Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
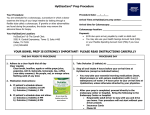
CHAPTER 7 OBSTETRICS, GYNAECOLOGY, AND URINARY-TRACT DISORDERS First line drugs – drugs recommended in both primary and secondary care Second line drugs – alternatives (often in specific conditions) in both primary and secondary care Specialist drugs – Drugs where specialist input is needed (see introduction for definition) Specialist only drugs – prescribing within specialist service only Notes: SLS Prescribing some drugs in this chapter on FP10 prescription is controlled by the Selective List Scheme (SLS). Drugs affected are highlighted and the explanatory notes provide further guidance. Doctors within secondary care are asked not to ask GPs to prescribe drugs outside of the controls imposed by SLS. Page: 7.1 7.2 7.3 7.4 Date 01.11 03.11 05.12 07.12 03.13 10.13 06.14 11.14 03.15 Revision 7.4.4 Deletion and revision 7.4.2 Section review. 7.4.5 Section review 7.4.2 Minor amendment 7.3 Section review 7.2.1 Strength discontinuation and addition 7.4.2 (NICE clinical guidelines)(NICE guidelines) 7.3.2 (Minor amendment) 7.3 (NICE guidance),7.3.2 (Drug addition), 7.4.1 (Drug addition) 7.4.2 (Section review) 7.4.5 (Section review) 07.15 01.17 7.4.2 (minor amendment) 7.3.2 (drug addition) First line drugs 2 Drugs used in obstetrics Treatment of vaginal and vulval conditions Contraceptives Drugs for genito-urinary disorders Second line drugs Specialist drugs Page 1 of 14 3 4 11 Contributor G Ells S Tyler-Murphy, G Ells G Ells J Percival, G Ells A Luck G Ells G Ells G Ells J Moore, F Kapasi, S TylerMurphy, G Ells G Ells G Ells Specialist only drugs 7.1 Drugs used in obstetrics 7.1.1 Prostaglandins and oxytocics Induction and augmentation of labour: Oxytocin Injection 10 units in 1 ml Dinoprostone Vaginal tablets 3 mg Misoprostol Tablets 200mcg Note: 1. Misoprostol is unlicenced in the induction of labour, but evidence supports its use. It is cheaper than gemeprost. 2. Oxytocin should be used in standard dilutions of 10 units/500ml (infusing 3ml/hour delivers 0.001 unit/minute) or, for higher doses, 30 units/500ml (infusing 1ml/hour delivers 0.001 unit/minute) NICE CG70 Induction of Labour (June 2008) Prevention and treatment of haemorrhage: Ergometrine and oxytocin (Syntometrine®) Injection containing ergometrine maleate 500 micrograms and oxytocin 5 units in 1 ml Ergometrine Injection 500 micrograms in 1 ml Carboprost Injection 250 micrograms in 1 ml Note: Carboprost is only indicated for postpartum haemorrhage due to uterine atony in patients unresponsive to ergometrine and oxytocin. 7.1.1.1 Ductus arteriosus Alprostadil Injection 500 micrograms in 1 ml for intravenous infusion Injection 1 mg vials Tablets 200 mg (maintenance of patency) Indometacin (closure of ductus arteriosus) 7.1.2 Mifepristone Mifepristone Note: Mifepristone is available as 200mg tablets. For each indication, 600mg (3 tablets) mifepristone should be given as a single dose. 7.1.3 Myometrial relaxants Atosiban Injection 7.5mg / ml (6.75mg/0.9ml vial) Terbutaline Injection 500micrograms / ml Notes: 1. Please refer to ESHT guidelines on Pre-term labour – Tocolysis. 2. Nifedipine (unlicensed indication, please refer to Chapter 2) has been shown to be effective in suppressing pre-term labour with minimal maternal and foetal side effects. It should be the first line tocolytic agent. 3. Oral ritodrine therapy is no longer considered to be superior to simple placebo and has no role in the treatment of premature labour. 4. Dexamethasone and indometacin (both unlicensed) can also be used to prevent pre-term labour in certain situations. First line drugs Second line drugs Specialist drugs Page 2 of 14 Specialist only drugs 7.2 Treatment of vaginal and vulval conditions 7.2.1 Preparations for vaginal atrophy Estriol (Ortho-Gynest®) Intravaginal cream containing 0.01% estriol Pessaries containing 500micrograms estriol Estriol (Ovestin®) Intravaginal cream containing 0.1% estriol Estradiol (Vagifem®) Vaginal tablet containing 10 micrograms of estradiol Estradiol (Estring®) Vaginal ring releasing estradiol approx. 7.5 microgram / 24 hours 25mcg discontinued 1. Estriol is preferred as there is thought to be less systemic effects. 2. If a topical oestrogen is to be used long-term consider co-prescribing an oral progestogen for 10-14 days each month to combat endometrial hyperplasia. Please refer to the Summary of Product Characteristics for individual drugs 7.2.2 Anti-infective drugs Fungal infections Clotrimazole 1% cream 20 g 10% vaginal cream 5 g 500 mg pessary Econazole 1% cream 15 g 150 mg pessary 1. The East Sussex Health Economy Medicines Committee “Management of Infection Guidance for Primary Care and Non-Acute Community Settings” (January 2006) recommends a single dose of clotrimazole (5g vaginal cream or 500mg pessary) for candidiasis. 2. With recurrent infections consider treating sexual partner(s) plus use of oral fluconazole 150 mg stat (not in pregnancy or breast feeding) 3. Econazole is included as an alternative topical anti fungal where patients may be sensitive to clotrimazole. 