel technique described by Blanco et al,19,20 is an interfascial plane block where local anesthetic is deposited into the plane between the pectoralis major muscle (PMm) and the pectoralis minor muscle (Pmm) (Pecs I block) and above the serratus anterior muscle at the third rib (Pecs II block). These novel techniques attempt to block the pectoral; intercostobrachial; intercostals III, IV, V, VI; and long thoracic nerves.19,20 Our study prospectively compares Pecs blocks in combination with general anesthesia and general anesthesia alone in modified radical mastectomy (MRM) surgery. We hypothesized that the Pecs blocks would provide superior postoperative analgesia for patients undergoing mastectomy as compared with a control group. Our primary outcome measure was visual analog scale (VAS) pain scores on the first postoperative day in patients who have preoperative Pecs block compared with those having general anesthesia alone. Secondary measures were perioperative opioid consumption, postoperative sedation, and postoperative nausea and vomiting (PONV). METHODS After obtaining approval from Egypt’s National Cancer Institute Institutional Review Board, we conducted this prospective randomized observer-blinded study from January 2013 to January 2014 in the National Cancer Institute of Egypt. A continuous sample of 120 American Society of Anesthesiologists (ASA) physical status I and II female adult patients undergoing elective unilateral MRM under general anesthesia were recruited Written informed consent was obtained. Exclusion criteria included declining to give written informed consent, history of allergy to the medications used in the study, contraindications to regional anesthesia (including coagulopathy and local infection), prior breast surgery except for diagnostic biopsies, and history of treatment for a chronic pain condition and/or psychiatric disorder. All patients included in the study were randomly assigned to 1 of the 2 groups: the Pecs group receiving Pecs blocks and general anesthesia (n = 60) and a control group receiving general anesthesia alone (n = 60). Group allocation was accomplished using a predetermined random 1:1 sequence. All the recruited patients were familiarized with VAS pain scoring and patient-controlled analgesia (PCA). Regional Anesthesia and Pain Medicine • Volume 40, Number 1, January-February 2015 Copyright © 2014 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited. Regional Anesthesia and Pain Medicine • Volume 40, Number 1, January-February 2015 Preoperative Management All patients were premedicated with 10 mg of oral diazepam on the night of surgery. In the preoperative holding area, patients were attached to standard ASA monitors, and intravenous (IV) access was obtained. Premedication with IV 1 to 2 mg of midazolam and 10 mg of metoclopramide was administered to all patients. The patients in the control group were then transferred immediately to the operating room, whereas the patients in the Pecs group received an ultrasound-guided Pecs block and a 15-minute observation time prior to their transfer to the operating room. One investigator (G.M.N.B) did all the blocks for patients in the Pecs group. Anesthesia management and data collection were performed by personnel blinded to the treatment group. A broadband (5–12 MHz) linear array probe of eZono 3000 portable ultrasound system (eZono USA, Redmond, Washington) was used, with an imaging depth of 4 to 6 cm. After cleaning the infraclavicular and axillary regions with chlorhexidine, the probe was placed below the lateral third of the clavicle, similar to what is done when performing infraclavicular brachial plexus block (Fig. 1). After recognition of the appropriate anatomical structures, the skin puncture point was infiltrated with 2% lignocaine, then the block was performed by using a 20-gauge Tuohy needle. The needle was advanced to the tissue plane between the PMm and Pmm at the vicinity of the pectoral branch of the acromiothoracic artery, and 10 mL of 0.25% bupivacaine was deposited (Figs. 2, 3, and 4). In a similar manner, 20 mL was deposited at the level of the third rib above the serratus anterior muscle with the intent of spreading injectate to the axilla (Fig. 5).19,20 Intraoperative Management Standard ASA monitors were attached to the patients. General anesthesia was induced with fentanyl 1 to 2 μg/kg, propofol 2 mg/kg, and cisatracurium 