Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Cardiac surgery wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
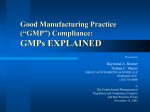
123 Mechanical Deformation of Vessel Wall and Shear Stress Determine the Basal Release of Endothelium-Derived Relaxing Factor in the Intact Rabbit Coronary Vascular Bed Daniel Lamontagne, Ulrich Pohl, and Rudi Busse Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 We investigated the mechanisms that are responsible for the basal release of endotheliumderived relaxing factor (EDRF), which is likely to be identical with nitric oxide, in the intact coronary circulation. The increase in cGMP content of platelets passing through the coronary bed of the isolated rabbit heart was used as an index of EDRF release. Platelet cGMP content after passage through the heart under control conditions (flow rate of 20 ml/min) amounted to 0.50±0.10 pmol/mg protein. Inhibition of endothelial nitric oxide synthesis by 30 ,uM NG-nitro-L-arginine (L-NNA) reduced this amount by more than 60%. Increasing flow rate from 20 ml/min to 40 and 60 ml/min led to flow-dependent dilation as reflected by the subsequent drop in perfusion pressure after an initial rise. The flow-dependent dilation was associated with a significant increase in the normalized platelet cGMP content. L-NNA abolished completely both the flow-dependent dilation and the increase in platelet cGMP content. Increasing shear stress by a strong vasoconstriction (1 nM endothelin-1) at constant flow was also accompanied by a 2.5-fold increase in platelet cGMP content. To investigate whether mechanical forces applied to the vascular wall by the myocardial contraction cycle were also a stimulus for EDRF release, cardiac arrest was induced by a continuous infusion of mepivacaine (final concentration, 0.02%). Under these conditions, a decrease in platelet cGMP content comparable to that after nitric oxide synthesis inhibition was observed in the arrested heart. The reappearance of mechanical activity after washout of mepivacaine was associated with the recovery of platelet guanylate cyclase activation, indicating the contribution of the mechanical activity on basal EDRF release. To study further the effects of wall deformation on EDRF release, experiments were performed in isolated saline-perfused rabbit arterial segments. Rhythmic squeezing of the segments led to a significant increase in EDRF release as assessed by assay of guanylate cyclase activity. These data indicate that at least two principles contribute to the basal agonistindependent release of EDRF in the intact coronary bed. Besides the continuously acting wall shear stress imposed by the streaming fluid, the periodic compression of intramyocardial vessels stimulates the formation of EDRF. This EDRF formation may result from the high shear stress imposed on the endothelial lining by the periodic diameter reduction and from the direct deformation of the endothelium. (Circulation Research 1992;70:123-130) The endothelium-derived relaxing factor (EDRF), which is likely to be identical with nitric oxide (NO),1,2 can be released after the action of several blood-borne agonists on their specific receptors.3 On the other hand, several studies From the Institute of Applied Physiology, University of Freiburg, Freiburg, FRG. Supported by a grant from the Deutsche Forschungsgemeinschaft (Bu 436/4-1 and 4-2). D.L. is a Research Fellow of the Heart and Stroke Foundation of Canada. Address for correspondence: Rudi Busse, Institut fiir Angewandte Physiologie, Hermann-Herder-Str. 7, D-7800 Freiburg, FRG. Received February 21, 1991; accepted September 16, 1991. support the concept that the intact coronary vascular bed is maintained under a constant dilating tone by a basal, agonist-independent release of EDRF. A significant amount of EDRF is released from the isolated guinea pig45 and rabbit6 heart without any agonist stimulation. Furthermore, inhibition of NO synthesis is accompanied by a considerable vasoconstriction in the coronary vascular bed of the isolated rabbit heart.7 8 However, the stimuli or mechanisms responsible for such a basal release of EDRF are still unclear. The release of EDRF can be stimulated by shear stress in isolated arterial segments9 and cultured 124 Circulation Research Vol 70, No 1 January 1992 Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 endothelial cells.10 Although the shear stress-induced release of EDRF in the intact coronary microcirculation has yet to be confirmed, the continuous shear stress imposed on the endothelial lining by the streaming fluid in the coronary vascular system could theoretically stimulate the basal, agonist-independent release of EDRF. Endothelial cells are also stimulated by