Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
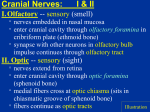
CRANIAL NERVES Bryan Sackey Pharmacy Biomedical Preview Program Summer 2012 [email protected] At the end of this presentation, participants should be able to discuss the: • Location and innervation of all twelve cranial nerves • Categorization of cranial nerves • Sensory • Motor • Mixed • Basic function of cranial nerves • Some clinical manifestations of cranial nerve damage Cranial Nerves • Humans possess 12 cranial nerves which emerge from the brain • All cranial nerves arise from brain stem except the 1st and 2nd (Olfactory and Optic nerve) • 1st and 2nd arise from cerebrum • Categorized as either sensory, motor or mixed (both sensory and motor) • 3 sensory • 5 motor • 4 mixed Cranial nerve I: Olfactory Nerve • Arises from Olfactory epithelium of cerebrum • Olfactory bulb • Enters the nasal cavity • Solely Sensory function • Functions in the special sense of smell • Clinical Implications • Anosmia Cranial Nerve II: Optic Nerve • Arises from retina of eye • Pass through optic canal and converge at optic chiasm then to visual cortex • Solely Sensory function • Carriers afferent impulses for vision • Clinical implications: • Blindness • Tunnel vision Cranial Nerve III: Oculomotor nerve • Arises from the midbrain • Enters Superior orbital fissure (to eye) • Solely Motor function • Innervates 5 extraocular muscles of the eye • Superior rectus – rotates eye upward • Medial rectus – rotates eye medial • Inferior rectus – rotates eye downward • Inferior oblique – rotates eye upward and laterally • Levator palebrae superioris – lifts up eyelids • Clinical implications • External strabismus Cranial Nerve IV: Trochlear Nerve • Arises from midbrain • Enters superior orbital fissure • Motor function • Innervates superior oblique muscle • Moves eye downward and medially • Clinical Manifestation • Damage to nerve causes eye to rotate laterally note: this is the right eye with the nose to the left of it Cranial Nerve V: Trigeminal Nerve • Arises from the pons • Has BOTH motor and Sensory functions (mixed nerve) • Composed of 3 branches • V1: Ophthalmic branch – superior orbital fissure • V2: Maxillary branch – foramen rotundum • V3: Mandibular branch – foramen ovale • V1 and V2 conveys sensory impulses from various parts of the face and V3 is responsible for mastication (motor) • Clinical Implications • Herpes Zoster • Tic Douloureax Cranial Nerve VI: Abducens Nerve • Arises from the pons • Enters superior orbital fissure • Solely Motor function • Innervates lateral rectus muscle of the extraocular muscle in eye • pulls eye laterally (abducts eye abducens!) • Clinical Implications • Internal strabismus Cranial Nerve VII: Facial Nerve • Arises from pons • Enters through stylomastoid foramen to the lateral aspect of face • BOTH motor and sensory function (mixed nerve) • Motor functions involves facial expression • Sensory function is taste from anterior 2/3 of tongue • Clinical Implications • Bell’s Palsy • paralysis of facial muscle leading to asymmetrical facial expression Cranial Nerve VIII: Vestibulocochlear • Arise from pons • Enter hearing and equilibrium apparatus of middle ear • Sensory function • Hearing and balancing • Clinical implications • Deafness • Tinnitis • Vertigo Cranial Nerve IX: Glossopharyngeal • Arises from medulla • Enters jugular foramen and runs to throat • BOTH motor and sensory function • Motor function innervates part of tongue for movement and salivary gland • Supplies sensory fibers to posterior 1/3 of tongue • Helps taste and swallow food • Clinical implications • Dysphagia • Swallowing difficulty Cranial Nerve X: Vagus Nerve • Arises from medulla • travels through jugular foramen • Only cranial nerve that extends beyond the head and neck • BOTH motor and sensory function • Motor functions are parasympathetic fibers to the heart, lungs, digestion, and visceral organs • Involved in swallowing and speech • Sensory functions is taste • Clinical implications • Responsible for many visceral functions so if damaged may lead to problems with visceral organs • Dysphagia Cranial Nerve XI: Accessory Nerve • Arises from Medulla • Enters through foramen magnum • Solely Motor function • Innervates sternocliedomastoid muscle and trapezius muscle • Responsible for head movement and neck rotation • An accessory to the motor functions of Vagus nerve by innervating larynx, pharynx, and soft palate • Clinical manifestations • Inability to shrug Cranial Nerve XII: Hypoglossal Nerve • Arise from Medulla • Enters through hypoglossal canal • Solely Motor function • Innervates both intrinsic and extrinsic muscles of tongue • Involved in protraction of tongue • Involved with swallowing and speech • Clinical implications • Deviation of tongue Summary • 3 sensory • Olfactory (CN I), Ophthalmic (CN II), Vestibulocochlear (CN VIII) • 5 motor • Oculomotor (CNIII), Trochlear (CN IV), Aducens (CN VI), Accessory (CN XI), Hypoglossal (CN XII) • 4 Mixed (both motor and sensory) • Trigeminal (CN V), Facial (CN VII), Glossopharyngeal (CN IX), Vagus (CN X) • 3 involved in taste • Facial (CN VII), Glossopharyngeal (CN IX), Vagus (X) • 2 involved in speech • Vagus (CN X), Hypoglossal (CN XI) • 3 involved in eye movement • Oculomotor (CN III), Trochlear (CN IV), Abducens (CN IV) • 1 leaves head and neck area • Vagus nerve (CN X)