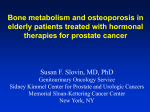
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
قد يكون بمقدور أحد الجينات تسهيل عمل األطباء في معرفة ما إذا كان مريض البروستات يعاني من سرطان خبيث .أو من نوع آخر ال يشكل خطرا على حياته وقد يكون هذا األمر مهما بالنسبة آلالف الرجال الذين يتلقون عالجا مكثفا باألشعة أو معرضين للخضوع لجراحة .استئصالية قد ال يحتاجون إليها وقد يسبب كال النوعين من العالج ضررا في األعصاب مما يجعل الرجل مصابا بانفالت السيطرة على البول أو .بالعجز الجنسي أو بكالهما وربما يساعد هذا االكتشاف العلمي ،على المدى الطويل ،األطباء على تطوير عالج للسيطرة حتى على السرطانات .الخبيثة ويعد سرطان البروستات من أكثر األورام شيوعا لدى الرجال في بريطانيا .ويعتقد أن النسبة األكبر من سرطانات .البروستات خاملة وليس من المرجح أن تسبب مشكلة للمريض خصوصا إذا كان متقدما في السن .والمشكلة التي يواجهها األطباء هي تشخيص السرطان القابل لالنتشار السريع خارج غدة البروستات نفسها وفي هذه الحالة يحتاج األمر إلى عالج فعال في حال تمكن المصاب من النجاة ،ألنه ما أن ينتشر السرطان حتى .يصبح من الصعب عالجه EZH2.والجين مدار البحث في الدراسة األخيرة التي قام بها فريق من جامعة مشيغان يدعى كشف علمي وقد الحظ الباحثون لدى فحص أنسجة مأخوذة من مصابين بالسرطان إن هذا الجين فعال جدا لدى الذين يعانون من .سرطان خبيث قابل لالنتشار خارج غدة البروستات .ويعني ذلك نظريا إن بإمكان األطباء تحديد درجة خطورة السرطان والعالج المطلوب .ويمكن بذلك تجنيب المرضى بسرطان خامل ال ينتشر أنواع العالجات التي تسبب أضرارا أخرى ويعتبر القائمون على البحث النتائج التي توصلوا إليها كشفا علميا ال بالنسبة لعمليات التشخيص فحسب بل كذلك بالنسبة للعالج في المستقبل .ويقولون إن الجين المكتشف جين رئيسي يتحكم بنشاط 02جين آخر يعتقد أن لدى .بعضها قدرة على تثبيط النشاط السرطاني وسيكون هذا الجين مستقبال هدفا للعالجات التي قد يمكن التوصل إليها لوقف انتشار سرطان البروستات BBC news ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ Prostate cancer is a type of cancer that affects the prostate gland in men. The prostate is located beneath the bladder, in front of the rectum, and wraps around part of the urethra. Causes and Risk Factors of Prostate Cancer We have yet to discover the exact causes of prostate cancer, but researchers have identified risk factors. Prostate cancer risk factors include: Age. As men age, the risk of developing prostate cancer naturally increases. At age 50, the risk dramatically increases. Race. The risk of prostate cancer is higher among African Americans, intermediate among Caucasians, and lowest among Asian and Hispanic males. The reason behind risk inequalities among the races has not been found. Family History. Having a father or brother with prostate cancer increases your risk. Studies show that prostate cancer can run in families and inherited genetic mutations may be the cause. You don't need a family history to be at risk. However, most diagnosed men do not have a family history of the disease. Diet. Ongoing studies question how diet affects prostate cancer development. Some studies suggest that a diet high in animal and dairy fats may slightly raise a man's risk. Other studies suggest a diet low in fruits and vegetables may also increase the risk. How Saturated Fats Increase Your Prostate Risk How More Sex Can Decrease Your Prostate Cancer Risk Symptoms of Prostate Cancer Prostate cancer symptoms do not usually appear until the disease has spread beyond the prostate gland. As prostate cancer advances, the prostate constricts the urethra, causing difficulties in urination -- a common symptom. Prostate cancer symptoms include: burning or pain during urination inability to urinate even though you feel the urge to frequent urination, especially during the night weak urine stream blood in urine or semen lower back pain, ache, or stiffness; may also occur in hips and upper thighs painful ejaculation Symptoms related to urination may be common with prostate cancer, but are also symptoms related to other prostate conditions like an inflamed or enlarged prostate. Diagnosis of Prostate Cancer Because prostate cancer commonly doesn't have symptoms in the early stages, it is usually a screening test that reveals a prostate abnormality that may indicate cancer. The American Cancer Society recommends that men who are at average risk of prostate cancer be offered a prostate specific antigen (PSA) test and digital rectal exam (DRE) annually beginning at age 50. Men who are at a higher risk should begin screening earlier, at age 45, or at their doctor's recommendation. Routine screening tests include the DRE and PSA test. When Should You be Screened for Prostate Cancer? PSA Test Results: What Does a High PSA Mean? If screening test results are suspicious, further examination of the prostate may be required. This can be done through a transrectal ultrasound and/or a prostate biopsy. A transrectal ultrasound is a small probe that is inserted through the rectum that provides images of the prostate. It can detect prostate abnormalities that could indicate prostate cancer, but it is ultimately a prostate biopsy that confirms the presence of the disease. During a prostate biopsy, small samples of prostate tissue are removed that are screened for cancer by a pathologist. With the aid of a transrectal ultrasound, the doctor uses a special spring-loaded biopsy instrument to remove several small tissue samples. If the biopsy samples reveal cancer, then the pathologist further examines the cells to determine the grade of the tumor and the Gleason score. Staging is also a necessary step in assessing prostate cancer and planning a course of treatment. Staging refers to how far the disease has spread. Screening