the deformation of the vessel wall. For example, pulsatile flow, which is accompanied by rhythmic changes in vessel diameter, is a more potent stimulus of EDRF release than nonpulsatile flow.11 Since the coronary vascular bed is constantly exposed to the rhythmic compression and decompression associated with the contraction-relaxation cycle of the myocardium, the mechanical activity of the beating heart could also stimulate the release of EDRF, therefore contributing to the basal release of EDRF in this organ. This study was thus performed to assess the contribution of shear stress and the cardiac mechanical activity as stimuli for the basal, agonist-independent release of EDRF in the intact coronary vascular bed of the isolated rabbit heart. Materials and Methods Isolated Perfused Rabbit Hearts Mongrel rabbits (1.0-1.5 kg) of either sex were anesthetized with sodium pentobarbital (30-60 mg/kg i.v.). After anticoagulation with heparin (1,000 IU i.v.), the carotid artery was transected, and the heart was rapidly perfused in situ (Langendorff preparation) through a cannula inserted into the aortic stump. The heart was then excised and perfused at a constant flow rate by means of a roller pump (Heidolph RGL 85, Kelheim, FRG). Two compliance chambers along the perfusion line ensured a continuous flow. The perfusion solution consisted of a modified Krebs-Henseleit buffer containing (mM) NaCl 118, KCI 4, CaCI2 2.5, KH2PO4 1.2, MgSO4 1, NaHCO3 24, D-glucose 5, and pyruvate 2, dissolved in double-distilled water. The perfusate was gassed with 95% 02-5% CO2 (pH 7.4) and kept at a constant temperature of 37°C. Bolus doses of drugs and platelets were administered through a Y connector in the aortic perfusion line. Coronary perfusion pressure (CPP) was measured with a pressure transducer (model P2310, Gould, Oxnard, Calif.) connected to a side arm of the aortic perfusion cannula. Isovolumetric left ventricular pressure was measured by a fluidfilled latex balloon inserted into the left ventricle through a pulmonary vein and connected to a second pressure transducer (model CP-01, Gould). The volume of the balloon was adjusted to obtain a diastolic pressure between 5 and 10 mm Hg. Fluid that could enter the ventricle was drained by means of a vent in the apex of the left ventricle. Heart rate was derived from the left ventricular pressure signal by a cardiotachometer. The coronary effluent was collected from the coronary sinus and the right atrium. Passage through the right ventricle was prevented by destruc- tion of the atrioventricular and pulmonary valves and ligation of the pulmonary arterial trunk. Platelet Preparation Blood from healthy human donors (70-80 ml) who had not received any medication was collected in a 3.8% sodium citrate solution (10% of final volume). Platelet-rich plasma was obtained by centrifugation at 200g for 20 minutes. After addition of citric acid/sodium citrate/dextrose (20 vol%) and prostacyclin (75 pg/ml), the platelet-rich plasma was centrifuged again (800g), and the pellet was suspended in a modified HEPES-buffered Tyrode's solution containing indomethacin (10 ,uM) to obtain a final platelet count of 2-3 x 106 platelets/gl. Prostacyclin was eliminated from this suspension by a final 10-minute incubation at 37°C. Experimental Protocols The basic experimental protocol consisted of evaluating the cGMP increase in platelets passing through the coronary bed, as an index of luminally released EDRF, under unstimulated conditions and, 10 minutes later, during endothelial stimulation with 1 ,uM acetylcholine (ACh, Sigma Chemical Co., Deisenhofen, FRG). This protocol was performed using different flow rates and pharmacological interventions. After a first stabilization period (15-20 minutes), each experiment started with a test response to the endothelium-dependent dilator ACh, followed by a further 30-minute stabilization period. The platelet cGMP content was evaluated with pairs of perfusate samples: a platelet-free sample taken 30 seconds before platelet injection and a sample containing the collected platelets. Platelets (300-gl bolus) were injected at time 0, over a 2-second period, and collected between 4 and 8 seconds, 3 and 5 seconds, and 2 and 3.5 seconds for perfusion rates of 20, 40, and 60 ml/min, respectively. An infusion of 0.1 ,uM superoxide dismutase (SOD, Serva, Heidelberg, FRG) was started 2 minutes before each bolus injection and maintained until platelets had been collected. In all experiments, the initial perfusion rate was set at 20 ml/min and, unless otherwise stated, maintained constant. In a first experimental series (n =7), bolus injections of platelets were administered before and after inhibition of endothelial NO synthesis (30-minute infusion of 