4. Patients should be advised that clotrimazole and econazole products might damage latex condoms and diaphragms. 5. Combination packs containing both vaginal and topical preparations are not recommended. Other infections Metronidazole Tablets 200mg, 500mg Vaginal gel 0.75% Clindamycin Cream, 2% Notes: 1. The East Sussex Health Economy Medicines Committee “Management of Infection Guidance for Primary Care and Non-Acute Community Settings” (January 2006 ) recommends metronidazole 2g in one dose or 400mg bd for 7 days for the treatment of bacterial vaginosis. 2. In pregnancy, metronidazole 400mg twice a day for 7 days or 0.75% vaginal gel 5g applicator at night for 5 nights is recommended. 3. Clindamycin cream is included as an alternative to metronidazole. 4. For trichomonas vaginalis infections, the East Sussex Health Economy Medicines Committee “Management Of Infection Guidance For Primary Care And Non-Acute Community Settings” (January 2006) recommends treating sexual partners concurrently and investigating for other sexually transmitted infections. Metronidazole 2g stat or 400mg twice a day for 7 days is recommended. In pregnancy use metronidazole 400mg twice a day for 7 days or clotrimazole 100mg pessary at night for 6 nights for symptomatic relief and treat post-natally. First line drugs Second line drugs Specialist drugs Page 3 of 14 Specialist only drugs 7.3 Contraceptives Prescribers are referred to Contraception - Your questions answered (5th edition) by John Guillebaud and the UKMEC 2009 Guidelines for further information. The following table provides a guide to the first-year (sterilisation rates are lifetime failure rates) user-failure rates per 100 women for different methods of contraception. Range in world literature (excludes atypical studies and all extended-use studies) Sterilisation Male (after azoospermia) Female 0 – 0.05 0 – 0.5 Subcutaneous implant Nexplanon® Injectable depot medroxyprogesterone acetate Combined pills 50 microgram oestrogen < 50 microgram oestrogen Progestogen only pill IUD Levonorgestrel IUD-20 (Mirena®) Multiload Cu 375®, TT 380 Slimline®, Neosafe T® Nova-T380® 0 – 0.07 0–1 0.1 – 3 0.2 – 3 0.3 – 4 0.1 – 0.2 0.2 – 1 0.6 4 – 20 2 – 15 5 – 15 6 – 17 4 – 25 2 – 25 6-? 80 – 90 40 – 50 10 – 20 0–5 Diaphragm (Male) condom Female condom Coitus interruptus Spermicides alone Fertility awareness ‘Persona’® No method, young women No method at age 40 No method at age 45 No method at age 50 (if still having menses) It is often preferable to start contraception as soon as it is requested. Guidance for doing this can be found at: FSRH Clinical Guidelines: Quick Starting Contraception (Sept 2010) Method Circumstances (day of menstrual cycle/ method of emergency contraception Requirements for additional contraception COCs Day 1-5 Not required Day 6 onwards/ quick start after POEC 7 days Quick start after UPA EC 14 days Combined vaginal ring Day 1 Not required Combined transdermal patch Day 2 onwards/ quick start after POEC 7 days Quick start after UPA EC 14 days Day 1-5 Not required Day 6 onwards/ quick start after POEC 2 days Quick start after UPA EC 9 days Day 1-5 Not required Day 6 onwards/ quick start after POEC 7 days Quick start after UPA EC 14 days Levonorgestrel releasing intrauterine system Day 1-7 Not required Day 8 onwards 7 days Copper bearing IUI Any start day Not required POPs Progestogen only implant and Injectable progestogen POEC = Progestogen only emergency contraception UPA = Ulipristal Acetate NB: Advice may be different for products not listed on the formulary First line drugs Second line drugs Specialist drugs Page 4 of 14 Specialist only drugs For detailed guidance on switching between products see Summary of Product Characteristics for individual products or the FSRH website. Switching TO… FROM… Combined hormonal contraceptive (CHC) Progestogen-only-Pills ( POP) When to start Combined Oral Contraceptive (COC) Combined Transdermal Patch (CTP) Combined Vaginal Ring (CVR) Instant switch after last active COC/ CTP/CVR No Progestogen only Pill (POP) Immediately No CHC Immediately if previous method used consistently and correctly POP Parenteral progestogenonly contraceptive, Progestogen implant, desogestrel only pill CHC Levonorgestrel releasing intrauterine system (LNGIUS) CHC Anytime up to when injection is due/ implant is removed/ last pill taken When injection is due. Immediately for implant/ pill Immediately if previous method used consistently and correctly POP initiation at time of IUS removal POP POP Copper bearing IUD Extra Precautions? CHC Up to day 5 of menstrual cycle Any other time POP At time of IUD removal 2 days before IUD removal Yes 7 days No No Yes 7 days Yes 2 days No Yes 7 days Yes 2 days No 7.3.1 Combined Hormonal Contraceptives (CHCs) To avoid confusion, it is advisable to prescribe CHCs by brand name. In order to establish the safety