test results and biopsy findings determine if further testing are required for staging. There are four stages of prostate cancer: stage I, stage II, stage III, and stage IV. Treatment of Prostate Cancer Treatment for prostate cancer heavily relies on the stage of the disease, the aggressiveness of the tumor, and overall general health. Watchful Waiting. Watchful waiting is a type of treatment where the prostate cancer is monitored, but no treatment is provided to remove the cancer. This option is sometimes recommended for older men whose prostate cancer is slow-growing and is confined to the prostate. Surgery. A prostatectomy (surgical removal of the prostate) is a common treatment method in men whose cancer has not spread beyond the prostate, but may also be performed on later stages, as well. Radiation Therapy. Radiation therapy uses certain types high energy beams of radiation to shrink tumors or eliminate cancer cells. Radiation therapy works by damaging a cancer cell's DNA, making it unable to multiply. Two primary types of radiation therapy are external beam radiation therapy and (EBRT) internal beam radiation, also called brachytherapy. How External Beam Radiation Therapy is Used to Treat Prostate Cancer Brachytherapy and Prostate Cancer: What You Need to Know Chemotherapy.The organs in our body are made of cells that divide and multiply as the body needs them. When these cells continue to multiply unnecessarily, the result is a mass or growth, also called a tumor. Chemotherapy drugs work by eliminating these rapidly multiplying renegade cells. Chemotherapy may be a treatment option for men whose prostate cancer is advanced and has spread to other parts of the body. Cryotherapy. During cryotherapy, prostate cancer is treated by freezing prostate tissue. This type of treatment is ideal for men whose tumors are contained within the prostate. Hormone Therapy. Hormone therapy works by suppressing hormone levels that can fuel prostate cancer cells to multiply. Types of hormone therapy include Source: an orchiectomy: the surgical removal of the testicles to lower hormone levels luteinizing hormone-releasing hormone (LHRH) agonists: drugs that help prevent the testicles from producing testosterone antiandrogens: drugs that inhibit androgen activity "General Information About Prostate Cancer." Prostate Cancer Treatment PDQ. National Cancer Institute. 23 May 2008. Accessed 09 July 2008. Cancer.about.com ــــــــــــــــ ـــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ ـــــــــــــــــــــــــــــــــــــــــــ Increased Risk of Metabolic Syndrome, Diabetes Mellitus, and Cardiovascular Disease in Men Receiving Androgen Deprivation Therapy for Prostate Cancer Posted 01/13/2009 Polly E. Kintzel, Pharm.D.; Sandra L. Chase, Pharm.D.; Lisa M. Schultz, Pharm.D.; Timothy J. O'Rourke, M.D. Author Information Abstract and Introduction Abstract Prostate cancer is the leading cancer diagnosis and second leading cause of cancer-related mortality for men in the United States. Due to the increased prevalence of prostate cancer in men older than 50 years, men at risk for prostate cancer represent the same population of men who are at greatest risk for metabolic syndrome, diabetes mellitus, and coronary artery disease (CAD). In addition to risk factors for CAD that are applicable to the general population, men with prostate cancer can be at increased risk for CAD due to long-term androgen deprivation therapy (ADT) administered as treatment for prostate cancer. Men undergo ADT by medical (drug therapy) or surgical (castration) means. Luteinizing hormone–releasing hormone (LHRH) agonists are the primary drug therapies used for ADT. Commercially available LHRH agonists are goserelin, histrelin, leuprolide, and triptorelin. Body composition changes, hyperlipidemia, insulin resistance, metabolic syndrome, and acute coronary syndrome are all reported adverse effects of ADT, which are consequences of reduced levels of circulating testosterone. Metabolic and body composition changes associated with ADT arise within months of beginning medical ADT and persist after discontinuation of therapy. To better understand the increased risk of metabolic syndrome, diabetes, and heart disease in patients undergoing ADT for prostate cancer, we performed a MEDLINE search (1986–2008) to identify pertinent studies and reports. Additional citations were obtained from the articles retrieved from the literature search. We found that the increased risk for serious cardiovascular disease becomes evident within months of beginning ADT. Pharmacists should provide counseling to these patients on primary disease prevention. Men receiving ADT should be monitored routinely for signs and symptoms of metabolic syndrome, diabetes, and CAD. Healthy lifestyle practices should be encouraged, and physical therapy should be considered for these patients. Introduction Prostate cancer is the leading cancer diagnosis and second leading cause of cancer-related mortality for men in the United States. In 2007, prostate cancer was diagnosed in approximately 220,000 men, and about 27,000 deaths were attributed to this disease.[1] Increasing age is the greatest risk factor for prostate cancer. The probability of being diagnosed with prostate cancer is 1 in 10,373 for men younger than 40 years. However, this probability increases with age to 1 in 39 at 40–59 years, 1 in 14 at 60–69 years, and 1 in 7 at 70–79 years.[1] Additional risk factors include African-American race, positive family history, and a diet high in animal fat and red meat consumption.