Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
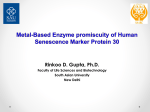
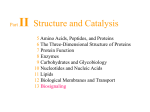
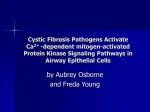
Chapter 27: Ca2+-Sensing Receptor Edward M. Brown From the Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, 7th Edition. www.asbmrprimer.org Figure 1 Figure 1 Predicted structure of the human CaSR (see text for details). SP, signal peptide; HS, hydrophobic segment. Xs show examples of sites of naturally occurring inactivating mutations, and asterisks indicate locations of activating mutations. (Reproduced in modified form with permission from Elsevier from Brown EM, Bai M, Pollak M 1999 In: Avioli L, Krane SM (eds.) Metabolic Bone Disease and Clinically Related Diseases. Academic Press, San Diego, CA, USA, pp. 479–499. Copyright Elsevier 1999.) From the Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, 7th Edition. www.asbmrprimer.org Figure 2 Figure 2 Mechanisms through which the CaR reduces maximal urinary-concentrating ability (see text for additional details). Elevated concentrations of Ca2+ in the blood activate the CaSR in the CTAL, which inhibits the reabsorption of Ca2+, thereby increasing the concentration of Ca2+ in the tubular fluid. Concomitant activation of the CaSR in the MTAL reduces transport of NaCl into the medullary interstitium, and, as a consequence, decreases maximal urinary concentrating ability by inhibiting countercurrent multiplication. If the level of Ca2+ in the tubular fluid remains high when it reaches the IMCD, activation of the CaSR on the apical membrane of the tubular epithelial cells directly inhibits vasopressin-stimulated reabsorption of water, further decreasing the concentration of Ca2+ in the final urine, and presumably the risk of forming Ca2+-containing kidney stones. (Reproduced with permission from Brown EM, Hebert SC 1997 Novel insights into the physiology and pathophysiology of Ca2+ homeostasis from the cloning of an extracellular Ca2+-sensing receptor. Reg Peptide Lett VII:43–47.) From the Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, 7th Edition. www.asbmrprimer.org Figure 3 Figure 3 Multiple agonists and other factors modulating the activity of the CaSR as well as the numerous intracellular signaling pathways through which the receptor can regulate cellular function. Ca2+, Mg2+, aminoglycoside antibiotics, spermine and other polyamines, and amyloid β peptides are examples of polycationic agonists of the CaSR. Aromatic amino acids and calcimimetics—drugs that activate the receptor and are used to control hyperparathyroidism—are allosteric modulators of the CaSR. The former bind to a site near a putative calcium-binding site in the receptor’s ECD, whereas the latter bind to the CaSR’s transmembrane domains; both increase its apparent affinity for polycationic agonists. AA, arachidonic acid; AC, adenylate cyclase; cAMP, cyclic AMP; cPLA2, cytosolic phospholipase A2; DAG, diacylglycerol; ERK, extracellular signal-regulated kinase; Gαi and Gαq, α subunits of the i- and q-type heterotrimeric G-proteins, respectively, Ins(1,4,5)P3, inositol 1,4,5-trisphosphate; Ins(1,4,5)P3R, 1,4,5trisphosphate receptor; JNK, Jun N-terminal kinase; MAPK, mitogen-activated protein kinase; MEK, MAPK kinase; PI4K, phosphatidylinositol 4-kinase; PKC, protein kinase C; PLC, phospholipase C; PtdIns(4,5)P2, phoasphatidylinositol-4,5-bisphosphate. (Reprinted with permission from Macmillan Publishers from Hofer A, Brown EM 2003 Extracellular calcium sensing and signaling. Nat Rev Cell Mol Biol 4:530–538.)