of combined hormonal contraception it is necessary to have an overview of the health status of the individual woman before first prescription of a CHC:Clinical history – contra-indications (see tables below) and conditions for which non-contraceptive benefits of CHCs may be helpful e.g. menorrhagia Clinical examination – Measure and record blood pressure Calculate Body Mass Index (BMI) where obesity is a concern Blood tests are unnecessary unless there is a clinical indication Breast and pelvic examinations are unnecessary in asymptomatic women UKMEC 2009 Guidelines are the definitive source of information regarding risk factors for CHCs. This list is not exhaustive. For more comprehensive information refer to the UKMEC 2009 guidelines There are 4 categories which define the degree of risk associated with COCs and specific risk factors (see below) UKMEC DEFINITION OF CATEGORY CATEGORY 1 A condition for which there is no restriction for the use of the contraceptive method CATEGORY 2 A condition where the advantages of using the method generally outweigh the theoretical or proven risks CATEGORY 3 A condition where the theoretical or proven risks generally outweigh the advantages of using the method. The provision of a method requires expert clinical judgement and/or referral to a specialist contraceptive provider, since use of the method is not usually recommended unless other more appropriate methods are not available or not acceptable CATEGORY 4 A condition which represents an unacceptable health risk if the contraceptive method is used First line drugs Second line drugs Specialist drugs Page 5 of 14 Specialist only drugs RISK FACTORS FOR VENOUS THROMBOEMBOLISM (VTE) Risk factor Category 4 Category 3 Category 2 Family history 1st 1st degree relative ≥ 45 Overweight (high body mass index) BMI ≥35 Immobility Confined to bed/ Wheelchair life degree relative < 45 BMI 30 - 34 Notes 1. A single category 2 risk factor indicates use of any pill if COC used. 2. Synergism - more than one category 2 risk factor elevates the overall risk to category 4 also if a risk factor is combined with age > 35. 3. Smoking appears to be a significant risk factor in VTE, resulting in a doubling of risk, which is similar in risk to that found for a BMI 30-34. 4. There are also important acute venous thromboembolism risk factors which need to be considered in individual cases: notably long-haul aeroplane flights, dehydration through any cause and recent SCUBA diving. RISK FACTORS FOR ARTERIAL CARDIOVASCULAR SYSTEM DISEASE Risk factor Category 4 Family history Cigarette smoking Diabetes mellitus (DM) Hypertension ≥ 35years AND ≥ 15 cigarettes/ day diabetic complications present (e.g. retinopathy, renal damage) Consistently elevated BP ≥ 160/95 mmHg on repeated testing Overweight Migraine With aura at any age Category 3 Category 2 Known hyperlipidaemias Known hyperlipidaemias ≥ 35years AND ≤ 15 cigarettes/day diabetic complications present (e.g. retinopathy, renal damage) < 35 years Stop COC at 35 if still smoking Non vascular disease IDDM NIDDM Category will depend on severity of complications Remarks Category will depend on degree of severity and presence of other CV risk factors Adequately controlled Consistently elevated BP 140-159 / 90-94 BMI > 35 BMI 30 – 34 Migraine without aura at any age – continuing when patient develops the condition Migraine without aura at any age – starting when patient already has the condition Flashing lights not classified as aura Notes: 1. Synergism: if more than one category 2 factor applies; or if one category 2 factor and the woman is now above the age of 35, do not use CHC. 2. Refer to the BNF for information on: Diarrhoea and vomiting Drug interactions Reason to stop immediately Dosing instructions 3. See link for latest Missed pill recommendations The risk of venous thromboembolism in women is estimated to be: (Drug Safety Update Volume 3, Issue 9 April 2010) Not pregnant women, not taking an oral contraceptive Using “second generation” COCs Using “third generation” COCs Pregnant 5-10 cases per 100,000 15 cases per 100,000 25 cases per 100,000 60 cases per 100,000 All currently available low doses CHCs carry an extremely low risk for healthy women. Oestrogen – CHCs containing 50 micrograms or more of oestrogens are associated with a larger relative risk of ischaemic stroke that those with lower doses. First line drugs Second line drugs Specialist drugs Page 6 of 14 Specialist only drugs CHCs containing no more than 35 micrograms ethinylestradiol plus no more than 1 mg norethisterone or 150 micrograms levonorgestrel are recommended as first-line agents Choosing a Combined Oral Contraceptive (COC) There are several brands of COCs marketed with identical ingredients but varying in price. The following products have been included in the formulary based on current prescribing patterns and cost. It is NOT recommended that brands are switched. 