[2] The prognosis for men with prostate cancer is quite variable and relates to disease characteristics, such as tumor size, prostate-specific antigen (PSA) level, Gleason score (risk assessment based on histologic findings), malignant extension outside of prostate capsule, seminal vesicle invasion, involvement of regional lymph nodes, and distant sites of metastatic disease.[2] Men with low-risk localized prostate cancer generally live with their tumor and eventually succumb to morbidity and mortality unrelated to malignant disease.[3,4] Fortunately, most cases of prostate cancer are diagnosed when the disease is localized to the prostate. In this group, the 5-year survival rate approaches 100%,[1,2] and the disease is largely asymptomatic except for difficulties from bladder outlet obstruction.[2] Unfortunately, for cases of recurrent or disseminated prostate cancer, the median overall survival time is 12–18 months.[1,2] Complications associated with advanced disease can be debilitating and include hypercalcemia, hypocalcemia, spinal cord compression, osteoblastic bone lesions, and chronic pain.[2] The mean age at death for men with prostate cancer of all prognostic risk levels is 79 years, and the leading cause of death is cardiovascular disease.[4] Due to the increased prevalence of prostate cancer in men older than 50 years, men at risk for prostate cancer represent the same population of men who are at risk for metabolic syndrome, diabetes mellitus, and coronary artery disease (CAD).[5] Of these conditions, CAD is the most immediately life threatening. Approximately 60 million people in the United States have CAD, and every year approximately 42% of all deaths are attributed to CAD.[5] The major risk factors for CAD include age and sex (male > 45 yrs, female > 55 yrs), positive family history, elevated low-density lipoprotein cholesterol (LDL) level, low high-density lipoprotein cholesterol (HDL) level, hypertension, diabetes, and tobacco use.[6] In addition to these risk factors for CAD that are applicable to the general population, men with prostate cancer can be at increased risk for CAD due to use of androgen deprivation therapy (ADT). Hyperlipidemia, insulin resistance, metabolic syndrome, and acute coronary syndrome are all reported consequences of ADT. Body composition changes that yield increased fat content occur with long-term administration of a luteinizing hormone–releasing hormone (LHRH) agonist.[7,8] Additional common adverse effects of ADT include hot flushes, fatigue, decreased libido, decreased quality of life, reduced bone mineral density (BMD), and anemia. Adverse effects caused by ADT administration are consequences of reduced levels of circulating testosterone.[7,9,10] Nonmalignant prostate tissue requires androgenic stimulation for growth, regular function, and morphologic integrity. This quality persists with the development of most cases of prostate cancer. Subsequently, interruption of androgenic activity is detrimental to the viability of malignant and nonmalignant prostate tissue.[2,11] Androgen deprivation therapy for the treatment of prostate cancer dates back to 1941.[2,11] First-line ADT is accomplished medically by using drug therapies that reduce or antagonize the effects of testosterone. The LHRH agonists are the mainstay of the drugs used to induce medical castration. The LHRH agonists are analogs of endogenous gonadotropin-releasing hormone that induce castration levels of testosterone in men by negative regulation of luteinizing hormone and follicle-stimulating hormone secretion from the anterior pituitary gland. Commercially available LHRH agonists are goserelin, histrelin, leuprolide, and triptorelin.[12] These products are available as depot formula-tions that are administered by intramuscular injection every 3–12 months.[13] Additional methods of ADT include bilateral orchiectomy and androgen-blocking agents. Bilateral orchiectomy provides ADT by removing the source of endogenous testosterone. Bilateral orchiectomy and LHRH agonist therapy are considered to be equally effective; however, most men prefer drug therapy over surgery.[2,12] Drugs categorized as androgen-blocking agents bind cytosolic androgen receptors and act as competitive inhibitors to prevent the initiation of androgen-mediated biologic activity.[11] Androgen-blocking agents are generally administered in combination with LHRH agonists or as a second-line alternative to them.[14] Commercially available androgen-blocking agents are bicalutamide, flutamide, and nilutamide. These products act as competitive inhibitors of androgen at the androgen receptor.[13] Both androgenblocking agents and LHRH agonists are normally administered continuously. Intermittent administration of ADT, which is related to serum PSA level results, is undergoing evaluation as a method to delay the development of androgen-refractory prostate cancer and reduce treatment-related adverse effects.[2,14] Clearly there is benefit to ADT for the reduction of morbidity in patients with advanced androgen-sensitive prostate cancer.[12,14] However, ADT is not considered curative therapy for prostate cancer, and its role is less well defined in early stages of the malignancy because of the variable nature of disease progression.