Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
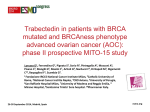
Randomized phase III trial on Trabectedin (ET 743) vs clinician’s choice chemotherapy in recurrent ovarian, primary peritoneal or fallopian tube cancers of BRCA mutated or BRCAness phenotype patients MITO – 23 Randomized phase III STRATIFICATION CRITERIA: Measurable Disease Platinum Sensitivity Number of Previous CHT Lines Mutational status Recurrent ovarian, primary peritoneal or fallopian tube cancers of BRCA mutated or BRCAness phenotype patients II line chemotherapy (physician choice): - PLD 40 mg/mq d1 q28; - Topotecan 4 mg/mq d1,8,15 q 28 - Weekly Paclitaxel 80 mg/mq d1,8,15 q28 - Gemcitabine 1000 mg/mq gg1,8,15 q28 - Carboplatin AUC 5 g 1 q 21 Random 1.1 Trabectedin 1.3 mg/mq d1 q 21 in 3 hours (central line) MITO - 23 STUDY OBJECTIVES Primary: The primary objective is to compare the treatment groups in terms of overall survival (OS) Secondary: •Progression free survival (PFS) •Radiological response rate (in patients with measurable disease) •Duration of response •CA-125 response rate per GCIG •Toxicity profile •Quality of life using the QLQ-C30 and QLQ-0V28 MITO - 23 INCLUSION CRITERIA • Female of age 18 years or older • Histologically or cytologically documented invasive epithelial ovarian cancer, primary peritoneal carcinoma, or fallopian tube cancer • Platinum resistant or sensitive patients with either: BRCA mutated patients BRCAness phenotype patients: patients who have received and responded (subsequent PFI>6 months) to at least 2 previous platinum based chemotherapy lines Platinum sensitive patients who are not able to receive or not willing to receive other platinum treatments • Measurable and evaluable disease per RECIST 1.1(Subjects with isolated rising CA-125 without radiologically visible disease are excluded) • ECOG performance status 0 or 1 • No limits in the number of previous chemotherapy lines, previous treatment with parp inhibitors is allowed • Left Ventricular Ejection Fraction (LVEF) ≥ institutional lower limit normal • Life expectancy of at least 3 months • Adequate organ functions • No other invasive malignancy within the past 3 years except non-melanoma skin cancer or in situ cervical cancer (patients with previous cancers may be enrolled providing that no recurrences have be reported in the last 3 years) • Written Informed Consent • Adequately recovered from the acute toxicity of any prior treatment • For agents in the standard arm, also refer to the local prescribing information with regards to warnings, precautions, and contraindications MITO - 23 EXCLUSION CRITERIA • Prior exposure to trabectedin • Known hypersensitivity to any of the components of the trabectedin i.v. formulation or dexamethasone • Subjects with borderline ovarian cancer, ie. Subject with low malignant potential tumors are excluded • Less than 2 reported responses to platinum (i.e. subsequent recurrences at least 6 months after the first and the second platinum based treatment), unless BRCA mutation is documented. • Less than 4 weeks from last dose of therapy with any investigational agent, or chemotherapy • History of another neoplastic disease (except basal cell carcinoma or cervical carcinoma in situ adequately treated) unless in remission for 3 years or longer • Known clinically relevant CNS metastases, unless treated and asymptomatic • Other serious illnesses, such as: Congestive heart failure or angina pectoris; myocardial infarction within 1 year before enrolment; uncontrolled arterial hypertension or arrhythmias. Psychiatric disorder that prevents compliance with protocol Active viral hepatitis; or chronic liver disease. Active infection. Any other unstable medical conditions. MITO - 23 Assessment Written Informed Consent Screening Day Before study procedures Cycle Day 1 Day 8 End of Treatment Day 15 Day 16-21 Demographic Data - 28 to 0 Medical History - 28 to 0 Prior surgical and/or chemotherapy treatments - 14 to 0 Vital Signs (heart rate, blood pressure, temperature) - 14 to 0 X Complete Physical Examination (assessment of signs and symptoms of desease) - 14 to 0 X X X X Performance Status (ECOG) - 14 to 0 X X X X ECG - 28 to 0 Repeat if clinically indicated Echocardiogram -28 to 0 Repeat every 3 cycle only in case of PLD and T treatments, in all other cases repeat only if clinically indicated Concomitant Disease and Medication - 14 to 0 Throughout the study Adverse Events - 14 to 0 Throughout the study Hematology Coagulation Test -7 to 0 -7 to 0 X Xa Xa X X Chemistry and Liver Panel -7 to 0 X Xa Xa X QoL assessments X Radiologic evaluations - 28 to 0 CA 125 -7 to 0 X Every 3 