1st generation 2nd generation 3rd generation 4th generation norethisterone (e.g. Loestrin®) Levonorgestrel (e.g. Microgynon 30®) Desogestrel (e.g. Mercilon®) drospirenone Gestodene (e.g. Femodette®) dienogest etynodiol diacetate (only in progestogen-only pill) norgestimate (e.g.Cilest®) Classification of progestogens (Mansour D. Use of the new progestogens in contraception and gynaecology. The Obstetrician & Gynaecologist 2006;8:229–34) Second-line choices of COCs: Problem: Consider: Where a patient complains of progestogenic sideeffects such as depression, sustained weight gain, loss of libido A more oestrogen dominant COC e.g. Ovysmen® Marvelon® If a woman will not tolerate a norethisterone or levonorgestrel COC because of “minor” sideeffects such as breakthrough bleeding, acne, headaches, depression, weight gain, breast symptoms or wants a change for personal reasons. A different progestogen e.g. desogestrel or gestodene containing pill. However, it is important that the woman accepts the possible increased risk of venous thromboembolism, backed up with an upto-date leaflet. The Family Planning Association produce a suitable leaflet (The combined pill). A woman complains of oestrogenic side effects such as nausea, bloating, breast tenderness or cyclical weight gain. 1. “Low strength” oestrogen formulation e.g. Loestrin 20® which may also be considered for older women where reduced metabolic effects due to oestrogen are required. Unfortunately, women taking low strength COCs have a higher incidence of breakthrough bleeding. 2, A more progestogen dominant COC e.g. Microgynon 30® The woman is taking a hepatic enzyme-inducing drug (e.g. some anti-epileptics). In a woman unable to use an alternative method of contraception, a combination of oral contraceptives to provide a daily intake of ethinylestradiol 50 micrograms or more [unlicensed use]; tricylcing is recommended. NB. Norinyl-1® contains 50 micrograms of mestranol. This is a pro-drug and only equates to 37.5-40 micrograms of ethinylestradiol. Triphasic pills e.g. Trinovum®, Logynon® Improved cycle control or patient preference. Severe acne in women refractory to prolonged antibiotic therapy. Some women with moderately severe hirsutism may also benefit, as hair growth is also androgen-dependent. First line drugs Dianette® - (see chapter 13) as it contains an anti-androgen. It is recommended that treatment be withdrawn 3 or 4 cycles after the indicated condition(s) has/have completely resolved and that Dianette® is not continued solely to provide oral contraception. Once acne has resolved the woman can be switched to a conventional COC with low androgenic tendencies e.g. Marvelon®. Note: When Dianette® is prescribed for contraceptive purposes the prescriber must mark the prescription ♀ otherwise a prescription charge must be paid by the patient. Second line drugs Specialist drugs Page 7 of 14 Specialist only drugs Low strength plus “second generation” progesterone Loestrin 20® Tablets containing ethinylestradiol 20 micrograms and norethisterone 1 mg Low strength plus “third generation” progesterone Femodette® Tablets containing ethinylestradiol 20 micrograms and gestodene 75 micrograms Mercilon® Tablets containing ethinylestradiol 20 micrograms and desogestrel 150 micrograms Standard strength plus “second generation” progesterone Microgynon 30® Tablets containing ethinylestradiol 30 micrograms and levonorgestrel 150 micrograms Cilest® Tablets containing ethinylestradiol 35 micrograms and norgestimate 250 micrograms Loestrin 30® Tablets containing ethinylestradiol 30 micrograms and norethisterone 1.5 mg Ovysmen® Tablets containing ethinylestradiol 35 micrograms and norethisterone 500 micrograms Triphasic preparations Logynon® Trinovum® 6 light brown tablets: ethinylestradiol 30 micrograms, levonorgestrel 50 micrograms; 5 white tablets: ethinylestradiol 40 micrograms, levonorgestrel 75 micrograms; 10 ochre tablets: ethinylestradiol 30 micrograms, levonorgestrel 125 micrograms 7 white tablets: ethinylestradiol 35 micrograms, norethisterone 500 micrograms; 7 light peach tablets: ethinylestradiol 35 micrograms, norethisterone 750 micrograms; 7 peach tablets: ethinylestradiol 35 micrograms, norethisterone 1 mg Standard strength plus “third generation” progesterone Femodene® Tablets containing ethinylestradiol 30 micrograms and gestodene 75 micrograms Marvelon® Tablets containing ethinylestradiol 30 micrograms and desogestrel 150 micrograms Standard strength transdermal patch EVRA® Patch releasing approx 34 micrograms ethinylestradiol and approx 203 micrograms norelgestromin per 24 hours Low strength vaginal ring NuvaRing® 1. 2. 3. 4. Ring releasing approx 15 micrograms ethinylestradiol and approx 120 micrograms etonorgestrel per 24 hours The patch is applied once a week for 3 weeks followed by a 7 day patch free interval Ring is inserted into the vagina and removed on day 22 followed by a 7 day ring free interval Both non oral formulations have similar effectiveness but cost significantly more than COCs The National Prescribing Centre recommends that the newer non oral CHCs should be reserved for women dissatisfied with oral formulations, particularly if compliance is a problem but remembering that there are other alternatives such as parenteral/ intra-uterine forms of contraception. 