30 ,uM N0-nitro-L-arginine [L-NNA], Serva). To assess whether platelet-derived NO12 contributes to cGMP increases, platelets were incubated for 30 minutes with 100 ,uM L-NNA in additional experiments (n=3). In a second experimental series (n=6), the effect of flow rate on NO release was studied. NO release was determined at perfusion rates of 20, 40, and 60 ml/min under unstimulated conditions and during ACh stimulation at 3 and 13 minutes after the flow increase, respectively. In a third experimental series (n = 8), we studied the effect of increasing shear stress on NO release at a constant flow rate by means of a vasoconstriction induced by a 1-nM infusion of Lamontagne et al Mechanisms of Basal EDRF Release Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 endothelin-1 (Peninsula Laboratories, Inc., Belmont, Calif.). In a final experimental series (n = 13), luminal NO release was determined before and 10 minutes after the cardiac arrest induced by a 0.02% mepivacaine (Astra Chemical, Wedel, FRG) infusion and again after washout of this drug. Platelet cGMP Content The coronary effluent collected was pipetted into tubes containing 100% trichloroacetic acid (final concentration of 6%). After centrifugation, trichloroacetic acid was extracted from the supernatant with water-saturated diethyl ether (four times, 5 vol ether for 1 vol sample), and the samples were kept at -20°C until analysis. cGMP was determined using a commercially available radioimmunoassay (New England Nuclear, Dreieich, FRG). The platelet cGMP content was calculated from the difference between the platelet-containing and platelet-free samples and was expressed as picomoles of cGMP per milligram of platelet protein. Protein Content The pellet of the centrifuged coronary effluent samples was redissolved in 100 gl of 1N NaOH, and the protein content of the sample was determined according to Lowry et al.13 Infusion of Drugs ACh, L-NNA, and SOD were dissolved in physiological perfusion buffer and infused at ¼loo of the coronary flow rate to produce a final concentration of 1, 30, and 0.1 ,M, respectively. Endothelin-1 was dissolved in a 0.2% bovine serum albumin solution and diluted with physiological perfusion buffer for a final concentration of 1 nM. Mepivacaine (Scandicain 1% solution, Astra Chemical) was infused at 2/oo of the coronary flow rate to produce a final concentration of 0.02%. NO Release From Isolated Perfused Arterial Segments Segments of rabbit femoral arteries (1.5 cm in length) with an intact endothelium were freed from adventitial tissue, cannulated at both ends, and placed in an organ bath. Luminal perfusion (10.4 ml/hr) was performed separately from organ bath perfusion with normal Tyrode's solution. The shear stress on the endothelium was increased by reducing the vessel diameter with either 30 ,uM norepinephrine (Arterenol, Hoechst AG, Frankfurt, FRG) or 60 nM endothelin-1, while maintaining the same perfusion rate. The effect of mepivacaine was tested under these experimental conditions to assess its effect on shear stress-induced release of EDRF. The effect of mechanically induced vessel wall deformation on EDRF release was also studied in the isolated perfused arterial segments. Two opposing plates, covered with a soft material, were used to perform a rhythmic squeezing (90 per minute) of the segments, with the lumen practically closed during the compression phase. - 2.U l1 1 = 125 control m ACh L._ 0 0. c, * 1.5- E E 1.0_. 0c 0.5- 0 4) -6J 0.0 - without L-NNA L-NNA L-NNA (endothelium) (platelets) FIGURE 1. Bar graph showing platelet cGMP content after passage through the coronary bed under control conditions and during acetylcholine (ACh, 1 pM) infusion, both in the absence of NG-nitro-L-arginine (L-NNA) (n= 7), after a 30minute intracoronary infusion of 30 MM L-NNA (n= 7), or after a 30-minute preincubation of platelets with 100 ,uM L-NNA (n=3). *p<0.05. The EDRF released from these segments was evaluated by activation of purified guanylate cyclase (GC) from bovine lungs.14 Effluent from the perfused vessels was collected for 15 seconds into a reaction mixture containing triethylamine-HCl buffer (30 mM, pH 7.4), MgCl2 (3 mM), SOD (0.3 ,uM), 0.1 mM [a-32P]GTP (0.2 ,uCi), glutathione (3 mM), EGTA (0.1 mM), bovine gamma globulin (0.1 mg/ml), and soluble GC (200 nM) purified to apparent homogeneity. The reaction proceeded for 1 minute at 37°C and was terminated by the addition of 50 mM zinc acetate and 55 mM sodium carbonate. Labeled cGMP was then separated from other nucleotides on small alumina columns, and GC activity was calculated. A detailed description of this technique is given elsewhere.15 Statistics Heart rate and CPP were analyzed with parametric statistical tests. A paired Student's