Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
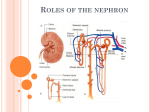
FORMATION OF URINE. The kidney produces urine containing metabolic wastes and regulates the composition of body fluids by three main processes: glomerular filtration, tubular reabsorption, and tubular secretion. A. Glomerular filtration 1. Definition: Glomerular filatration is the transfer of fluid and solutes from the glomerular capillaries along a pressure gradient into Bowman's capsule. Filtration is assisted by the following factors: 2. Mechanics of glomerular filtration a. The glomerular hydrostatic (blood) pressure forces fluids and solutes out of the blood and into Bowman's capsular space. b. Two forces oppose glomerular hydrostatic pressure. (1) The hydrostatic pressure exerted by the fluid in Bowman's capsule tends to move fluid from the capsule into the glomerulus. (2) The colloid osmotic pressure in the glomerulus, which is generated by the plasma proteins, is a pulling force for fluid from Bowman's capsule to enter the glomerulus. c. The effective filtration pressure (EFP) is the net driving force. It is the difference between the forces tending to force fluid out of the glomerulus into Bowman's capsule and the forces tending to move fluid into the glomerulus from Bowman's capsule. EFP = (glomerular hydrostatic pressure) &emdash;( (capsular pressure) + (glomerular colloid osmotic pressure)) 3. The glomerular filtration rate (GFR) is the amount of filtrate formed per minute in all the nephrons of both kidneys. In males, the rate is about 125 ml/min. or 180 L in 24 hours; in females, about 110 ml/min. 4. Composition of the glomerular filtrate a. The filtrate in Bowman's capsule is identical to that of plasma with respect to water and solutes of low molecular weight, such as glucose, chloride, sodium, potassium, phosphate, urea, uric acid, and creatinine. B. Tubular reabsorption. Most of the filtrate (99%) is selectively reabsorbed in the kidney tubules. Approximately 85% of the sodium chloride and water and all of the glucose and amino acids in the glomerular filtrate are absorbed in the proximal convoluted tubule. 1. Reabsorption of sodium ions (85%) 2. Reabsorption of chlorine ions and other negative ions 3. Reabsorption of glucose, fructose, and amino acids a. Glucose and amino acids share carriers with sodium ions and are moved by cotransport. b. Transport maximum(Tm):the maximum reabsorption capacity for glucose and amino acids by carriers in the tubular cell membranes, The Tm for glucose is approximately 200 mg glucose/100 ml plasma . When the blood level of glucose exceeds the Tm, the excess remains in the urine (glycosuria). 4. Reabsorption of water (85%) 5. Reabsorption of urea. All the urea formed dally Is filtered through the glomerulus. About 50% is passively reabsorbed due to a diffusion gradient created when water is reabsorbed. Therefore, about 50% of the urea filtered is excreted in the urine. 6. Reabsorption of other inorganic ions, such as potassium, calcium, phosphate, and sulfate, and of a number of organic ions is by active transport. C. Tubular secretion mechanisms are effective processes that transfer substances out of the blood in peritubular capillaries across the tubular cells into the tubular fluid for elimination in the urine. 1. Substances such as hydrogen, potassium, and ammonium ions, the metabolic end product creatinine and certain drugs (penicillin), are actively secreted into the tubules. 2. The selective tubular secretion of hydrogen and ammonium ions helps regulate plasma pH and the acid-base balance of the body fluids. URINE CONCENTRATION AND DILUTION MECHANISMS A. Urine volume. The daily volume of urine produced varies from 600 ml to more than 2,500 ml. B. The countercurrent multiplier system in the loop of Henle 1. A countercurrent system is one in which the inflow into a U-shaped tube (such as the loop of Henle) runs parallel, close to and in an opposite direction to the outflow from the tube. A countercurrent multiplier system is a countercurrent system assisted by active transport. 2. As the iso-osmotic (same concentration) glomerular filtrate enters and passes through the loop of Henle, it becomes progressively more concentrated (hyperosmotic) at the bottom of the loop: a. The descending limb of the loop of Henle is highly permeable to water and relatively impermeable to solutes such as NaCl b. The ascending limb is impermeable to water but relatively permeable to NaCl. This increases the osmotic concentration of NaCl in the interstitial fluid. c. Due to the increased osmolarity of the interstitial fluid, water moves out of the descending limb and the loop into the peritubular interstitial fluid by osmosis. Volume of the filtrate decreases as water leaves. Osmotic concentration of the filtrate increases as it rounds the hairpin turn of the loop of Henle. d. As the filtrate