7.3.2 Progestogen-only contraceptives 7.3.2.1 Oral progestogen-only contraceptives Desogestrel Tablets 75 micrograms Femulen® Tablets containing etynodiol diacetate 500 micrograms First line drugs Second line drugs Specialist drugs Page 8 of 14 Specialist only drugs Micronor® Tablets containing norethisterone 350 micrograms Norgeston® Tablets containing levonorgestrel 30 micrograms 1. Desogestrel has been selected as the POP of first choice because it has a 12-hour safety period before failure to take is regarded as a “missed” pill. Other products are regarded as “missed” after only 3 hours. 2. Desogestrel is available as a generic product which is more cost effective than the branded version. As it is a single ingredient product available as a single strength only the risk of confusing this with other products is low hence it is acceptable to prescribe desogestrel generically. 3. On the limited evidence available progestogen-only pills (POPs) may be suitable for women who want to use an oral contraceptive but who have risk factors for cardiovascular complications with CHC, such as moderate to severe hypertension, diabetes, focal migraine, obesity, a history of venous thromboembolism or heavy smoking. However, these women will still need to be carefully screened and monitored. 4. POPs are also indicated during lactation. 5. If a women is experiencing bleeding problems or “minor” side-effects such as breast discomfort and acne an alternative progestogen may be tried as side-effects appear to depend on target-organ sensitivity. 7.3.2.2. Parenteral progestogen-only contraceptives Guidance on the use of Long-acting reversible contraceptives can be found at and NICE CG30 (September 2014) Medroxyprogesterone acetate Injection 150 mg in 1 ml for deep intramuscular injection every 12 weeks. Injection 104mg in 0.65ml for subcutaneous injection every 13 weeks (Depo-Provera®) Medroxyprogesterone acetate (Sayana Press®) 1. Guidance on quick-starting injectable contraceptives can be found at: FSRH Clinical Guidelines: Quick Starting Contraception (Sept 2010) 2. A woman should be counselled and the manufacturer’s leaflet given (with time to read it and any questions answered) before she decides on injectable contraception. This should cover: Amenorrhoea Frequent irregular bleeding patterns, particularly at outset. Weight gain – not inevitable as it is mainly caused by increased appetite. Delay in fertility return – on average it may take 9 months from the time of last injection to conceive. Theoretical long-term risks – the issues of arterial disease and osteoporosis, especially if there were to be prolonged amenorrhoea, are not fully resolved. Likely irregular bleeding pattern in the first six months, which may recur. 3. The interval between injections should be reduced from 12 to 10 weeks (8 weeks for a very potent inducer such as rifampicin) when an enzyme-inducing drug is also prescribed. Etonogestrel (Nexplanon®) 68 mg in each flexible rod for subdermal implantation 1. The practitioner fitting (or removing) Nexplanon® must be fully trained in the technique. 2. When the fitter is not the prescriber, the prescribing clinician has the responsibility to ensure that the fitter is competent in fitting the implant and has received appropriate training. 3. Guidance on quick-starting implants can be found at: FSRH Clinical Guidelines: Quick Starting Contraception (Sept 2010) 4. A woman should counselled and the manufacturer’s leaflet given (with time to read it and any questions answered) before she decides on an implant. Counselling should cover: Likely bleeding patterns over the first 6 months “Minor” progestogenic side effects e.g. acne, headache, breast pain, and mood changes. Local adverse effects at site of insertion. 5. Nexplanon® is licensed for 3 years. 6. Women prescribed enzyme-inducing drugs, for example, rifampicin, St. John’s Wort require additional precautions. 7. The PPA has classified Nexplanon® as an implant and not an injection. Therefore, for GP practices it will not be reimbursed as a personally administered item. First line drugs Second line drugs Specialist drugs Page 9 of 14 Specialist only drugs 7.3.2.3 Intra-uterine progestogen-only contraceptive Levonorgestrel (Mirena®) Intra-uterine system releasing 20 micrograms of levonorgestrel per 24 hours Levonorgestrel (Jaydess®) Intra-uterine system releasing 6 micrograms of levonorgestrel per 24 hours 1. Mirena® is a Nova T shaped device which releases levonorgestrel directly into the uterine cavity and is effective for 5 years (4 years when used with HRT). 2. Mirena® is licensed for use as a contraceptive and for the treatment of primary menorrhagia. It is effective as long as treating primary menorrhagia, if not used as a contraceptive. 