0.15 mg/kg, and the airway was secured by endotracheal intubation. Anesthesia maintenance consisted of 1 MAC of isoflurane in 50% oxygen and air with additional cisatracurium at the discretion of the anesthetist. Additional boluses of fentanyl were administered to maintain blood Pectoral Nerve Blocks for Breast Surgery pressure and/or heart rate values within or 20% lower than the baseline values. Toward the completion of the surgery, paracetamol (Perfalgan) 1 g/100 mL IV infusion was started, and isoflurane was discontinued. Neostigmine 0.05 mg/kg with atropine 0.02 mg/kg was administered IV for neuromuscular blockade reversal as clinically relevant. After responding to verbal command, patients were extubated in the operating room then transferred to the postanesthesia care unit (PACU). Postoperative Management In the PACU, patients were monitored with standard ASA monitors. They were monitored for pain intensity using VAS pain score, degree of sedation using the Ramsay sedation scale,21 and incidence of PONV using a 5-point scale (0–4), where 0 = no nausea or vomiting, 1 = mild nausea, 2 = severe nausea, 3 = vomiting once, and 4 = vomiting more than once. When the reported VAS score was 3 or greater, a loading dose of 5 mg of morphine was administered through slow IV route. Then, a PCA was administered. The PCA pump (Graseby 3300 Pump; Smith Medical International, Ashford, Kent, UK) was loaded with 1 mg/mL of morphine and set to deliver on demand bolus doses of 1 to 2 mL based on body weight with a 5minute lockout period. No background infusion was allowed. Oral paracetamol (1 g) and ketoprofen (100 mg), to be administered 3 times daily, were prescribed to all patients as soon as oral feeding was permitted. Ondansetron 8 mg IV was used to treat nausea and vomiting. Patients with a score of 10 in the modified Aldrete scoring system were considered eligible for discharge to the surgical ward.22 Patients were discharged from the hospital based on the protocols of the surgical team, which included a pain score of less than 3 without morphine and PONV and sedation scores of 0. The following data were collected: intraoperative fentanyl consumption; postoperative VAS pain scores (at 0, 3, 6, 9, and 24 postoperative hours); need for PCA morphine; time to PCA administration as well as morphine requirements at 0 to 4, 4 to 12, and 12 to 24 postoperative hours; PONV scores; sedation scores; PACU stay; and postsurgical hospital stay. FIGURE 1. Image of the probe position and needle direction from medial to lateral during Pecs I block.30 © 2014 American Society of Regional Anesthesia and Pain Medicine 69 Copyright © 2014 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited. Bashandy et al Regional Anesthesia and Pain Medicine • Volume 40, Number 1, January-February 2015 FIGURE 2. Pecs I block ultrasound view. ax.a Indicates axillary artery; p., pectoral branch of thoracoacromial artery. Statistical Analysis All data analyses were carried out according to a preestablished analysis plan. Altman’s nomogram was used for simple size measurement. We believed that the distinction in VAS pain scores would be significant if there was at least 1 point of difference between patients who received Pecs block as preemptive analgesia before mastectomy versus the control group (variability estimated from an interim analysis; SD, 1.8). Thus, assuming α = 0.05 and the power of the study at 0.80, a total sample size of 100 patients would be required (50 in each group). To compensate for patients who dropped out, we had planned to enroll 120 patients. The normality of distribution of the initial data was assessed using Kolmogorov-Smirnov and Shapiro-Wilk W tests. The data that followed a normal distribution pattern were analyzed using t test for equality of means. Equality of variances was estimated using Levene test. The data that did not follow the normal distribution were analyzed using the nonparametric Mann-Whitney U test. The Pearson goodness-of-fit χ2 test was used to analyze associations between independent variables. P < 0.05 was set as the cutoff point for significance. Statistical analyses were performed using SPSS version 13.0 (SPSS Inc, Chicago, Illinois) and Statistica version 8.0 (StatSoft Inc, Tulsa, Oklahoma). RESULTS Patient demographics and duration of surgery for both groups were comparable (Table 1). Statistically significantly lower VAS pain scores were observed in the Pecs group compared with the control group in all test time periods (Fig. 6). In comparing FIGURE 3. Ultrasound image of needle tip at the plane of Pecs I block between the 2 pectoral muscles (arrows indicate the needle). 