t test was used for comparison of two observations; an analysis of variance for repeated measurements was used for three or more observations. Since platelet cGMP data were not normally distributed, nonparametric tests were used. A Wilcoxon matched-pair signed-rank test was used to compare two paired observations; a Friedman test followed by a Wilcoxon and Wilcox multiple comparison was used for more than two observations. All results are presented as mean+SEM. Results Effect of L-NNA on Platelet cGMP The cGMP content of platelets before passage through the heart amounted to 0.18+±0.04 pmol/mg protein (n =9). When platelets were injected into the coronary bed, the cGMP content increased by 2.8fold under control conditions and by 7.5-fold during ACh stimulation (Figure 1). After a 30-minute infu- 126 Circulation Research Vol 70, No 1 January 1992 9: from 40 to 60 mI/min A: from 20 to 40 ml/min 150 G) Q) 60- c - 0 a)(L) Q} 100 E E alCL 0 40 - ron T *- CL - T 0 50- 00 1 0 1 5 . . 0 . . . . . 20 . Q) (0 5 Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 time [min] FIGURE 2. Coronary perfusion pressure (CPP) plotted as a function of time after increases in perfusion rate from 20 to 40 mllmin (panel A) and from 40 to 60 ml/min (panel B). Horizontal error bars represent ±SEM of the time after which the minimal pressure value was observed. *p<0.05 (n=6) compared with the preceding value. 0 60 40 20 flow rate [mi/min] FIGURE 3. Bar graph showing platelet cGMP content, expressed as percent of the platelet cGMP content measured during 1 iM acetylcholine (ACh) infusion, under different perfusion rates. *p<O0.05 (n=6). sion with L-NNA, the cGMP content of platelets passing through the unstimulated heart (0.18±0.08 pmol/mg protein) was similar to the amount found in platelets before passage, indicating that a basal, agonist-independent EDRF release was responsible for the increase in platelet cGMP content under control conditions. Likewise, the ACh-induced increase in platelet cGMP was totally blocked by L-NNA (Figure 1). In contrast, platelets treated with 100 ,uM L-NNA showed a similar increase in cGMP after passage through the heart under control conditions as well as during ACh stimulation (Figure 1), which excludes any important contribution of platelet-derived NO in the cGMP content increases we observed in our experimental conditions. Effect of Increases in Flow Rate Increases in flow rate from 20 to 40 ml/min and from 40 to 60 ml/min were accompanied by proportional increases in CPP and led to flow-dependent dilation, as reflected by the significant drop in CPP that followed the initial rise (Figure 2). To detect the effect of increasing flow on luminal NO release, one has to consider that the platelet transit time is inversely related to the flow rate. Consequently, the platelet cGMP content under ACh stimulation decreased linearly with increasing flow rate (2.52±0.61, 1.31+0.66, and 0.78±0.37 pmol/mg protein for 20, 40, and 60 ml/min, respectively). Expressed in percent of the values obtained during ACh stimulation, the platelet cGMP content under unstimulated conditions showed a significant increase with increases in flow rate (Figure 3). The effect of NO synthesis inhibition with L-NNA (30 ,M) on the flow-dependent dilation was studied in a separate series of experiments. A 30-minute infusion of L-NNA reversed the ACh-induced vasodilation to a constriction and prevented the flowdependent dilation (Figure 4). The dilator response gM sodium nitroprusside infusion was not affected by L-NNA. None of these effects were observed with the inactive D stereoisomer of L-NNA. Effect of an Increased Shear Stress Induced by Vasoconstriction The strong vasoconstriction produced by endothelin-1 in the coronary vascular bed was used to increase shear stress while maintaining constant flow rate. Infusion of 1 nM endothelin-1 increased the CPP from 37±3 to 101±7 mm Hg (p <0.001). Under these conditions, the cGMP content of platelets passing through the vascular bed was increased 2.5fold (Figure 5). Despite the strong vasoconstriction, the dilator response to ACh (20±6% before versus 24±4% during infusion of endothelin-1) as well as the ACh-induced increase in platelet cGMP (Figure to 1 ACh 130- - flow increase (2 fold) CPP [mm3Hg] 30J .