moves along the ascending limb, it looses sodium chloride. Because the ascending limb is impermeable to water, the water cannot follow, and the filtrate becomes progressively more dilute (hypoosmotic) as it passes upward toward the cortex. That is, the volume of the filtrate does not change, but the concentration declines. e. Some of the NaCl leaving the ascending limb moves by diffusion into the descending limb from the interstitial fluid, thereby increasing the solute concentration in the descending limb. Also, new NaCl in the glomerular filtrate continuously enters the tubule inflow to be transported out of the ascending limb into the peritubular interstitial fluid. Thus, the recycling mechanism multiplies the concentration of NaCl. f. The result is that the interstitial fluid surrounding the loop of Henle contains a high concentration of salt, as does the filtrate in the loop of Henle. A vertical concentration gradient from the cortex (iso-osmotic) to the medulla (hyperosmotic) is maintained. 3. The medullary recycling of urea helps maintain the vertical concentration gradient in the interstitial fluid and the loop of Henle. a. Urea diffuses passively out of the collecting ducts into the medullary interstitial fluid. Some urea diffuses from the medullary fluid into the descending limb. b. Thus, urea is recirculated between the collecting tubules and the descending limb. The high concentration of urea in the medullary interstitial fluid contributes to its osmolarity. This increases the osmotic movement of water out of the descending limb and increases the filtrate's concentration of NaCl in the descending limb. C. The countercurrent exchanger mechanism in the blood vessels and the renal tubules aids the countercurrent multiplier mechanism. 1. The capillaries of the vasa recta function as countercurrent exchangers, because the direction of blood flow around the loop of Henle is opposite to the direction of filtrate flow around the loop. 2. The walls of the vasa recta are permeable to NaCl and water. As blood flows down the descending vessel of the vasa recta, which is parallel to the ascending limb of the tubule, it becomes hyperosmotic as it picks up sodium and chlorine ions and loses some water. At the bottom of the capillary loop, the plasma osmolarity Is Identical to that of the surrounding interstitial fluid. 3. As the blood flows back up the ascending vessel of the vasa recta, which is parallel to the descending limb of the tubule, salt diffuses back out of the capillary and the water reenters the vessel. The osmolarity of the blood decreases as It flows toward the cortex. 4. Because of the passive exchange of salt and water between the vasa recta and the medullary Interstitial fluid and the fact that the blood flow in the vasa recta Is relatively slow, the blood leaves the medulla only slightly hyperosmotic to arterial blood. D. Excretion of a concentrated urine 1. The hypo-osmotic (dilute) filtrate in the ascending limb of Henle's loop enters the distal convoluted tubule and travels down the collecting duct toward the ureter. As a result of the countercurrent systems, the interstitial fluid surrounding the collecting ducts is hyperosmotic and the necessary concentration gradient for osmosis of water out of the ducts is established. 2. The collecting ducts are impermeable to water in the absence of ADH. Water will leave the collecting ducts by osmosis in the presence of ADH. E. Excretion of a dilute urine. When ADH is not present, the collecting ducts become almost impervious to water. The dilute urine enters the kidney pelvis to be excreted. Micturition Reflex A. Micturition (urination) Is dependent on parasympathetic and sympathetic innervation as well as voluntary nerve impulses. The expulsion of urine requires the active contraction of the detrusor muscle. 1. The micturition reflex is initiated when distention of the bladder by 300 ml to 400 ml of urine stimulates stretch receptors in the bladder wall. a. The micturition reflex causes contraction of the detrusor muscle and relaxation of the internal and external sphincters to result in emptying of the bladder. 2. Inhibition of the micturition reflex through voluntary control of the external sphincter is a learned response. DISORDERS OF THE URINARY SYSTEM A. Cystitis is inflammation of the urinary bladder. It may be due to a bacterial infection (usually Escherichia coli) that has spread from the urethra or may be an allergic reaction or the result of mechanical irritation of the bladder. B. Glomerulonephritis is inflammation of the nephrons, especially of the glomeruli. C. Kidney stones (urinary calculi) are formed from precipitated salts of calcium, magnesium, uric acid, or cysteine. Small stones may be passed in the urine; larger stones may become lodged in the ureter and cause intense pain (renal colic), which radiates from the kidney area to the groin.