Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Urinary tract infection wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Behçet's disease wikipedia , lookup
Common cold wikipedia , lookup
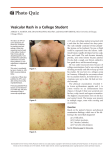
Infection control wikipedia , lookup
Neonatal infection wikipedia , lookup
Hepatitis C wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Schistosomiasis wikipedia , lookup
Pathophysiology of multiple sclerosis wikipedia , lookup
Hepatitis B wikipedia , lookup
Onchocerciasis wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Dermatology and HIV HAIVN Harvard Medical School AIDS Initiative in Vietnam 1 Learning Objectives By the end of this session, participants should be able to: Describe the most common skin diseases among PLHIV in Vietnam Explain how to treat these skin conditions 2 What are Common Skin Conditions Among PLHIV in Vietnam? Pruritis Drug allergy rash Varicella-Zoster Herpes Simplex Seborrheic dermatitis Scabies Molluscum contagiosum Penicillium Marneffei PPE (PapuloPruritic Eruption) 3 Pruritis - Itchy Skin (1) Causes: Dry scaly skin: • Seborrheic dermatitis • Fungal infection • Eczema • Xerosis Papules: • Scabies • Insect bites • Eosinophilic folliculitis • Papulopruritic eruption • Infections 4 Pruritis - Itchy Skin (2) Treatment: Oral antihistamines Topical moisturizers Topical steroids Avoid excessive bathing, soap, or hot water 5 Topical Steroid Use for Pruritis Use the lowest potency that is effective for the least amount of time needed Topical Steroids by Potency: Potency Steroid Low Medium High • Hydrocortisone (Hytone, Synacort) • Fluocinolone (Flucinar, Synalar) • Triamcinolone (Kenalog) • Clobetasol (Cloderm, Dermovate, Eumovate, Powercort) • Betamethasone (Diprolene, Diprosalic, Beprosalic) 6 What is the Diagnosis? This patient presented with a painful rash on the back of the neck for 2-3 days On exam, there were multiple vesicles with surrounding erythema 7 Varicella Zoster Virus (VZV) Shingles – Zona (1) Vesicular rash in one dermatome Treatment: • Acyclovir 800 mg 5x/d x 7d • Most effective if started within 72 hours of onset of rash For >1 dermatome or disseminated infection: • Acyclovir IV 10 mg/kg q8hr x 7-14 days 8 Varicella Zoster Virus (VZV) Shingles – “Zona” (2) 9 What is the Diagnosis? This patient presented with a recurrent painful ulcer on the penis Herpes Simplex Virus (HSV) (1) Most common cause of chronic or recurrent ulcers in the genital area Ulcers are more likely to be chronic in PLHIV Primary or recurrent episodic treatment: • Acyclovir 400 mg TID or 200 mg 5x per day x 7-10 days • Severe case: 5 mg/kg IV every 8 hours Chronic suppressive treatment: • Acyclovir 200 mg TID or 400 mg BID 11 Herpes Simplex Virus (HSV) (2) Chronic ulcer on scrotum Chronic ulcer on hand What is the Diagnosis? This patient presented with a chronic red scaly rash on the forehead and face Seborrheic Dermatitis (1) Cause: Dermatophyte (fungal) Erythematous, papular to scaly rash CD4 < 500 Nasolabial fold, beard, hairlines Seborrheic Dermatitis (2) Treatment: Ketoconazole cream or shampoo Shampoos (tar, selenium sulfide) Low potency steroid cream (hydrocortisone or antifungal) Antiretroviral Therapy 15 What is the Diagnosis? This patient presented with a very itchy rash on the hands, ankles and abdomen Lesions were red and 1-2 mm in size There were no pustules or vesicles 16 Scabies (1) Cause: Sarcoptes Scabiei (mites) Symptoms: • Itchy, red, papular lesions • Linear “burrows”, often between fingers Commonly located on hands, wrists and ankles, and groin Norwegian Scabies • Severe form in PLHIV • Hyperkeratotic lesions 17 Scabies (2) Scabies (3) Treatment: Benzyl benzoate, DEP Permethrin 5%- safe for children >2 months Lindane 1%- not safe in young children or pregnancy Ivermectin 19 What is the Diagnosis? This patient presented with many small nodules on the face and neck. No pain or itching No fever or wasting 20 Molluscum Contagiosum (MC) (1) Caused by a viral infection (MC virus) Spread by direct skin-to-skin contact Lesions: • Chronic, dome shaped papules (2 to 5 mm) • Shiny surface and central umbilication • Must differentiate from Penicillium and Cryptococcus Lesions can be found anywhere on the body except the palms and soles 21 Molluscum Contagiosum (2) Molluscum Contagiosum (3) Molluscum lesions on neck Treatment: Responds to ARV Cryotherapy: liquid nitrogen What is the Diagnosis? This patient presented with erythematous papules with central umbilication on the face and torso He also had fever, wasting and enlarged liver and spleen Penicillium marneffei (1) Common OI in Vietnam Occurs in advanced AIDS; CD4 < 100 Skin lesions: papules with central necrotic umblication 25 Penicillium marneffei (2) Lesions occur most commonly on the face Usually accompanied by systemic symptoms such as : • • • • Prolonged fever Fatigue Weight loss Hepatosplenomegaly Diagnosis: • Scraping skin lesions for staining and culture • Blood culture 26 What is the Diagnosis? This patient presented with a very itchy papular rash on the legs No fever or other symptoms Pruritic Papular Eruption (PPE) Itchy red papules 1-5 cm Etiology is unclear Differential diagnosis: • • • • • Bacterial infection (staphylococcus) Fungal infection TB Scabies Eosinophilic folliculitis Responds well to ARV 28 A B Identify the Skin Condition (1) C D Oral Mucosal Lesions 30 Oropharyngeal Candidiasis (Thrush) Common OI in Vietnam Diagnosis: clinical appearance Treatment: • Fluconazole 100150 mg/day x 7 days • Ketoconazole 200 mg bid x 7 days 31 Aphthous Ulcers Can be very large and painful in PLHIV Topical anesthetics for pain Topical steroids may decrease pain and swelling 32 Oral Hairy Leukoplakia Caused by Ebstein-Barr Virus (EBV) WHO Clinical stage 3 No treatment necessary Less Common Skin Conditions Eosinophilic Folliculitis Cryptococcal Infection Bacillary Angiomatosis Kaposi’s Sarcoma 34 Eosinophilic Folliculitis Chronic pruritic skin eruption Occurs with low CD4 counts (< 200) Etiology is unknown Clinical findings: • Pruritus: moderate-tosevere • Follicular papules on face, neck, upper trunk Disseminated Cryptococcus Skin lesions occur in up to 15% of patients Lesions may present as: • small nodules or papules that subsequently ulcerate, or • abscesses, erythematous nodules, or cellulitis Treatment: • Amphotericin B • Fluconazole Bacillary Angiomatosis Vascular lesions in skin and other organs Caused by infection with Bartonella species Lesions are red to purple papules or nodules Treatment: • Doxycycline, erythromycin or azithromycin x > 2 months Kaposi’s Sarcoma Vascular tumor associated with infection with human herpes virus 8 (HHV-8) Typically involves skin, but can involve any organ Skin lesions are red to purple dermal papules, nodules, tumors, or plaques Treatment: • Most respond to ART • Chemotherapy for severe cases E F Identify the Skin Condition (2) G H Key Points Skin conditions are very common in PLHIV, but can be difficult to diagnose If treatment is not effective, biopsy may be necessary to make a diagnosis Most skin conditions will improve with ART 40 Thank you! Questions? 41