Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Globalization and disease wikipedia , lookup
Behçet's disease wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Osteochondritis dissecans wikipedia , lookup
Common cold wikipedia , lookup
Neonatal infection wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Herpes simplex wikipedia , lookup
Hepatitis C wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Infection control wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Hepatitis B wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
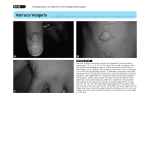
MOLLUSCUM CONTAGIOSUM Molluscum is a benign viral skin infection that is caused by the DNA pox virus. It affects both children and adults and spreads through close direct contact or contact with contaminated objects e.g. towels. The incubation period can vary between 7 days and 6 months. Diagnosis: Characteristic discrete pearly smooth lesions, often with an umbillicated centre. No need for laboratory confirmation. It can be associated with eczema. Management: Offer STI testing if appropriate. Most lesions spontaneously regress/crust over in 3-9 months, although secondary bacterial infection can occur if lesions are scratched. Treatment is offered for cosmetic reasons only. In adults with facial lesions, consider HIV testing. In clients with immunodeficiency due to HIV infection, anti retroviral therapy may assist in resolution of lesions. General Advice: Patients must be warned of risks of autoinoculation and, for example, advised against shaving or waxing their genital regions, to prevent further spread of lesions. Similarly, patients should be advised against squeezing molluscum spots, both due to risk of super-infection and also as the central plug is full of infectious virus which is easily spread to uninfected skin. Towels, bed-linen, clothes etc. should not be shared when active lesions are present, to reduce risk of onward transmission. Lesions should be covered with waterproof bandages or clothes, if possible, prior to using swimming pools. With genital molluscum, condoms may reduce transmission, but this is not absolute. Treatment: Clients may opt for no treatment and await spontaneous regression. Cryotherapy with liquid nitrogen. The aim is tissue (viral) destruction. This is also suitable for pregnant women. Apply for 5 – 10 seconds. Repeat at weekly intervals as necessary. There are no reported trials on its efficacy in treatment of molluscum. There is one randomised controlled trial demonstrating the efficacy of Podophyllotoxin in treating genital molluscum, and evidence of efficacy of Imiquimod in treating molluscum in both HIV positive and negative patients. Second line treatments for self-application (unlicensed): Podophyllotoxin cream (0.5%) for men and nonpregnant women or Imiquimod cream 5% for men and non-pregnant women (please discuss with senior clinician first) should we change imiquimod and podophyllotoxin to first line treatments in individuals with no risk of pregnancy in light of this evidence? Follow-up and Partner Notification: No need for partner notification. No specific follow-up. References: BASHH. Management of Molluscum Contagiosum. New Guidelines June 2014.. Molluscom Contagiosum CEG Dec 2014