3. Women who have Mirena® inserted at or after the age of 45 years and are amenorrhoeic may retain it until age 55 years. 4. Jaydess® is a smaller device than Mirena® releasing a lower dose of levonorgestrel per day into the uterine cavity and is effective for 3 years. 5. Jaydess® is particularly indicated for women wishing to have a LNG-IUS a. But with a uterus which is too small to accommodate the Mirena® device b. Wishing to review their family planning after 3 years 6. The effects of the intra-uterine systems are mainly local and hormonal including prevention of endometrial proliferation, thickening of cervical mucus, and suppression of ovulation in some women (in some cycles). Return of fertility after removal is rapid and appears to be complete. 7. Advantages of LNG-IUS over copper IUCDs are that there may be an improvement in any dysmenorrhoea and a reduction in blood loss. There is also evidence that the frequency of pelvic inflammatory disease may be reduced particularly in the youngest age groups who are most at risk. 8. When the fitter is not the prescriber, the prescribing clinician has the responsibility to ensure that the fitter is competent in fitting LNG-IUS and has received appropriate training. 9. A full list of counselling points can be found in the FSRH Clinical Guidance on Intrauterine Contraception (2007) Counselling should cover: Mode of action Efficacy Likely bleeding pattern over the first 6 months Possible progestogenic side-effects Risks associated with intrauterine device and its fitting 10. The PPA has classified Mirena® and Jaydess® as intra-uterine devices. Therefore, for GP practices, it will be reimbursed as a personally administered item 7.3.3 Spermicidal contraceptives Nonoxinol-‘9’ gel Gygel® Excipients include parabens, propylene glycol, sorbic acid 1. Spermicides are suitable for use with a barrier method(s) for added protection. They are not suitable for use alone for contraception except in exceptional circumstances. 2. There is no evidence of harm to latex condoms and diaphragms with nonoxinol–‘9’ 3. There is evidence of vaginal reactions with nonoxinol-‘9’ (N9) and thus increased risk of acquisition of sexually transmitted diseases. Therefore condoms are no longer manufactured with N9. 7.3.4 Contraceptive devices Fertility (Ovulation Thermometer) 1. Fertility thermometers are not an accurate method of detection without appropriate training. Therefore mercury thermometers have not been included in the formulary. The Natural Family Planning (NFP) technique can be effective if taught correctly by trained practitioners. 2. Digital thermometers are not included in the Drug Tariff and so cannot be prescribed on FP10. Intrauterine Contraceptive Devices (IUCDs) IUCDs are classed as appliances and only those listed in part IXA of the Drug Tariff can be prescribed and reimbursed in primary care. Mini TT 380® Slimline T-Safe ® 380A QuickLoad UT 380 Standard® Replacement every 10 years For uterine length over 5 cm Replacement every 10 years For uterine length over 6.5 - 9cm Replacement every 5 years For uterine length 6.5 - 9cm 1. IUCDs with a surface area of copper (Cu) less than 380 mm 2 are no longer recommended as they may be less effective. First line drugs Second line drugs Specialist drugs Page 10 of 14 Specialist only drugs Vaginal Contraceptive Caps and Diaphragms Caps and diaphragms are used infrequently. Advice on choice, prescription and fitting of caps and diaphragms should be obtained from a Specialist (primary or secondary care) in their use. Diaphragms are usually used. They are normally replaced annually, have expiry dates and are used with spermicides. Flat spring diaphragm (latex) Coil spring diaphragm (silicone) Arcing spring diaphragm (silicone) sizes 55 – 95 mm (rising in 5 mm) first choice sizes 60 – 90 mm (rising in 5 mm) sizes 60 – 90 mm (rising in 5 mm) Caps are used less often e.g. prolapse, poor muscle tone, urinary symptoms. They last longer than diaphragms, have expiry dates and are used with spermicides. Soft silicone cap (FemCap) available in sizes 22, 26, and 30 mm 7.3.5 Emergency hormonal contraception (EHC) Tablet 1.5mg Levonorgestrel (Levonelle® 1500) Ulipristal acetate (ellaOne®)▼ Tablet 30mg Note: 1. Levonelle® 1500 is licensed to prevent pregnancy when taken within 72 hours of unprotected intercourse. It is more effective the sooner it is taken after unprotected sex, preferably within 12 hours but no later than after 72 hours. 2. ellaOne® is a selective progesterone modulator (SPRM) licensed for emergency hormonal contraception up to 120 hours (5 days) after unprotected sex. 3. Levonorgestrel may be less effective than ulipristal at preventing pregnancy up to 72 hours after unprotected sex but levonorgestrel is significantly cheaper. 4. Ulipristal is more effective than levonorgestrel at preventing pregnancy between 72 and 120 hours after unprotected sex 5. Levonelle® One Step is available to purchase from Community Pharmacies only. It costs over twice as much when prescribed on FP10 than Levonelle® 1500. 