[3,12,15] To better understand the increased risk for metabolic syndrome, diabetes, and heart disease in patients receiving ADT for prostate cancer, we performed a search of the medical literature using MEDLINE (1986–2008). Subject headings and key words used were prostatic neoplasms, prostate cancer, leuprolide, goserelin, histrelin, triptorelin, and androgen deprivation therapy. The search was limited to English-language journals and human studies. Clinical and epidemiologic studies pertaining to metabolic syndrome, diabetes, and heart disease in patients undergoing ADT for prostate cancer were included. Additional citations were identified from the studies retrieved from the literature search. The methods of studies published by the same authors were scrutinized to ensure that duplicated data were not inadvertently presented as additional data. Clinical Studies of Androgen Deprivation Therapy Body Composition and Biochemical Changes Androgen deprivation therapy is associated with development of body composition and biochemical changes characteristic of metabolic syndrome, diabetes, and CAD. Increased body fat content and reduced lean body mass develop subsequent to initiation of therapy.[8,16–18] Mean body weight has been shown to increase up to 3.1% and fat content 4.3–20%, after 12 months of ADT for the treatment of locoregional prostate cancer. Lean body mass was shown to decrease 1.4–3.8%.[8,16–19] Two studies demonstrated that body composition changes were evident after 6 months of ADT, with trends continuing, albeit at a less abrupt trajectory, when the patients were measured after 12 months of therapy.[16,19] The reported effects of ADT on plasma lipid profiles are variable ( Table 1 ). After adjustment for body mass index (BMI), significantly higher fasting levels of total cholesterol (p=0.02), LDL (p=0.04), and non-HDL (p=0.03) were noted in 16 men after at least 12 months of ADT for recurrent or metastatic prostate cancer compared with 14 matched control patients with locoregional prostate cancer not receiving ADT and 14 matched controls without prostate cancer.[20] This study did not find significant differences in fasting HDL levels, triglyceride levels, or the total cholesterol:HDL ratio among the designated groups. Another study reported elevated levels of LDL (p=0.03), HDL (p=0.002), and triglycerides (p=0.39) in 26 men receiving ADT with leuprolide for a 12-month period.[19] The rate of increase was greatest during the first 3 months of therapy. (This study was omitted from Table 1 because many of the results were shown as graphs without the actual numeric values.) However, significant reduction in HDL (p<0.05) and elevation in triglyceride (p<0.05) levels were reported in men with localized prostate cancer after 3 months of ADT relative to untreated controls.[17] Another study documented a significant increase in plasma HDL (p<0.005) and triglyceride (p<0.05) levels without significant changes in plasma total cholesterol or LDL values after 2.5 years of treatment with cyproterone acetate (a steroidal compound with antiandrogenic activity).[25] Hyperglycemia and insulin resistance can occur with ADT.[22–24,26] Statistically significant increases in fasting insulin levels (p=0.04) and hemoglobin A1c (p<0.001) were documented 3 months after initiation of ADT in 25 nondiabetic men with locally advanced or recurrent prostate cancer.[23] Insulin sensitivity gauged with use of the homeostatic model decreased 12.8% (p=0.02) in this group of men. Metabolic Syndrome and Diabetes Mellitus The frequency of metabolic syndrome developing in patients with prostate cancer was evaluated in a cross-sectional study that compared 20 men undergoing ADT for at least 12 months, 18 age-matched patients with prostate cancer without previous or current ADT, and 20 age-matched male control subjects ( Table 1 ).[21] Metabolic syndrome was defined according to the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) criteria for men; men who met three of the following five criteria were considered to have metabolic syndrome: waist circumference greater than 40 inches, fasting blood glucose level above 110 mg/dl, fasting triglyceride level above 150 mg/dl; fasting HDL level below 40 mg/dl; and blood pressure greater than 130/85 mm Hg.[6] More than half of the men in the ADT group were categorized as having metabolic syndrome. The prevalence of metabolic syndrome was more than 2-fold higher in the group receiving ADT compared with the control group with prostate cancer (p<0.01) and the control group without prostate cancer (p=0.03). The existing conditions defining metabolic syndrome in the ADT group were truncal obesity (p=0.007), hyperglycemia (p=0.006), and hypertriglyceridemia (p=0.06). Hypertriglyceridemia was significantly greater in the ADT group compared with the control group without prostate cancer (p=0.02). The BMI in the ADT group was significantly greater than that of the control group without prostate cancer (p=0.001), although it was similar to that of the control group with prostate cancer. All groups were similar in terms of low HDL levels and prevalence of hypertension. Total cholesterol levels were similar among the three groups (p=0.11). One subject in the ADT group and one subject in the control group had preexisting diabetes mellitus. Both patients were included in the analysis. The average duration of ADT was 45 months (range 12–101 mo). Most men (85%) in the ADT group were receiving treatment with an LHRH agonist. Three men (15%) in the ADT group had undergone bilateral orchiectomy. As expected, serum testosterone was at castration levels for men receiving ADT (mean ± SD 10.9 ± 15.8 ng/ml), whereas testosterone was measured at normal concentrations (> 280 ng/ml) for the control group with prostate cancer (mean ± SD 325.4 ± 103.6 ng/ml) and the control group without prostate cancer (mean ± SD 506.8 ± 161.0 ng/ml; p<0.0001). Increased risk of new-onset diabetes and worsening parameters of glycemic control in diabetic patients attributed to ADT were reported in two studies, one of which was a retrospective analysis of patients with prostate cancer who were receiving ADT at a single institution[26] and the other an observational study of Medicare recipients with a diagnosis of locoregional prostate cancer.