70 © 2014 American Society of Regional Anesthesia and Pain Medicine Copyright © 2014 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited. Regional Anesthesia and Pain Medicine • Volume 40, Number 1, January-February 2015 Pectoral Nerve Blocks for Breast Surgery FIGURE 4. Local anesthetic spread between the 2 pectoral muscles. The arrow is pointing to the needle. LA indicates local anesthetic. perioperative opioid needs, the intraoperative fentanyl requirements were found to be lower in the Pecs group than in the control group (115 ± 28.56 μg and 252.5 ± 44.352 μg, respectively, with P < 0.001). In addition, the total amount of postoperative morphine needed to keep VAS pain scores less than 3 was 2.9 ± 1.714 mg and 6.9 ± 1.861 mg in the Pecs and control groups, respectively, and the difference was found to be statistically significant (P < 0.001). The patients in the Pecs group used less morphine in the first 12 hours postoperatively than did the control group patients, but the morphine needs of the 2 groups were comparable in the succeeding 12 hours (Table 2). Only 12 of 60 patients in the Pecs group required morphine PCA based on the protocol of the study, where an adequate VAS pain score of less than 3 was maintained only by paracetamol and nonsteroidal anti-inflammatory drug that were given to all patients in our study. Conversely, 36 of 60 patients in the control group required PCA morphine administration. Postanesthesia care unit stay was statistically shorter in the Pecs group than in the control group (14 ± 11 minutes and 28 ± 12 minutes, respectively, where P = 0.012). This finding may be explained in part by lower VAS pain scores in the Pecs group, as well as lower PONV scores (0.15 ± .366 vs 1.65 ± 0.875, with P < 0.001). The reported lower sedation scores in the Pecs group compared with those in the control group are an alternative explanation of shorter PACU stay in the Pecs group (2.10 ± 0.308 vs 3.20 ± 0.523, respectively, with P < 0.001). Postsurgical hospital stay was shorter in the Pecs group than that in the control group (P < 0.001). All patients in the Pecs group were discharged from the hospital within 24 hours, whereas in the control group, only 12 patients left within 24 hours, 42 FIGURE 5. A, Image showing external probe position during Pecs II block.30 B, Ultrasound view of Pecs II block (r. 3 indicates 3rd rib; serr., serratus anterior muscle; white line, needle path to deposit local anesthetic above serratus anterior muscle. © 2014 American Society of Regional Anesthesia and Pain Medicine 71 Copyright © 2014 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited. Regional Anesthesia and Pain Medicine • Volume 40, Number 1, January-February 2015 Bashandy et al TABLE 1. Demographic Data Variable Age, y Weight, kg Height, cm Duration of surgery, min Pecs Group (n = 60) Control Group (n = 60) P 48.65 (10.7) 75.96 (6.3) 163 (6.8) 110 (17) 50.47 (12.1) 74.34 (5.9) 162 (7.8) 109 (19) 0.74 0.14 0.84 0.34 Values are mean (SD). P > 0.05 is statistically insignificant. patients were discharged within 48 hours, and 6 patients stayed in the hospital for more than 48 hours. DISCUSSION Lower pain scores were observed in patients undergoing MRM with preemptive Pecs I and II blocks than in the controls. Perioperative opioid use, including intraoperative fentanyl as well as postoperative morphine, was lower in the Pecs group compared with that in the control group. Our study also revealed lower opioid-related adverse effects with lower sedation and PONV scores in the Pecs group. Moreover, PACU and hospital stays were shorter in the Pecs group compared with that in the control group. To start performing the Pecs block, the neural supply of structures involved in breast surgery must be well understood. The pectoral nerves (PNs) show wide variability in their course.23 They are described in most textbooks as purely motor nerves, but it was suggested that they also transport proprioceptive and nociceptive fibers as shown in other motor nerves.24 In some patients, there might be additional innervations from the fourth intercostal nerve.25 A meta-analysis of available literature showed that