6. Women should be encouraged to seek treatment as early as possible after unprotected sex and advised that treatment failure may occur. 7. Women who do not experience a normal period within 3 weeks of using EHC should be followed up so that pregnancy can be excluded. 8. The possibility of an ectopic pregnancy should be considered, particularly in women with a previous ectopic pregnancy, fallopian tube surgery or pelvic inflammatory disease. 9. A copper IUCD is more effective than levonorgestrel but its effectiveness compared to ulipristal is unknown. It can be inserted up to 5 days after unprotected sexual intercourse or up to 5 days after the earliest likely day of ovulation (i.e. before implantation). The IUCD can then be removed with the next period or left in situ for long-term contraception. 7.4 Drugs for genito-urinary disorders 7.4.1 Drugs for urinary retention Alpha-blockers Tamsulosin Modified release capsules 400 micrograms Alfuzosin Modified release tablets 10 mg Tamsulosin/solifenacin Vesomni® 400 micrograms/6mg modified release tablets First line drugs Second line drugs Specialist drugs Page 11 of 14 Specialist only drugs Notes: 1. All alpha-blockers are equally effective 2. Tamsulosin should be prescribed as capsules not tablets as the tablets are considerably more expensive and confer no added advantage 3. First dose of alfuzosin may cause collapse because of the hypotensive effect. 4. The combination product of an alpha-blocker and an anticholinergic may be used in men who still have storage symptoms after treatment with an alpha blocker alone (see NICE CG97 LUTS 2010). 5. Finasteride is included in Section 6.4.2. 7.4.2 Drugs for urinary frequency, enuresis and incontinence Tolterodine Tablets 2.5 mg, 5 mg Ditropan® Elixir 2.5mg in 5ml Tablets 1mg, 2mg Oxybutynin patches Kentera®Transdermal patches 36mg Mirabegron▼ Betmiga® Modified release tablets 25mg,50mg Fesoterodine Tovias® Modified release tablets 4mg, 8mg Solifenacin Vesicare® Tablets 5mg, 10mg Botulinum Toxin Type A Botox® Powder for reconstitution. Vial, 50 units, 100 units, 200 units Oxybutynin Notes: Accurate assessment and diagnosis of the cause of incontinence is vital for treatment success. Non-drug treatments have an important role in management. NICE CG 171. Urinary Incontinence in Women (September 2013) gives guidance on the treatment of urinary incontinence in women. NICE CG 148. Urinary incontinence in neurological disease (August 2012) gives guidance on the management of lower urinary tract dysfunction in neurological disease. NICE guidance (September 2013) confirms there is no evidence of a clinically important difference in efficacy between antimuscarinic drugs and immediate release non-proprietary oxybutynin or tolterodine are the most cost effective of the available options. Patients should be advised that the full benefit of treatment may not be evident for up to 4 weeks Mirabegron and fesoterodine are second line options if the first treatment for OAB or mixed UI is not effective or welltolerated. Oxybutynin (immediate release) should not be offered to frail older women Oxybutynin patches are an option for patients who have difficulty swallowing tablets Mirabegron has been approved by NICE for treating the symptoms of overactive bladder in patients who cannot tolerate antimuscarinic drugs or in whom they are contraindicated or ineffective see TA290 (June 2013). The standard dose is 50mg daily with the 25mg dose being reserved for patients with renal impairment (eGFR 15-29 ml/min/1.73m2). Botulinum toxin type A is a treatment option for patients with spinal cord disease who have symptoms of overactive bladder and where antimuscarinic treatment have been either ineffective or poorly tolerated (CG 148 August 2012) Botulinum toxin type A is a treatment option for women with OAB caused by proven detrusor overactivity that has not responded to conservative management (including OAB drug therapy) (CG 171 September 2013). For treatment of nocturnal enuresis, refer to Section 6.5.2 Other relevant NICE guidance: NICE CG97: LUTS (May 2010) 7.4.3 Drugs used in urological pain Potassium citrate mixture BP Oral solution “well diluted with water” Notes: 1. The discomfort of cystitis may be relieved by alkalinisation of urine with potassium citrate. 