-NHA W 1 min FIGURE 4. Original recordings of coronary perfusion pressure (CPP) during an infusion of 1 1iM acetylcholine (ACh) and after a twofold increase in perfusion rate (from 25 to 50 ml/min), both before and after a 30-minute infusion with 30 /gLM NG-nitro-L-a,ginine (L-NNA). Similar results were obtained in five additional experiments. Lamontagne et al Mechanisms of Basal EDRF Release A: unstimulated heart 1.5* 1.0o 2 C .0 0 0 0. -U, 0 cr E N 1.0 CL 0~> E r- ---7 r* **-I 3 0.5 1 :~[ a. 0.5 r>2 E 0 EE E N ns E cL E B: ACh-stimulation A: unstimulated heart B: ACh-stimulation 127 1 0. C, 0.0 U0 CL0.0- 0Q control endothelin control endothelin Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 FIGURE 5. Bar graphs showing platelet cGMP content after passage through the coronaty bed of the unstimulated heart (panel A) and the increase in platelet cGMP content after the induction of acetylcholine (ACh, 1 pM) (panel B), both before (control) and during the strong vasoconstriction induced by infusion of endothelin-1 (1 nM). *p<0.05 (n=8). 5) were not affected. In this group, a significant positive correlation between platelet cGMP content and CPP was observed (Figure 6, top panel), indicating that NO release is proportional to shear stress. Effect of Cardiac Arrest Induced by Mepivacaine Heart rate and developed left ventricular pressure under control conditions were 157±8 beats per 2.4 r=0.63, p<0.05 * control o endothelin i - ,' .I 1.6 - 00 ._ 0-m 0.8 cL- 0.0 j 5- 80 40 CPP Q- 120 [mmHg] 0 0~ CD 0.6 r=0.09, ns 0 0a .:4 .0 0.4~ 0* 0 CL 0.2 * * 0 L *B 0.0 l00 150 200 heart rate [beats/min] FIGURE 6. Scatter plots showingplatelet cGMP content as a function of coronary perfusion pressure (CPP) (top panel) and of heart rate (bottom panel). Linear regressions (solid line) are shown along with the 95% confidence interval (dashed lines) in the top panel. washout control mepivocoine washout mepivocoine control FIGURE 7. Bar graphs showing platelet cGMP content after passage through the coronary bed of the unstimulated heart (panel A) and the increase in platelet cGMP content after the induction of acetylcholine (ACh, 1 MM) (panel B), both before (control) and during cardiac arrest induced by a 0. 02% mepivacaine infusion and after washout of this drug. *p<0.05 and **p<0.01 (n=13). minute and 88 ± 6 mm Hg, respectively. Perfusion of mepivacaine resulted in a rapid cardiac arrest, with undetectable levels of developed left ventricular pressure within seconds. The CPP response to mepivacaine was biphasic, with a rapid pressure drop (from 40±4 to 28±3 mm Hg, p<0.01) preceding a slow increase in perfusion pressure (maximal value of 80+3 mm Hg,p<0.01). The cGMP content of platelets passing through the arrested heart was significantly reduced by more than 50%, compared with that under control conditions (Figure 7). In contrast, the platelet cGMP content (Figure 7) and the reduction in CPP (21±6% versus 20±3%) during ACh infusion were not affected by mepivacaine. Washout of mepivacaine resulted in a rapid recovery of the mechanical activity in all hearts studied: heart rate was restored to 132±7 beats per minute (p<0.01 compared with control), and developed left ventricular pressure was restored to 80±4 mm Hg (p>0.05). The platelet cGMP content after passage through the heart was no longer reduced (Figure 7). The ACh-induced reduction in CPP (26±4%) and the increase in platelet cGMP (Figure 7) were slightly increased after washout of mepivacaine, although the difference was not statistically significant. Mepivacaine modified the cGMP content neither of resting platelets nor of platelets stimulated in vitro with sodium nitroprusside (1 and 10 ,uM) (data not shown). In a separate experimental series, the effect of an enhanced heart mechanical activity on platelet cGMP content was studied with a continuous norepinephrine infusion (1 ,uM). Increases in both heart rate and contractility by more than 50% did not significantly affect platelet cGMP content after passage through the coronary system (from 0.29+16 to 0.32±0.19 pmol/mg protein, n=6). Similarly, we found no significant correlation between platelet cGMP content and heart rate of unstimulated, spontaneously beating hearts under control conditions (Figure 6, bottom panel). 128 Circulation Research Vol 70, No 1 January 1992 Release of EDRF (NO) From Isolated Femoral Segments At a resting diameter of 1,920±100 ,um, the activity of purified GC added to the effluent from the segments was 5.3+1.4 nmol* min-l mg-1 protein (n=6). Both endothelin-1 and norepinephrine induced a strong constriction (1,170±70 ,um) at constant perfusion rate that was associated with an increase in GC activity to 9.3±2.0 nmol * min-1 mg` (p<0.01, n=7). The increased EDRF release was no longer observed when the vasoconstriction was abolished by forskolin (3 gM) (data not shown). The addition of 0.02% mepivacaine in the luminal perfusion had no influence on the diameter of maximally constricted femoral segments and did not affect the shear stress-induced release of EDRF (GC activity, 10.8±2.4 nmol min-l *mg-1). The rhythmic compression and decompression (1.5 Hz) of femoral segments also induced an increase in GC activity from 7.3±0.4 