[27] The retrospective study identified 396 men receiving treatment with ADT at a Veterans Affairs medical center from 1989–2005.[26] Men who received neoadjuvant (presurgical) treatment only were excluded from analysis. The ADT consisted of medical castration for 94% and surgical castration for 6%. Three hundred sixty patients (91%) received continuous ADT (medical or surgical), and 36 patients (9%) received intermittent administration. Of the 396 patients, 257 (65%) had locoregional disease, although all stages of prostate cancer were included in the population evaluated. Disease stage could not be determined for 125 men (32%). Approximately one third of patients were receiving ADT as primary therapy for prostate cancer. For the remainder of patients, ADT was salvage therapy after evidence of disease progression (increasing PSA level) despite prostatectomy, brachytherapy, cryoablation, and external beam radiation therapy. Mean follow-up was 66.1 months (range 10.7–208.2 mo). The study population included 113 patients with diabetes, of which 77 cases (68%) were a preexisting comorbidity and 36 cases (32%) developed after initiation of ADT ( Table 2 ). Management of new-onset diabetes included insulin therapy (11%), oral hypoglycemic drugs (53%), and initiation of the American Diabetic Association diet (36%). Patients with preexisting diabetes had a significantly greater BMI compared with patients without diabetes (p<0.001). The BMI was similar for patients with new-onset diabetes attributed to ADT when compared with those with preexisting diabetes (p=0.27) and men without diabetes (p=0.77). The study also used univariate and multivariate logistical regression analysis to assess risk factors for worsening glycemic control. Univariate analysis identified Caucasian race as predictive of developing a 10% or greater increase in mean hemoglobin A1c during ADT. Multivariate analysis did not identify a relationship with fasting blood glucose level and age, race-ethnicity, BMI, pretreatment PSA level, castration schedule (continuous or intermittent), vitamin D supplementation, or bisphosphonate administration. The observational study evaluated the association of ADT with treatment-emergent diabetes in 73,196 Medicare patients with a diagnosis of locoregional prostate cancer from 1992–1999 with documented follow-up through 2001.[27] Androgen deprivation therapy consisted of an LHRH agonist and bilateral orchiectomy for 36.9% and 6.9% of the men, respectively. The remaining 56.2% of the population studied did not receive ADT. Duration of ADT was reported as the percentage of time from diagnosis of prostate cancer until censoring (completion of data collection for that subject) that the patient was receiving treatment: the average duration of ADT was 40% for men receiving an LHRH agonist and 76.3% for men undergoing surgical castration. All patients in this analysis were at least 66 years old. For the entire study cohort, 12% had preexisting diabetes and these patients were not included in the statistical analysis evaluating the rate or prevalence of treatment-emergent diabetes. After the diagnosis of prostate cancer, diabetes developed in 10.9% of men without a preexisting diagnosis for this condition. When evaluated as number of events/1000 patient-years, a significantly greater rate of treatment-emergent diabetes occurred in men treated with an LHRH agonist (p<0.001) or surgical castration (p=0.005) compared with men not treated with ADT. The increased risk of ADT-related diabetes remained significant when analyzed by using Cox proportional hazards modeling to adjust for patient-and prostate cancer–related characteristics, including age; race-ethnicity; marital status; residence; Surveillance, Epidemiology, and End Results (SEER) program region; income; education level; tumor grade; comorbidity score; year of diagnosis; and primary surgical therapy. (The SEER program is the epidemiologic arm of the National Cancer Institute.) For men receiving an LHRH agonist, the increased risk of diabetes was evident within 1–4 months of beginning the drug, and the risk remained elevated throughout the duration of therapy. Cardiovascular Disease The aforementioned observational study that evaluated the association of ADT with treatment-emergent diabetes in 73,196 Medicare patients with a diagnosis of locoregional prostate cancer also evaluated the risk of treatment-associated cardiovascular disease in this population.