2. Ascorbic acid (for acidification of urine) has not been included as the BNF classifies it as “less suitable for prescribing”. The high doses that are required can lead to renal stones in those with hyperoxaluria. First line drugs Second line drugs Specialist drugs Page 12 of 14 Specialist only drugs 7.4.4 Bladder instillations and urological surgery Urological surgery Glucose 5% irrigation solution, 3 litre Sodium chloride 0.9% irrigation solution, 1 litre, 3 litre Maintenance of indwelling urinary catheters CATHETER MAINTENANCE SOLUTIONS These should be considered for short term use to treat indwelling catheters blocked by encrustation or on removal of the catheter to dissolve crystal formation. They should not be considered as an option for routine catheter maintenance. Getliffe et al (2000) suggest that two sequential instillations of a small volume are more effective than a single administration. Monitoring urine pH will help identify the need for, and the type of solution required. Citric acid should only be used for those patients who have a consistently high pH of 7.4 and above (Pomfret 1995). It is good practice to cut open catheters on removal, from those patients where blocking is problematic to see if the lumen is blocked by sediment deposit. B BRAUN URO-TAINER TWIN. The solution is divided into a twin delivery system allowing for two sequential administrations. ORDER CODE 9746609 PRODUCT PACK SIZE 10 Citric acid 3.23% Suby G - 2 x 30mls (prevent or dissolve urinary salts & encrustation) 9746625 10 Citric acid 6% Solution R - 2 x 30mls (should not be used for more than 2 weeks and only when 3.23% solution has failed) DRUG TARIFF PRICE £41.00 / £4.10 each £41.00 / £4.10 each 7.4.5 Drugs for Erectile Dysfunction (ED) Sildenafil Tablets 25mg, 50 mg, 100 mg (on demand dosing) Tablets 25mg daily (post radical prostatectomy only) Vardenafil SLS Levitra® Tablets 10mg, 20mg Tadalafil SLS Cialis® Tablets 10mg, 20mg (on demand dosing) Cialis® Tablets 2.5mg, 5mg (red when used post radical prostatectomy) Alprostadil SLS Caverject® Dual Chamber cartridge + diluent for intracavernosal injection 10 microgram, 20 microgram, powder + solvent for injection, 5 microgram, 10 microgram, 20 microgram, 40 microgram MUSE® 250 microgram, 500 microgram, 1000 microgram transurethral delivery system Vitaros® 3mg/g cream (300 micrograms per dose) 1. The drug treatment pathway for ED (see below) outlines prescribing choices for patients meeting the NHS criteria for prescribing in ED and the options for patients who do not. 2. Daily use of PDE5 inhibitors after laprascopic radical prostatectomy should be prescribed by ED specialists only. 3. HSC 1999/177 recommends that treatment for ED should be available from specialist services when it is causing severe distress. GPs can prescribe sildenafil for these patients but if this is ineffective or not tolerated, these patients should be referred into a specialist service who will then prescribe other ED treatments as necessary. GPs cannot issue an FP10, endorsed SLS, where treatment has been started by a specialist for a patient suffering severe distress unless they also meet one of the above criteria. 4. Vacuum Erection Devices (VEDs) are available to all patients with ED regardless of whether they meet NHS criteria for prescribing the drugs or not. Patients require specialist advice to help select the most appropriate product and instruct on its use, hence all patients considering a VED should be referred into the ED clinic. 5. A VED should be supplied to the patient by the ED clinic. Associated consumables can be prescribed in primary care. First line drugs Second line drugs Specialist drugs Page 13 of 14 Specialist only drugs Drug Treatment Pathway for Patients with Erectile Dysfunction (ED) Laprascopic Radical Prostatectomy (LRP) patients: Sildenafil 25mg daily (Tadalafil 2.5mg – 5mg daily) Patient has one or more of the following conditions (SLS criteria): OR OR Diabetes Multiple sclerosis Parkinson’s disease, Poliomyelitis Prostate cancer, Severe pelvic injury Single gene neurological disease Spina bifida Spinal cord injury; Specialist prescribing only Patients not meeting SLS criteria Prescribe generic sildenafil 50mg100mg on demand on FP10 prescription Is on dialysis for renal failure Prescribe sufficient for 1 treatment per week*. Has had any of the following surgery: Laproscopic Radical Prostatectomy Radical pelvic surgery Renal transplant. Dose can be reduced to 25mg if higher doses not tolerated OR Was receiving ED treatments on the th NHS on 14 September 1998 *A GP can prescribe more than one treatment per week if clinical judgement indicates this would be appropriate. Inadequate treatment outcome or sildenafil not tolerated Patients not meeting SLS criteria Patients meeting SLS criteria Private prescription for an alternative PDE5 inhibitor Vardenafil 10mg or 20mg on demand OR Tadalafil 10mg or 20mg on demand Prescribe sufficient for 1 treatment per $ week . Inadequate treatment outcome or not tolerated $ Tadalafil 2.5mg and 5mg daily doses should be reserved for patients who have responded to tadalafil on demand and where it is the GP’s clinical judgement that more than 2 treatments per week are indicated. FP10 forms must be endorsed SLS Refer to ED Clinic Alprostadil products – see formulary # Vacuum erection device (VED) # Vacuum pump devices are not subject to SLS restrictions and can be prescribed for anybody with ED on the NHS NHS REGULATIONS DO NOT ALLOW PRESCRIBING OF COMBINATIONS OF DRUG TREATMENTS First line drugs Second line drugs Specialist drugs Page 14 of 14 Specialist only drugs