to 17.4±1.0 nmol* min-l mg-1 (p<0.05, n=3). The dilator response to ACh (1 ,uM) was not affected by this rhythmic compression and decompression (data not shown), indicating the preservation of the functional integrity of the endothelium. - Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 Discussion In the present study, we used human platelets as a bioassay tissue for the detection of EDRF (NO) released from the luminal side of the coronary vascular bed. Human platelets contain considerable amounts of soluble GC,16 which can be activated by NO during a single passage through the coronary bed. This approach has already been proven to be a reliable index of EDRF (NO) release.6,8 It has been reported recently that human platelets stimulated with collagen can synthesize NO.12 However, it is unlikely that platelet-derived NO contributes in a major part to the cGMP increase we observed, since the preincubation of platelets with a high concentration of L-NNA did not alter the increases in cGMP. Increments in flow induced a vasodilation in the coronary bed, as reflected by the pressure drop that follows the sharp initial rise in CPP. Flow-dependent dilation has been well documented in epicardial coronary arteries of laboratory animals'7,18 and humans,1920 as well as in other conduit arteries.2122 Furthermore, it was found to be endothelium dependent.1921,22 Our data indicate that flow-dependent dilation takes place not only in large conduit arteries but also in resistance-sized vessels. Increments in flow were also accompanied by increases in EDRF release. An enhanced nitrite outflow from the unstimulated rabbit heart induced by an increase in flow rate has recently been described.23 Our study adds further evidence of a flow-induced EDRF release from the unstimulated heart. These findings, added to the fact that L-NNA abolishes the flowdependent dilation, are strongly in favor of EDRF as the endothelial mediator of flow-dependent dilation in the coronary bed. Flow exerts its effect through the shear stress imposed on the endothelial lining. This is illustrated best by the experiments with endothelin-1 at constant flow rate. Endothelin-1 elicited a strong and sustained vasoconstriction that increased both shear stress on endothelial cells and release of EDRF. Increasing shear stress in isolated arterial segments resulted also in an enhanced release of EDRF. There are reports indicating that endothelin-1 may stimulate directly the release of EDRF from arterial segments of rats24 and rabbits.25 In rabbit femoral arteries, however, no EDRF release by endothelin-1 was observed when the constriction was abolished by a strong vasodilator. This is in agreement with our previous report in which endothelin-1 did not elicit EDRF release from rabbit aortic segments.26 In the rabbit heart, bolus injections of endothelin do not induce vasoconstriction unless hemoglobin is present or the endothelium is destroyed.27 This can be interpreted as a direct stimulatory effect of endothelin on endothelial EDRF release. On the other hand, one cannot rule out the possibility that the shear stress-induced EDRF release readjusts vessel tone, maintaining a constant CPP despite the transient exposure of the coronary vessels to the peptide. Likewise, endothelin has been reported to stimulate the release of prostacyclin from the isolated rabbit heart.28 Since flow increases are also accompanied by an enhanced release of prostacyclin,23 it is possible that the endothelin-induced release of prostacyclin is in fact the consequence of an increased shear stress. Thus, discrimination between direct and shear stress-induced effects of endothelin is difficult. In our study, however, the positive correlation between platelet cGMP and CPP is highly suggestive of a shear stress-induced release of EDRF. The platelet cGMP content after passage through the coronary bed of the unstimulated heart is significantly reduced after endothelial NO synthesis inhibition with L-NNA. This strongly suggests that, under basal conditions, the endothelium continuously releases EDRF in a concentration high enough to activate the platelet GC during a single passage through the coronary system. Other studies have confirmed the existence of a basal, agonist-independent release of EDRF.4-6 The residual platelet cGMP content after L-NNA, which is very close to the cGMP content of resting platelets (before passage through the heart) might reflect their basal GC activity. Cardiac arrest induced by mepivacaine led to a significant reduction in the cGMP content of platelets after passage through the unstimulated heart, which was reversed after reappearance of heart mechanical activity. The normal cardiac activity is accompanied by the cyclic compression