the lateral PN (LPN) arises most frequently with 2 branches from the anterior divisions of the upper and middle trunks (33.8%) or as a single root from the lateral cord (23.4%). The medial PN (MPN) usually arises from the medial cord (49.3%), anterior division of the lower trunk (43.8%), or lower trunk (4.7%). The 2 PNs are usually connected by the ansa pectoralis immediately distal to the thoracoacromial artery.26 Hoffman and Elliott27 suggested blocking the PNs to reduce chronic postoperative pain or muscle spasm after mastectomy. A denervation point for PMm targeting the neurovascular bundle containing the LPN deep to the PMm was identified. This point is at distances of 2.81 ± 0.33 cm vertically from the medial third part of the clavicle and 8.12 ± 1.09 cm horizontally from the midsternal line.28 The MPN runs under the Pmm. It crosses the Pmm in 62% of the patients to reach the lower third of the PMm after piercing the 2 layers of the clavipectoral fascia. In the remaining 38%, it is located at the lateral border of the Pmm.26 Ultrasound-guided injection of 10 mL of the solution in cadavers was found to be sufficient in staining all the medial and LPN branches without any proximal extension to the cords of the brachial plexus.23 In MRM surgery, blocking the PNs alone is not enough. The anterior divisions of the intercostal nerves from T2 to T6 and the long thoracic and the thoracodorsal nerves should be blocked FIGURE 6. Visual analog scale scores in both study groups in different time points. VAS-0: first VAS after recovery from general anesthesia. VAS-3,VAS-6, VAS-9, VAS-24 are VAS at 3, 6, 9, 24 hours postoperatively, respectively. 72 © 2014 American Society of Regional Anesthesia and Pain Medicine Copyright © 2014 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited. Regional Anesthesia and Pain Medicine • Volume 40, Number 1, January-February 2015 Pectoral Nerve Blocks for Breast Surgery TABLE 2. PCA Morphine Requirements Variable Time to the first dose of morphine, min No. PCA morphine demands PCA morphine, mg 0–4 h 4–12 h 12–24 h Pecs Group (n = 60) Control Group (n = 60) P 170 (11.2) 2.5 (1.2) 130 (14.7) 4.3 (1. 8) 0.008* 0.04* 0 (0–9) 1 (0–4) 2 (0–15) 4 (2–12) 4 (0–10) 2 (0–25) 0.02* 0.035* 0.519 Values are means (SD) or median and range (Q1–Q3). 0–4 h, 4–12 h, and 12–24 h are postoperative hours where 0 is time of PACU admission. *P < 0.05. also.20 The intercostal nerves lie at the back between the pleura and the posterior intercostal membrane and run in a plane between the intercostal muscles as far as the sternum. They give off lateral branches that pierce the external intercostal and the serratus anterior muscles at the midaxillary line to give off anterior and posterior terminal branches. The lateral cutaneous branch of the second intercostal nerve does not divide in the anterior and posterior branches, and it is called the intercostobrachial nerve. The intercostal nerves also give anterior branches that cross in front of the internal mammary artery and pierce the internal intercostals muscle, the intercostal membranes, and the PMm to supply the medial aspect of the breast.20,29 The long thoracic nerve arises from C5 to C7, entering the axilla behind the brachial plexus resting on the serratus anterior muscle. The thoracodorsal nerve is a branch of the posterior cord made up of the 3 posterior divisions of the trunks of the brachial plexus. It follows the thoracodorsal artery and innervates the latissimus dorsi in the posterior wall of the axilla.20 Blanco19 first described Pecs I block in 2011 as an interfascial block to place local anesthetic into the plane between PMm and Pmm. He targeted the LPN, which is consistently located adjacent to the pectoral branch of the thoracoacromial artery between the PMm and Pmm. In addition, Blanco19 stated that a catheter can readily be placed into that interfascial plane. One year later, Blanco et al20 described a second version of the Pecs block called modified Pecs block or Pecs block type II, another approach aiming to block the axilla and the intercostal nerves that are necessary for axillary node dissection and wider excisions, respectively. In Pecs block type II, 20 mL of local anesthetic has to be deposited above the serratus anterior muscle. The local anesthetic would spread to the axilla where the long thoracic nerve and lateral branches of the intercostal nerves are found as