[27] Coronary artery disease developed in 25.3% of men without a preexisting diagnosis of this condition after the diagnosis of prostate cancer. In addition, 5.4% of the population studied had an acute myocardial infarction and 4.5% experienced sudden cardiac death. When evaluated as number of events/1000 patient-years, men treated with an LHRH agonist had a significantly greater rate of treatment-associated CAD (p<0.001), myocardial infarction (p<0.001), and sudden cardiac death (p<0.001) than men not treated with ADT. Moreover, men who underwent bilateral orchiectomy also had a significantly greater rate of treatment-associated myocardial infarction (p=0.01) and sudden cardiac death (p<0.001) than men not treated with ADT. Using Cox proportional hazards modeling to adjust for patient-and prostate cancer– related characteristics, the study identified an association between LHRH agonist administration and a significantly increased risk of developing CAD, myocardial infarction, and sudden cardiac death ( Table 3 ).[27] Bilateral orchiectomy was not associated with a significantly increased risk of CAD, myocardial infarction, or sudden cardiac death ( Table 3 ). However, the low percentage of men (6.9%) undergoing orchiectomy may have hindered identification of a statistically significant relationship between this method of ADT and heart disease. The increased risk of CAD (p<0.001) was evident within 1–4 months of beginning LHRH agonist administration, and it remained elevated throughout the duration of therapy. The rates of myocardial infarction and cardiac sudden death increased with a similar time course relative to initiation of treatment with an LHRH agonist; however, the findings were not significantly different over the duration of therapy. Preexisting CAD was reported in 18% of the entire cohort, and these patients were not included in the statistical analysis evaluating the rate or prevalence of treatment-associated CAD. Another study reported that as little as 3 months of LHRH agonist administration with or without an androgen-blocking agent was associated with a shorter time period to fatal myocardial infarction for men aged 65 years or older with localized and locally advanced prostate cancer compared with matched cohorts not receiving ADT.[28] (Prostate cancer is defined as locally advanced when there is a growth extension outside the prostate capsule, possibly involving neighboring organs such as the bladder or rectum.) The study population consisted of 1372 men enrolled in three different multicenter, prospective, randomized clinical trials conducted in Australia, New Zealand, Canada, and the United States from February 1995–June 2001. Study subjects were randomly assigned to receive radiation therapy with ADT for 0 versus 3 versus 6 months (802 men), or 3 versus 8 months (364 men), or 0 versus 6 months (206 men). The treatment groups were well matched in terms of risk factors for CAD. The analysis pooled database information for men assigned to receive the same or similar treatments. Overall, acute myocardial infarction occurred in 29 (3.6%) of 802, 6 (1.6%) of 364, and 16 (7.8%) of 206 men. The time to fatal myocardial infarction was significantly shorter for men aged 65 years or older who received ADT compared with men of the same age group who did not receive ADT (p=0.017; Figure 1A). In addition, time to fatal myocardial infarction was significantly shorter for men aged 65 years or older who received ADT compared with men younger than 65 years who also received ADT (p=0.016; Figure 1B). The duration of ADT was not significantly associated with time to fatal myocardial infarction. Figure 1. (click image to zoom) Time to fatal myocardial infarction was significantly shorter in men aged 65 years or older who received androgen deprivation therapy (ADT) compared with men in the same age group who did not receive ADT (p=0.017; panel A) and men younger than 65 years who also received ADT (p=0.016; panel B). (From reference 28.) A 20% increase in the risk of serious cardiovascular morbidity attributed to medical ADT was reported in a retrospective analysis of 22,816 men with newly diagnosed prostate cancer.[29] Subjects were identified from the SEER registry database and consisted of men with prostate cancer diagnosed from 1992–1996. Medicare claims were reviewed to identify cardiovascular events and morbidity. The methodology did not capture data for obesity and tobacco use. Men were excluded from the analysis for any cardiovascular events or death from any cause that occurred within 12 months after their prostate cancer diagnosis. The study did not include patients treated with surgical ADT. Most men (87%) had locoregional disease, metastatic disease was diagnosed in 2%, and disease stages were unknown in 11%. The ADT and control cohorts had 4810 (21%) and 18,006 (79%) men, respectively. The mean duration that patients received ADT was 21 months. Of note, medical ADT was started more often in older men (≥ 80 yrs) and non-Caucasian men (p<0.0001). Men with metastatic prostate cancer were more likely to begin ADT at the time of diagnosis (p<0.001). The ADT cohort included more patients with a history of a cardiovascular event within 12 months preceding the prostate cancer diagnosis (p<0.001). Not surprisingly, these patients were more likely to experience a cardiovascular event 12–60 months after starting ADT (p<0.001). The findings of hypertension (20% vs 17%, p<0.001) and diabetes (7% vs 5%, p=0.021) were more prevalent in the ADT group versus the control cohort. Multivariate analysis established that several clinical and demographic factors were associated with cardiovascular morbidity.