and decompression of blood vessels, including endothelial cells. This mechanical activity, which also imposes a highly oscillatory flow in the coronary bed, is no longer Lamontagne et al Mechanisms of Basal EDRF Release Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 present during cardiac arrest. Therefore, it is very likely that the beating heart, by imposing a compression-decompression cycle on the endothelial lining and by creating an oscillatory shear stress, stimulates a continuous release of EDRF. The stimulatory effect of rhythmic endothelial compression and decompression on EDRF release was confirmed in isolated arterial segments. The similar reduction in platelet cGMP content with both cardiac arrest and endothelial NO synthesis inhibition by L-NNA suggests that the mechanical activity is the basal stimulus for a continuous release of EDRF in the coronary system. Since increases in heart rate and contractility do not result in a further increase in platelet cGMP content, it is likely that this mechanically induced NO release is already completely activated in the spontaneously beating heart. The lack of a positive correlation between heart rate and NO release is also in favor of an all-or-none stimulatory effect of the heart mechanical activity. Moreover, the endothelial lining of the vascular system is constantly exposed in vivo to shear stress exerted by the streaming blood. We found that flow stimulates in a proportional manner NO formation in the coronary system, superimposed on the mechanically induced NO release. This flowinduced NO release may then contribute to the adjustment of the conductivity of conduit and resistance-sized arteries in the heart, by counteracting neuronal or myogenic vasoconstriction. It is interesting to note that cardiac arrest was accompanied by a vasoconstriction, most likely due to the absence of mechanical work and the subsequent reduced production of vasoactive metabolites (such as adenosine and protons). Despite the resulting increase in shear stress, a reduction in platelet cGMP content after passage through the unstimulated arrested heart was observed, which suggests that, in the saline-perfused coronary microcirculation, the stimulation of the endothelium by shear stress is subthreshold with the absence of the heart mechanical activity. It has been reported that endothelium-dependent dilations are reduced by some local anesthetics, suggesting an inhibition of EDRF release by these drugs.29 However, we found that mepivacaine has no inhibitory action on ACh-induced release of EDRF or on the dilator response to this agonist. We were also unable to detect an effect of mepivacaine, at the concentration used in this study, on shear stressinduced release of EDRF in isolated arterial segments. Furthermore, mepivacaine has no effect on soluble GC of platelets or on the activation of this enzyme by NO, since neither the basal values nor sodium nitroprusside-induced increases in cGMP were modified in the presence of this drug. In conclusion, flow, by inducing shear stress on the endothelial lining, stimulates the release of EDRF, which accounts for the flow-dependent dilation observed in the coronary bed. However, the basal stimulus for the continuous EDRF formation in the intact coronary microcirculation may be the mechanical activity of the heart, by imposing an oscillatory 129 shear stress and a direct deformation of blood vessel wall. In addition to this continuous EDRF formation, shear stress-induced EDRF release can adjust vascular conductivity of the coronary bed. Acknowledgments The skillful technical assistance of H. Miinzel, I. Winter, and C. Kircher is gratefully acknowledged. References 1. Furchgott RF: Studies on the relaxation of rabbit aorta by sodium nitrite: The basis for the proposal that the acidactivatable inhibitory factor from bovine retractor penis is inorganic nitrite and the endothelium-derived relaxing factor is nitric oxide, in Vanhoutte PM (ed): Vasodilatation. New York, Raven Press, Publishers, 1988, vol 4, pp 401-414 2. Palmer RMJ, Ferrige AG, Moncada S: Nitric oxide release accounts for the biological activity of endothelium-derived relaxing factor. Nature 1987;327:524-526 3. Furchgott RF: The role of endothelium in responses of vascular smooth muscle. Circ Res 1983;53:557-573 4. Kelm M, Schrader J: Nitric oxide release from the isolated guinea pig heart. Eur J Pharmacol 1988;155:313-316 5. Kelm M, Schrader J: Control of coronary vascular tone by nitric oxide. Circ Res 1990;66:1561-1575 6. Pohl U, Busse R: EDRF increases cyclic GMP in platelets during passage through the coronary vascular bed. Circ Res 1989;65:1798-1803 7. Amezcua JL, Palmer RMJ, de Souza BM, Moncada S: Nitric oxide synthesized from L-arginine