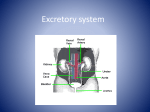
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Creatinine Creatinine is the waste product formed in muscle from a high energy storage compound ,creatine phosphate (phosphocreatine). ATP is the immediate source of energy for muscular contraction as it hydrolyzed to ADP. Creatine phosphate can be stored in muscle at 4 times the concentration ATP. Small amount of creatinine is ingested as constituent of meat. Creatinine is the best indicator of renal function than others. The amount of creatinine excreted daily is a function of the muscle mass and is not affected by diet, age and sex. Schema for the formation of creatinine in muscle. CK (creatine kinase) Creatine phosphate and ADP are converted by enzymatic action to creatine and ATP. A side reaction occurs and small portion of the creatine phosphate loses its phosphate as phosphate ion, with closure of the ring to form creatinine. Normal range of creatinine in serum: adult male: 0.7-1.4 mg/dl female: 0.6-1.3 mg/dl children: 0.4-1.2 mg/dl Increase concentration A) Prerenal factor: - Congestive heart failure - Shock - Salt and water depletion associated with vomiting, diarrhea, uncontrolled diabetes, excessive use of diuretics and excessive sweating. B) Renal factors: - Involve damage to glomeruli, tubules, renal blood vessels. C) Postrenal factors: - Prostatic hypertrophy - Neoplasms compressing the ureters - Calculi blocking the ureters - Congenital abnormalities that compress or block the ureters Decrease concentration Low serum creatinine concentration has no clinical significance Urine creatinine The concentration of creatinine in urine is much higher than in serum (about 1mg/ml). Normal range of urine creatinine concentration (roughly): Men: 2.0 g/ 24 hours women: 1.6 g/24 hours Children: new born 7 mg/kg/24 hours 1.5-22 mo: 5 mg/kg/24 hours 2.5-3.5 years: 9 mg/kg/24 hours 4-10 years: 15 mg/kg/24 hours Creatinine Clearance The most sensitive method of assessing renal function. Provide an estimate of the amount of the plasma that must have flowed through the kidney glomeruli per minute with the complete removal of creatinine to account for creatinine per minute actually appearing in the urine. The creatinine clearance is calculated as U/S X V where u creatinine concentration in urine S creatinine concentration in serum V volume of urine excreted per minute 120±25 ml/min for male 112±20 ml/min for female Estimation of creatinine clearance A number of formulae exist for predicting creatinine clearance (or GFR) from plasma [creatinine] and other readily available information, such as age, sex and weight. The best known of these is that of Cockcroft and Gault (1976): Creatinine clearance = (140 − age) × wt × (0.85 if patient is female) 0.814 × serum[creatinine] (creatinine clearance in ml/min, age in years, weight in kg, [creatinine] in μmol/L). Blood Urea Nitrogen (BUN) When protein are ingested, they are hydrolyzed to amino acids (a.a). Amino acids are used for anabolic or catabolic. Excess proteins cannot be stored in the body. The amino α-group of all a.a that are broken down in the mammalian body, end up in the urea compound. Urea appears in renal glomerular filtrate in the same concentration as in plasma, 40% urea is reabsorbed in renal tubule. As with creatinine, the serum urea rises with impairment renal function. Serum concentration of urea is affected strongly by the degree of protein catabolism. In the case of diet, a change to high protein diet can double the serum urea, and a low protein intake can reduce it by half. A) Illustration of the fate of ingested protein B) The reaction that occurs when urea is split by urease Urea formation pathway Urea cycle Urea production occurs almost exclusively in liver. Urea is produced from ammonia in five enzymatic steps. 1) Carbamoyl phosphate synthetase I. 2) Ornithine transcarmoylase. 3) Argininosuccinate synthetase. 4) Argininosuccinase. 5) arginase Normal range of serum urea concentration: 15-45mg/dl Increase concentration high protein diet Administration of cortisollike steroids Stressful situation Prerenal, renal, and postrenal factors Decrease concentration late in pregnancy Starvation Low protein diet Uric acid Uric acid is a purine compound that circulated in plasma as sodium urate and is excreted by kidney. It is derived from the breakdown of nucleic acid. Uric acid are ingested or come from the destruction of tissue cells and synthesized in the body from simple compounds. Urate appears in the glomerular filtrate and partially reabsorbed in tubules. Urate is of low solubility in plasma and uric less. Urate deposition in the kidney may lead to renal failure There is a danger of precipitation of uric acid crystal where there is local rise in H+ concentration. Schematic representation of uric acid formation and excretion Purines catabolism in other organisms Uric acid is the excreted end product of purine catabolism in primates, birds, and some other animals. In most mammals and many other vertebrates , uric acid is further degraded to allantoin by the action of urate oxidase. In other organisms the pathway is further extended as shown Illustration of uric acid pathway Purines catabolism Purine nucleotides are degraded by pathway in which they lose their phosphate through the action of 5‘-nucleotidase. Adenylate yields adenosine, which is deamination to inosine by the action of adenosine deaminase. Inosine is hydrolyzed to hypoxanthine and D-ribose. Hypoxanthine is oxidized successively to xanthine and then uric acid by xanthine oxidase . GMP catabolism also yields uric acid as end product. Gout disease Gout is a form of acute arthritis that causes severe pain and swelling in the joints. It most commonly affects the big toe, but may also affect the heel, ankle, hand, wrist, or elbow. It affects the spine often enough to be a factor in back pain. Gout usually comes on suddenly, goes away after 5-10 days, and can keep recurring. Gout is different from other forms of arthritis because it occurs when there are high levels of uric acid circulating in the blood, which can cause urate crystals to settle in the tissues of the joints Normal range of uric acid: male: 3.5-7.5 mg/dl female: 2.5-6.5 mg/dl children: 2.0-5.5 mg/dl Increase concentration Decrease concentration Gout disease Renal disease After increased breakdown of nucleic acid and nucleoprotein ( leukemia, polycythemia, toxemia of pregnancy, and after irradiation of x-ray sensitive carcinomas) After the administration of ACTH or cortisol – like steroids Certain drugs that decrease the reabsorption of urate by renal tubules ( aspirin, probenecid, penicillamine) by drugs (allopurinol) that block a step in formation of uric acid. . Primary hyperuricemia Increased production of uric acid from purine kidneys cannot get rid of the uric acid in blood, resulting in high levels Secondary hyperuricemia o Certain cancers, or chemotherapy agents may cause an increased turnover rate of cell death. This is usually due to chemotherapy, but high uric acid levels can occur after chemotherapy is administered. o After chemotherapy, there is often a rapid amount of cellular destruction, and tumor lysis syndrome may occur. Tumor lysis syndrome like in certain types of leukemia, lymphoma, or multiple myeloma, o o Medications - can cause increased levels of uric acid in the blood Endocrine or metabolic conditions -certain forms of diabetes, or acidosis can cause hyperuricemia o Elevated uric acid levels may produce kidney problems, or none at all. People may live many years with elevated uric acid levels, and they do not develop gout or gouty arthritis (arthritis means "joint inflammation").