[29] Administration of ADT was associated with a 1.2-fold risk of cardiovascular morbidity after controlling for age, prostate cancer stage and grade, race-ethnicity, comorbidity score, history of pretreatment cardiac disease, treatment type, socioeconomic status, and geographic location. The increased risk of cardiovascular disease was greatest in men treated with ADT for 12 months or less compared with men receiving ADT for more than 12 months (hazard ratio 1.37, 95% confidence interval 1.29–1.46), which suggests that physiologic changes increasing the risk of cardiovascular disease occurred rather suddenly with initiation of ADT. This is consistent with the finding that changes in body composition, arterial stiffness, glycemic control, and lipid profiles occur within a few months of starting ADT.[24,25,27,30] Additional factors associated with an increased risk of cardiovascular morbidity in the ADT cohort included older age at diagnosis of prostate cancer; residing in Detroit, Michigan; previous external beam radiation therapy; and preexisting comorbidities.[29] Lower risk of cardiovascular morbidity was associated with Hispanic ethnicity and history of radical prostatectomy. The authors reported a significant relationship between residing in Detroit and African-American race; however, the cardiovascular risk of African-American men in Detroit was similar to that of Hispanic men and less than that of Caucasian men. Moreover, access to medical care was presumably similar for all groups because they were identified through Medicare claims. The effect of ADT on blood pressure is not consistent among studies. One prospective study reported similar blood pressure measurements at baseline and after 12 months of leuprolide therapy in 26 men with recurrent or locally advanced prostate cancer.[19] In this study, mean ± SD systolic and diastolic blood pressure measurements were 138 ± 4 and 78 ± 2 mm Hg, respectively, at baseline compared with mean ± SD systolic and diastolic blood pressure measurements of 134 ± 4 and 77 ± 2 mm Hg at the 12-month physical examination. In addition, a previously mentioned cross-sectional study comparing 20 men undergoing ADT for at least 12 months, 18 age-matched patients with prostate cancer without previous or current ADT, and 20 age-matched male controls found that metabolic syndrome was more prevalent in men undergoing treatment with ADT (p=0.03); however, hypertension was a less prominent component (p=0.53) of the condition than increased waist circumference (p=0.007), elevated fasting blood glucose level (o=0.006), and hypertriglyceridemia (p=0.06).[21] In contrast, the retrospective study evaluating risk of serious cardiovascular morbidity and ADT in 22,816 men with newly diagnosed prostate cancer from the SEER registry database report identified more cases of hypertension in the ADT group compared with the control cohort (p<0.001).[29] Reduced Testosterone Levels The association of ADT with endocrine and cardiovascular disease is supported by a link between decreasing endogenous testosterone concentrations and the development of metabolic syndrome, diabetes, and CAD that was previously established in aging males without a diagnosis of prostate cancer. Reductions in serum testosterone, sex hormone– binding globulin (SHBG), and the testosterone precursor dihydroepiandrosterone sulfate are associated with increasing waist circumference, hypertriglyceridemia, reduced HDL level, increased fasting serum glucose, and hypertension in independently living middleaged and elderly men.[31,32] A cross-sectional study of 400 independently living men aged 40–80 years reported that serum concentrations of testosterone and SHBG were related to insulin sensitivity after adjustment for body composition, fasting serum insulin levels, age, smoking (selfreported), alcohol consumption (self-reported), and physical activity score.[32] Moreover, the risk of metabolic syndrome or diabetes was increased 1.5–2-fold in middle-aged and elderly men with low levels of serum testosterone and SHBG.[33,34] An evaluation of 504 nonsmoking men (mean ± SD age 69.7 ± 7.3 yrs) found that the risk of severe atherosclerosis was over 2-fold greater for men with testosterone and SHBG levels in the lowest tertile.[35] In this study, atherosclerosis was measured radiographically in the abdominal aorta. Similar findings were described in 34 men undergoing cardiac catheterization for chest pain or an abnormal stress test.[36] The men were selected from 55 consecutive male patients, with exclusion of those having major preexisting medical conditions or markedly outlying serum testosterone levels. After controlling for age and BMI, there was an inverse correlation between serum testosterone levels and the extent of CAD. A link between hypotestosteronism and development of metabolic syndrome, diabetes, and CAD is also supported by the discovery that the endocrine and proartherogenic effects attributed to reduced endogenous testosterone can be reversed with exogenous testosterone therapy.[37–40] However, exogenous testosterone administration is not considered an option for men with prostate cancer because of the risk of promoting cancer growth and disease progression. An association between reduced testosterone levels and development of the body composition and physiologic changes characteristic of metabolic syndrome, diabetes, and CAD is well documented clinically.[41,42] However, the underlying biochemical relationship is not fully elucidated. One manner in which testosterone influences male body composition is through receptor-mediated stimulation of lipolysis in adipocytes.[42] A link between testosterone and vascular function is suggested by the finding of androgen receptors and androgen-responsive receptors in human arterial vessels, and in cultivated vascular smooth muscle cells, endothelial cells, macrophages, megakaryocytes, and platelets.