regulates vascular tone in the coronary circulation of the rabbit. Br J Pharmacol 1989;97: 1119-1124 8. Lamontagne D, Pohl U, Busse R: N0-Nitro-L-arginine antagonizes endothelium-dependent dilator responses by inhibiting endothelium-derived relaxing factor release in the isolated rabbit heart. Pflugers Arch 1991;418:266-270 9. Rubanyi GM, Romero JC, Vanhoutte PM: Flow-induced release of endothelium-derived relaxing factor. Am J Physiol 1986;250:H1145-H1149 10. Cooke JP, Stamler J, Andon N, Davies PF, McKinley G, Loscalzo J: Flow stimulates endothelial cells to release a nitrovasodilator that is potentiated by reduced thiol. Am J Physiol 1990;259:H804-H812 11. Pohl U, Busse R, Kuon E, Bassenge E: Pulsatile perfusion stimulates the release of endothelial autacoids. JAppl Cardiol 1986;1:215-235 12. Radomski MW, Palmer RMJ, Moncada S: An L-arginine nitric oxide pathway present in human platelets regulates aggregation. Proc Natl Acad Sci U SA 1990;13:5193-5197 13. Lowry OH, Rosebrough NJ, Farr AL, Randall RJ: Protein measurement with phenol reagent. J Biol Chem 1951;193: 265-275 14. Mulsch A, Gerzer R: Purification of heme-containing soluble guanylyl cyclase, in Johnson RA, Corbin JD (eds): Methods in Enzymology. New York, Academic Press, Inc, 1991, vol 195, pp 377-383 15. Jackson WF, Mulsch A, Busse R: Rhythmic smooth muscle activity in hamster aortas is mediated by continuous release of NO from the endothelium. Am JPhysiol 1991;260:H248-H253 16. Bohme E, Jung R, Mechler I: Guanylate cyclase in human platelets, in Hardman JG, O'Malley BW (eds): Methods in Enzymology. New York, Academic Press, Inc, 1974, vol 38, pp 199-202 17. Gerova M, Smiesko V, Gero J, Barta E: Dilatation of conduit coronary artery induced by high blood flow. Physiol Bohemoslov 1983;32:55-63 18. Hintze TH, Vatner SF: Reactive dilation of large coronary arteries in conscious dogs. Circ Res 1984;54:50-57 19. Nabel EG, Selwyn AP, Ganz P: Large coronary arteries in humans are responsive to changing blood flow: An endothelium-dependent mechanism that fails in patients with atherosclerosis. JAm Coil Cardiol 1990;16:349-356 130 Circulation Research Vol 70, No 1 January 1992 20. Zeiher AM, Drexler H, Wollschlager H, Just H: Modulation of coronary vasomotor tone in humans: Progressive endothelial dysfunction with different early stages of coronary atherosclerosis. Circulation 1991;83:391-401 21. Pohl U, Holtz J, Busse R, Bassenge E: Crucial role of endothelium in the vasodilator response to increased flow in vivo. Hypertension 1986;8:37-44 22. Hull SS, Kaiser L, Jaffe MD, Sparks HV: Endotheliumdependent flow-induced dilation of canine femoral and saphenous arteries. Blood Vessels 1986;23:183-198 23. Wennmalm A, Benthin G, Karwatowska-Prokopczuk E, Lundberg J, Petersson A-S: Release of endothelial mediators and sympathetic transmitters at different coronary flow rates in rabbit hearts. J Physiol (Lond) 1991;435:163-173 24. de Nucci G, Thomas R, D'Orleans-Juste P, Antunes E, Walder C, Warner TD, Vane JR: Pressor effects of circulating endothelin are limited by its removal in the pulmonary circulation and by the release of prostacyclin and endotheliumderived relaxing factor. Proc Natl Acad Sci U S A 1988;85: 9797-9800 25. Warner TD, Mitchell JA, de Nucci G, Vane JR: Endothelin-1 and endothelin-3 release EDRF from isolated perfused arterial vessels of the rat and rabbit. J Cardiovasc Pharmacol 1989;13(suppl 5):S85-S88 26. Pohl U, Busse R: Differential vascular sensitivity to luminally and adventitially applied endothelin-l. J Cardiovasc Pharmacol 1989;13(suppl 5):S188-S190 27. Stewart DJ, Baffour R: Functional state of the endothelium determines the response to endothelin in the coronary circulation. Cardiovasc Res 1990;24:7-12 28. Karwatowska-Prokopczuk E, Wennmalm A: Effects of endothelin on coronary flow, mechanical performance, oxygen uptake, and formation of purines and on outflow of prostacyclin in the isolated rabbit heart. Circ Res 1990;66:46-54 29. Johns RA: Local anesthetics inhibit endothelium-dependent vasodilation. Anesthesiology 1989;70:805-811 KEY WORDS * endothelium-derived relaxing factor * endothelium * flow-dependent dilation * L-arginine analogues * cGMP platelets Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 Mechanical deformation of vessel wall and shear stress determine the basal release of endothelium-derived relaxing factor in the intact rabbit coronary vascular bed. D Lamontagne, U Pohl and R Busse Downloaded from http://circres.ahajournals.org/ by guest on May 4, 2017 Circ Res. 1992;70:123-130 doi: 10.1161/01.RES.70.1.123 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1992 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/70/1/123 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/