they exit at the level of the midaxillary line.20 Pérez et al also30 described a different approach for Pecs block and reported decreased perioperative systemic analgesic requirements and improved patient satisfaction in major and minor breast surgeries. The ultrasound probe is placed below the outer third of the clavicle, after identifying 4 structures: PMm, Pmm, thoracoacromial artery, and cephalic vein; the needle is introduced in plane with the ultrasound probe from medial to lateral. They claimed that their approach stays far from the pleura and blood vessels and avoids blocking the needle path through the coracoid process.30 Pectoral nerves block was used in conjunction with TPVB in an observational study. The researchers compared TPVB and sedation with and without a Pecs block for breast augmentation surgery. Better postoperative analgesia and a lower requirement for sedation were observed in patients who received Pecs block.31 The paravertebral space communicates with the epidural space, is close to the pleural space, and contains supply arteries to the spinal cord; hence, special precautions should be adopted while performing © 2014 American Society of Regional Anesthesia and Pain Medicine TPVB. Thoracic paravertebral block often becomes an epidural block and may also result in total spinal anesthesia.32,33 The Pecs block is a combination of motor and sensory nerve blocks. One advantage of Pecs block, requiring emphasis, is that it is not associated with sympathetic block as are the TPVB and epidural blocks. On the other hand, intravascular injection into the pectoral branch of the acromiothoracic artery is another possibility that could be considered. Complications should be easily avoided with proper ultrasound training and searching for the right pattern of spread of the local anesthetic.20 Limitations One limitation of our study is that we did not have enough time to assess the quality of the block before the induction of anesthesia. Moreover, blinding the patients to the received technique by doing sham blocks to the control group would have made the results more reliable. Another limitation is that, in an attempt to minimize morphine consumption, we did not offer PCA morphine except for patients with VAS scores of less than 3 when we should have offered it to all patients upon arrival to the PACU or as soon as they are alert enough to use it. CONCLUSIONS The Pecs blocks produce excellent analgesia when combined with general anesthesia for breast surgery with axillary dissection. They are simple, easy-to-learn techniques, having easily identifiable landmarks based on good anatomical and ultrasound knowledge, making them an excellent alternative to the conventional thoracic paravertebral and neuraxial blocks for radical breast surgeries. Prospective randomized studies comparing Pecs blocks with paravertebral and neuraxial blocks are recommended. REFERENCES 1. Desantis C, Ma J, Bryan L, Jemal A. Breast cancer statistics, 2013. CA Cancer J Clin. 2014;64:52–62. 2. Tyczyński J, Bray F, Parkin D. Breast Cancer in Europe. Ispra, Italy: Eur Netw Cancer Regist Cancer Fact Sheets; Dec 2002. Available at: http:// encr.eu/images/docs/factsheets/breast-factsheets.pdf. Accessed September 2, 2014. 3. Hirko KA, Soliman AS, Hablas A, et al. Trends in breast cancer incidence rates by age and sage at diagnosis in Gharbiah, Egypt, over 10 years (1999-2008). J Cancer Epidemiol. 2013;2013:916394. 4. Poleshuck EL, Katz J, Andrus CH, et al. Risk factors for chronic pain following breast cancer surgery: a prospective study. J Pain. 2006;7: 626–634. 5. Gärtner R, Jensen M-B, Nielsen J, Ewertz M, Kroman N, Kehlet H. Prevalence of and factors associated with persistent pain following breast cancer surgery. JAMA. 2009;302:1985–1992. 73 Copyright © 2014 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited. Bashandy et al Regional Anesthesia and Pain Medicine • Volume 40, Number 1, January-February 2015 6. Sittl R, Irnich D, Lang PM. Update on preemptive analgesia: options and limits of preoperative pain therapy [in German]. Anaesthesist. 2013;62: 789–796. 7. Richebé P, Rivat C, Liu SS. Perioperative or postoperative nerve block for preventive analgesia: should we care about the timing of our regional anesthesia?. Anesth Analg. 2013;116:969–970. 8. Richebé P, Pouquet O, Jelacic S, et al. Target-controlled dosing of remifentanil during cardiac surgery reduces postoperative hyperalgesia. J Cardiothorac Vasc Anesth. 