chemotherapy cycles Every 12 +/- 1 week X Follow Up X X X X Xb STATISTICS PROTOCOL Phase III The primary endpoint is OS Hazard Ratio: 0.67 Median OS expected in the control arm: 10 months Median OS hoped for the experimental arm : 15 months Two-sided log-rank test at the error alfa= 0.05 Statistical Power 80% 198 events are required Overall 244 patients will be enrolled in 30 months (8 patients/months) Interim futility analysis at ~ 99 events MITO - 23 MITO-23: TRANSLATIONAL STUDIES • Evaluating the impact of altered gene and microRNA (miRNA) expression on trabectedin efficacy with the aim of identify which genes are involved in the so called BRCAness phenotype; • Analysis of cellular infiltrate present on tumor specimens of patients treated with trabectedin; • DNA sequencing in order to evaluate mutation/genetic aberration profile in selected panels of genes associated to tumor sensibility to trabectedin (BRCA test). MITO - 23 TRANSLATIONAL STUDIES: Specimens Tumor histological blocks (FFPE material): samples will be collected at primary surgery and/or interval debulking surgery (or before trabectedin treatment by dedicated biopsies). Storage and analysis will be centralized at Fondazione Istituto Nazionale dei Tumori. •Characterization of tumor infiltrate by IHC (2 slides per marker & 1 HE slide & 3 backup slides); •Extraction of RNA from tissue sections for gene expression by DASL microarray analysis; •Extraction of DNA from tissue sections for targeted sequencing of “Panel cancer related genes” (in collaboration with Istituto Mario Negri, Milan). Blood samples: Blood samples will be collected at baseline (registration), at third cycle of treatment and at progression. Storage and analyses will be centralized at Fondazione IRCCS Istituto Nazionale Tumori, Milan. 10 ml blood sample will be taken at each time point, centrifuged in EDTA, processed to obtain 5 ml plasma collected and stored at -20°C or at 80°C when possible. •Analysis of miRNA profile by Agilen microarrays or evaluation of selected miRNA by RT-qPCR (in collaboration with Fondazione Istituto Nazionale dei Tumori) MITO - 23 Site Principal Investigator Status Ethical Committee Francesco Raspagliesi/ Domenica Lorusso In approvazione 26.11.2015 Fondazione Policlinico Universitario A. Gemelli - Roma Giovanni Scambia In valutazione 03.12.2015 Istituto Nazionale Tumori Pascale - Napoli Carmen Pisano In valutazione 16.12.2015 Ospedale San Raffaele – Milano Giorgia Mangili In istruttoria Fondazione del Piemonte per l'Oncologia - Istituto di Candiolo Giorgio Valabrega In istruttoria Ospedale Fatebenefratelli - Roma Enrico Breda In compilazione ULLS 13 - Mirano Grazia Artioli In istruttoria IRST - Meldola Ugo De Giorgi In istruttoria A.O. di Perugia - Ospedale Santa Maria Misericordia - Perugia Anna Maria Mosconi In valutazione Sapienza Università di Roma-Policlinico Umberto I - Roma Pierluigi Benedetti Panici In istruttoria CRO IRCCS - Aviano Roberto Sorio In istruttoria IRE-Istituto Nazionale Tumori REGINA ELENA - Roma Patrizia Vici In istruttoria AOU Federico II Sabino De Placido In compilazione Fondazione IRCCS Policlinico S.Matteo di Pavia Stefano Bogliolo In istruttoria U.O.Oncologia Medica - Ospedale Vito Fazzi - Lecce Graziana Ronzino In istruttoria Ospedale degli Infermi - Faenza Stefano Tamberi In istruttoria AULSS 21 Regione Veneto - Legnago Filippo Greco In valutazione Ospedale Civile SS. Trinità - Sora Teresa Gamucci In istruttoria A.O. S.Giuseppe Moscati - Avellino Cesare Gridelli In istruttoria Ospedale Santa Croce - Fano Rodolfo Mattioli In istruttoria A.O. Carlo Poma - Mantova Maria Giovanna Cavazzini In istruttoria Ospedale S.Maria delle Croci - Ravenna Claudia Casanova In istruttoria A.O.U. Santa Maria della Misericordia - Udine Claudia Andreetta In istruttoria Centro Sociale Oncologico AAS1 Triestina - Trieste Rita Ceccherini In istruttoria IRCCS AOU San Martino - IST - Genova Serafina Mammoliti In istruttoria Ospedale Civile G.Fornaroli - Magenta Silvia Elvira Negretti In istruttoria Istituto Europeo di Oncologia - Milano Nicoletta Colombo In istruttoria Arcispedale sant'anna - Cona, Ferrara Antonio Frassoldati In istruttoria Spedali Civili di Brescia - Brescia Germana Tognon In istruttoria AOU Maggiore della Carità - Novara Roberta Buosi IRCCS Istituto Nazionale Tumori – Milano COORDINATING CENTER MITO - 23 In istruttoria 16.12.2015 02.12.2015 ADMINISTRATIVE INFORMATION •Academic trial •NCI of Milan sponsor •Data center: NCI of Milan (MITO center) •Planned study start: February 2016 •Pharma-Mar support: Trabectedin supply , financial support for insurance, translational studies and data management. MITO - 23