[42,43] Notably, macrophages derived from healthy human donor monocytes by one investigator expressed androgen receptors in a sex-specific manner. The amount of messenger RNA for androgen receptor was 4-fold greater in cells from male versus those from female donors.[44] In addition, the activity of adenosine 5 ′-triphosphate– sensitive, voltage-dependent, calcium-activated, and potassium-activated vascular membrane channels is modulated by testosterone in vitro.[42,45,46] Physiologic concentrations of testosterone in vitro seem to promote fibrinolysis and anticoagulation by stimulating release of tissue plasminogen activator and tissue factor pathway inhibitor from human umbilical vein endothelial cells. Inhibition of plasminogen activator type 1 was demonstrated in the same experimental system.[47] Management of Reduced Physical Function Morbidity in men with prostate cancer can be exacerbated by reduced physical function attributed to long-term use of ADT.[48] Treatmentrelated reduction in BMD and increased adiposity underlie some of this effect.[17,48,49] Loss of BMD, osteopenia, and osteomalacia occur secondary to ADT and metastatic prostate cancer affecting the skeletal system.[17,50–53] Physical conditioning can improve physical strength, endurance, and quality of life for men with prostate cancer receiving ADT.[54,55] A 12-week course of resistance training reduced fatigue (p=0.002) and improved quality of life (p=0.001) for 82 men beginning treatment with ADT compared with a similar group of 73 men beginning ADT who were on a waiting list to undergo the same course of physical therapy.[54] The resistance training also resulted in increased upper (p=0.009) and lower (p<0.001) body strength. These findings are supported by the demonstration of significantly increased muscle strength (upper and lower body) and endurance (p<0.001) after a 20-week course of progressive resistance training for 10 men with localized prostate cancer who were actively undergoing long-term ADT.[55] For subjects in both of the aforementioned studies, resistance training increased muscle thicManagement of Risk Factors for Cardiovascular Disease Clearly, use of ADT for the treatment of prostate cancer provides the double-edged sword of offering anticancer treatment with the increased likelihood of metabolic syndrome and cardiovascular disease in a population already at risk for these health problems. All middle-aged and elderly persons should undergo routine monitoring of plasma lipid profiles, glucose tolerance, and blood pressure to detect metabolic syndrome and cardiovascular disease, which must be managed aggressively when identified by using all available appropriate diagnostic and therapeutic interventions, as well as adoption of healthy lifestyle practices.[1,56] It is imperative to recognize that the paradigm for reduction of cardiovascular morbidity and mortality does not change for men with the diagnosis of prostate cancer because most patients with prostate cancer live to the usual life expectancy for men in the Unites States and are more likely to die from complications of heart disease than from their cancer.[3,4,57] As the gatekeepers and guardians of pharmaceutical care, pharmacists are in an ideal position to identify men undergoing treatment with ADT who are at risk for or diagnosed with metabolic syndrome, diabetes, and CAD. Most of the related risk factors can be reduced by healthy lifestyle practices and compliance with drug therapy ( Table 4 ). At the start of ADT, fasting glucose levels or an oral glucose tolerance test and lipid profile should be evaluated. These tests should be repeated every 3 months during the first year of ADT because the adverse treatment-related endocrinologic and biochemical changes tend to develop within the first few months of therapy.[16,23,27,58] After the first year of ADT, laboratory monitoring should be done as appropriate for the patient's endocrinologic and cardiovascular health. It is also important to consider the duration of androgen suppression after discontinuation of therapy when monitoring patients for adverse drug effects. The duration of LHRH analog–induced hypotestosteronism may persist for many months after the end of the standard dosing interval.[59] kness while lean body mass was preserved and adiposity was not reduced.[54,55] Conclusion Long-term administration of ADT for the treatment of prostate cancer increases the risk of metabolic syndrome, diabetes, and CAD. Pharmacists should provide counseling to these patients on primary disease prevention. Men, especially those with preexisting cardiovascular disease, should be counseled on the endocrine and cardiovascular risks of ADT. Those undergoing treatment with ADT should be monitored routinely for signs and symptoms of metabolic syndrome, diabetes, and CAD. These diseases must be handled in an appropriate and aggressive manner when identified. All men undergoing treatment with ADT for prostate cancer should be encouraged to adopt healthy lifestyle practices, such as smoking cessation, weight reduction, and regular exercise. Men with metabolic syndrome, diabetes, and CAD who are managed with drug therapy should be encouraged to practice strict drug compliance. Physical therapy should be considered as warranted by the patient's baseline physical condition and level of activity. ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