2011;25:917–925. 9. Sacerdote P, Bianchi M, Gaspani L, et al. The effects of tramadol and morphine on immune responses and pain after surgery in cancer patients. Anesth Analg. 2000;90:1411–1414. 10. Gupta K, Kshirsagar S, Chang L, et al. Morphine stimulates angiogenesis by activating proangiogenic and survival-promoting signaling and promotes breast tumor growth. Cancer Res. 2002;62:4491–4498. 11. Schnabel A, Reichl SU, Kranke P, Pogatzki-Zahn EM, Zahn PK. Efficacy and safety of paravertebral blocks in breast surgery: a meta-analysis of randomized controlled trials. Br J Anaesth. 2010;105:842–852. 12. Tahiri Y, Tran DQH, Bouteaud J, et al. General anaesthesia versus thoracic paravertebral block for breast surgery: a meta-analysis. J Plast Reconstr Aesthet Surg. 2011;64:1261–1269. 13. Sundarathiti P, Pasutharnchat K, Kongdan Y, Suranutkarin P. Thoracic epidural anesthesia (TEA) with 0.2% ropivacaine in combination with ipsilateral brachial plexus block (BPB) for modified radical mastectomy (MRM). J Med Assoc Thai. 2005;88:513–520. 14. Kaya M, Oğuz G, Şenel G, Kadıoğulları N. Postoperative analgesia after modified radical mastectomy: the efficacy of interscalene brachial plexus block. J Anesth. 2013;27:862–867. 15. Kolawole IK, Adesina MD, Olaoye IO. Intercostal nerves block for mastectomy in two patients with advanced breast malignancy. J Natl Med Assoc. 2006;98:450–453. 19. Blanco R. The “Pecs block”: a novel technique for providing analgesia after breast surgery. Anaesthesia. 2011;66:847–848. 20. Blanco R, Fajardo M, Parras Maldonado T. Ultrasound description of Pecs II (modified Pecs I): a novel approach to breast surgery. Rev Esp Anestesiol Reanim. 2012;59:470–475. 21. Ramsay MA, Savege TM, Simpson BR, Goodwin R. Controlled sedation with alphaxalone-alphadolone. Br Med J. 1974;2:656–659. 22. Aldrete JA. The post-anesthesia recovery score revisited. J Clin Anesth. 1995;7:89–91. 23. Desroches J, Grabs U, Grabs D. Selective ultrasound guided pectoral nerve targeting in breast augmentation: how to spare the brachial plexus cords?. Clin Anat. 2013;26:49–55. 24. Bremner-Smith AT, Unwin AJ, Williams WW. Sensory pathways in the spinal accessory nerve. J Bone Joint Surg Br. 1999;81:226–228. 25. Beheiry EE. Innervation of the pectoralis major muscle: anatomical study. Ann Plast Surg. 2012;68:209–214. 26. Porzionato A, Macchi V, Stecco C, Loukas M, Tubbs RS, Caro RD. Surgical anatomy of the pectoral nerves and the pectoral musculature. Clin Anat. 2012;25:559–575. 27. Hoffman GW, Elliott LF. The anatomy of the pectoral nerves and its significance to the general and plastic surgeon. Ann Surg. 1987;205: 504–507. 28. Sefa Özel M, Özel L, Toros SZ, et al. Denervation point for neuromuscular blockade on lateral pectoral nerves: a cadaver study. Surg Radiol Anat. 2011;33:105–108. 29. Davies F, Gladstone RJ, Stibbe EP. The anatomy of the intercostal nerves. J Anat. 1932;66:323–333. 30. Pérez MF, Miguel JG, de la Torre PA. A new approach to pectoralis block.. Anaesthesia. 2013;68:430. 16. Kundra P, Varadharajan R, Yuvaraj K, Vinayagam S. Comparison of paravertebral and interpleural block in patients undergoing modified radical mastectomy. J Anaesthesiol Clin Pharmacol. 2013;29:459–464. 31. Sopena-Zubiria LA, Fernández-Meré LA, Valdés Arias C, et al. Thoracic paravertebral block compared to thoracic paravertebral block plus pectoral nerve block in reconstructive breast surgery [in Spanish]. Rev Esp Anestesiol Reanim. 2012;59:12–17. 17. Exadaktylos AK, Buggy DJ, Moriarty DC, Mascha E, Sessler DI. Can anesthetic technique for primary breast cancer surgery affect recurrence or metastasis? Anesthesiology. 2006;105:660–664. 32. Norum HM, Breivik H. Thoracic paravertebral blockade and thoracic epidural analgesia: two extremes of a continuum. Anesth Analg. 2011;112: 990; author reply 990–991. 18. Louden K. Nerve block may reduce breast cancer recurrence and death. In: Presented at the American Society of Anesthesiology annual meeting, San Francisco, CA: Medscape Medical News; 2013. 33. Purcell-Jones G, Pither CE, Justins DM. Paravertebral somatic nerve block: a clinical, radiographic, and computed tomographic study in chronic pain patients. Anesth Analg. 1989;68:32–39. 74 © 2014 American Society of Regional Anesthesia and Pain Medicine Copyright © 2014 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited.