Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
به نام خدا
دکتراقازاده
General aspect:
o Worldwide more than
2 billion people are infected
with helminthes.
o Classification helminthes of :
1. Nematodes (roundworm)
2. Platy helminthes:
• Tissue nematodes
• Intestinal nematodes
• Trematodes
• Cstodes
Intestinal Nematodes
o
Ascariasis (1)
• Causal Agents:
– Ascaris lumbricoides is the most common and the
largest nematode ( giant roundworm )
parasitizing the human intestine. (Adult females: 20 to
35 cm; adult male: 15 to 30 cm.)
Ascaris lumbricoides Life Cycle:
Geographic Distribution:
Worldwide distribution.
Highest prevalence in tropical and subtropical
regions, and areas with inadequate sanitation.
Clinical Features:
adult worms usually cause no acute symptoms.
High worm burdens may cause abdominal pain
and intestinal obstruction.
Migrating adult worms may cause symptomatic
occlusion of the biliary tract or oral expulsion.
During the lung phase of larval migration,
pulmonary symptoms can occur (cough,
dyspnea, hemoptysis, eosinophilic pneumonitis Loeffler’s syndrome).
Laboratory Diagnosis:
– Microscopic identification of eggs in the stool is the
most common method for diagnosing intestinal
ascariasis. Where concentration procedures are not
available, a direct wet mount examination of the
specimen is adequate fore detecting moderate to
heavy infections.
– Larvae can be identified in sputum or gastric
aspirate during the pulmonary migration phase.
– Adult worms are occasionally passed in the stool or
through the mouth or nose and are recognizable by
their macroscopic characteristics.
Below are several Ascaris eggs seen in wet mounts. Diagnostic characteristics:
•Fertilized eggs are rounded, thick shell, external mammillated layer Size: 60 µm in
diameter when spherical, and up to 75 µm when ovoid.
•Unfertilized eggs are elongated and larger (up to
90 µm in length); their shell is thinner; and their
mammillated layer is more variable
Unfertilized and fertilized eggs
(left and right, respectively).
Fertilized Ascaris
egg, still at the
unicellular
stage.Eggs are
normally at this
stage when passed
in the
stool.Complete
Egg containing a
development of larva, which will be
the larva
infective if
requires 18 days ingested.
under favorabl
Larva hatching
from an egg
Diagnostic characteristics:
tapered ends; length 15 to 35
cm. This worm is a female(size
and genital girdle )
Treatment:
•
The drugs of choice for treatment of
ascariasis are:
•
•
•
- Albendazole (400mg once),
- Mebendazole (500 mg once or 100mg BID for 3 days),
- pyrantel pamoate(11mg/kg once; maximum 1g – safe in
pregnancy).
Hookworms
•
Causal Agent:
• - The human hookworms include two nematodes :
•
•
Ancylostoma duodenale
Necator americanus
• - A smaller group of hookworms infecting animals
can invade and parasitize humans (A. ceylanicum) or
can penetrate the human skin (causing cutaneous
larva migrans), but do not develop any further (A.
braziliense, Uncinaria stenocephala).
hookworms Life Cycle:
Geographic Distribution:
o
o
- The second most common human helminthic infection
- Worldwide distribution, mostly in areas with moist, warm
climate. Both N. americanus and A. duodenale are found in
Africa, Asia and the Americas. Necator americanus
predominates in the Americas and Australia, while only A.
duodenale is found in the Middle East, North Africa and
southern Europe.
Clinical Features:
o
o
o
o
- Iron deficiency anemia (caused by blood loss at the site
of intestinal attachment of the adult worms) is the most
common symptom of hookworm infection, and can be
accompanied by cardiac complications.
- Gastrointestinal and nutritional/metabolic symptoms can
also occur.
- In addition, local skin manifestations ("ground itch") can
occur during penetration by the filariform (L3) larvae,
- and respiratory symptoms can be observed during
pulmonary migration of the larvae.
Laboratory Diagnosis:
- Microscopic identification of eggs in the
stool is the most common method for
diagnosing hookworm infection.
Treatment:
o - In countries where hookworm is common and
reinfection is likely, light infections are often not
treated.
o
Albendazole (400mg once).
Mebendazole (500mg once). or
pyrantel pamoate(11mg/kg for 3 days)
Strongyloidiasis
• Causal Agent:
•
•
Strongyloid Stercolaris
Other Strongyloides include S. fülleborni, which
infects chimpanzees and baboons and may
produce limited infections in humans.
Strongyloidiasis Life Cycle:
Geographic Distribution:
o
o
Tropical and subtropical areas, but cases also
occur in temperate areas
More frequently found in rural areas, institutional
settings, and lower socio-economic groups.
Clinical Features:
Frequently asymptomatic.
Pulmonary symptoms (including Loeffler’s syndrome)
can occur during pulmonary migration of the
filariform larvae.
• Dermatologic manifestations include urticarial rashes
in the buttocks and wrist areas.
o Disseminated strongyloidiasis occurs in
immunosuppressed patients, can present with
abdominal pain, distension, shock, pulmonary and
neurologic complications and septicemia, and is
potentially fatal.
Blood eosinophilia is generally present during the
acute and chronic stages, but may be absent with
dissemination.
Laboratory Diagnosis:
Microscopic identification of
larvae ( rhabditiform and
occasionally filariform) in
the stool or duodenal fluid.
•
Examination of serial samples may be necessary,
and not always sufficient, because stool examination
is relatively insensitive.
The duodenal fluid can be examined using
techniques such as the Enterotest string or
duodenal aspiration.
– Larvae may be detected in sputum from patients
with disseminated strongyloidiasis.
Treatment:
The drug of choice for the treatment of
uncomplicated strongyloidiasis is :
Ivermectin(200μg/kg daily for 1 or 2 days),
Thiabendazole (25 mg/Kg bid 2days)
Albendazole (400mg daily for 3 days repeated
at 2 weeks), All patients are at risk of
disseminated strongyloidiasis and should be
treated.
Enterobiasis
•
Causal Agent:
•
•
Enterobius vermicularis (previously Oxyuris vermicularis)
also called human pinworm. (Adult females: 8 to 13 mm,
adult male: 2 to 5 mm.) Humans are considered to be the
only hosts of E. vermicularis. A second species
, Enterobius gregorii, has been described and reported
from Europe, Africa, and Asia. For all practical purposes, the
morphology, life cycle, clinical presentation, and treatment
of E. gregorii is identical to E. vermicularis.
Enterobius vermicularis Life Cycle:
Geographic Distribution :
• Worldwide, with infections more frequent in school-
or preschool- children and in crowded
conditions. Enterobiasis appears to be more
common in temperate than tropical countries.
•
Clinical Features:
•
•
•
Enterobiasis is frequently asymptomatic.
The most typical symptom is perianal pruritus, especially at
night, which may lead to excoriations and bacterial
superinfection.
Occasionally, invasion of the female genital tract with
vulvovaginitis and pelvic or peritoneal granulomas can
occur.
Other symptoms include anorexia, irritability, and abdominal
pain.
Laboratory Diagnosis:
– Scotch test", cellulose-tape slide test) on the
perianal skin and then examining the tape placed on
a slide.
– Anal swabs or "Swube tubes" can also be
used. Eggs can also be found, but less frequently, in
the stool, and occasionally are encountered in the
urine or vaginal smears.
• Adult worms are also diagnostic, when found in the
perianal area, or during ano-rectal or vaginal
examinations.
Laboratory Diagnosis:
Eggs measure 50 to 60 µm by 20 to 3 µm.
Anterior end of Enterobius
vermicularis adult worm.
Enterobius eggs on
cellulose tape prep.
•
Treatment:
•
- Mebendazole 100 mg once daily(single dose)
• Albendazole (400mg once)
•
pyrantel pamoate(11mg/kg once; maximum 1g
-Susp . 250 mg/ 5 ml,Tab. 125 mg– safe in pregnancy)
• PYRVINIUM PAMOATE (Coated Tab. 50 mg, Susp. 50
mg / 5 ml)
• Measures to prevent reinfection, such as personal
hygiene and laundering of bedding, should be
discussed and implemented in cases where
infection affects other household members.
Tissue Nematodes
Angiostrongylus Cantonensis
Dracunculiasis
Trichinella Spiralis
Angiostrongyliasis
Causal Agent:
The nematode (roundworm) Angiostrongylus
cantonensis, the rat lungworm, is the most
common cause of human eosinophilic
meningitis,
Angiostrongylus cantonensis Life Cycle:
Angiostrongyliasis
Geographic Distribution:
o
Most cases of eosinophilic meningitis have been reported from
Southeast Asia and the Pacific Basin, although the infection is
spreading to many other areas of the world, including Africa and
the Caribbean. Abdominal angiostrongyliasis has been reported
from Costa Rica, and occurs most commonly in young children.
Clinical Manifestations
•
- eosinophilic meningitis Symptoms include severe headaches,
•
Abdominal angiostrongyliasis mimics appendicitis, with
eosinophilia.
nausea, vomiting, neck stiffness, seizures, and neurologic
abnormalities. Occasionally, ocular invasion occurs. Eosinophilia
is present in most of cases. Most patients recover fully.
Laboratory Diagnosis:
o
In eosinophilic meningitis the cerebrospinal fluid (CSF) is abnormal
(elevated pressure, proteins, and leukocytes; eosinophilia). On
rare occasions, larvae have been found in the CSF.
o In abdominal angiostrongyliasis, eggs and larvae can be identified in
the tissues removed at surgery.
Treatment:
o
No drug has proven to be effective for the treatment of A.
cantonensis or A. costaricensis infections. Relief of symptoms
for A. cantonensis infections can be achieved by the use of
analgesics, corticosteroids, and careful removal of the cerebral
spinal fluid at frequent intervals.
Trichinellosis
Etiology
Epidemiology
Life cycle
Clinical Manifestation
Laboratory Finding
Treatment
trichinellosis
Dracunculiasis
Causal Agent:
guinea worm disease is caused by the nematode (roundworm)
Dracunculus medinensis
Geographic Distribution:
An ongoing eradication campaign has dramatically
reduced the incidence of dracunculiasis, which is now
restricted to rural, isolated areas in a narrow belt of
African countries and Yemen.
Dracunculus medinensis Life Cycle:
Dracunculiasis
Clinical Features:
o
The clinical manifestations are localized but
incapacitating. The worm emerges as a whitish
filament (duration of emergence: 1 to 3 weeks) in
the center of a painful ulcer, accompanied by
inflammation and frequently by secondary bacterial
infection.
Dracunculiasis
Laboratory Diagnosis:
The clinical presentation of dracunculiasis is so typical,
and well known to the local population, that it does not
need laboratory confirmation. In addition, the disease
occurs in areas where such confirmation is unlikely to
be available. Examination of the fluid discharged by
the worm can show rhabditiform larvae. No serologic
test is available.
Treatment:
Local cleansing of the lesion and local application of
antibiotics, if indicated because of bacterial
superinfection. Mechanical, progressive extraction of
the worm over a period of several days. No curative
antihelminthic treatment is available.
Trematodes
o Blood Flukes
o
Liver Flukes
o
Intestinal Flukes
o
Lung Flukes
Blood Flukes
(Schistosomiasis)
S .Mansomi
S .Intercalatum
S .Hematubium
S .Japonicum
S .Mekongi
Epidemiology
S .Mansoni
S .Japonicum
West Africa
S .Mekongi
China .Philippines .Indonesia
S .Intercalatum
Africa .SousAmerica .Middle East
Southeast Asia
S .Haematobium
Africa .Middle East
Life cycle
Clinical Manifestation
Cercarial Dermatitis
Acute Schistosomiasis- Katayama Fever
Chronic Schistosomiasis
Cercarial Dermatitis
Dependent to species .Intensity of Infection
and host factors
Most often by S .mansoni &S .japonicum
2-3 days after invasion (swimmer itch)
Self- limiting entity
Acute Schistosomiasis
(Katayama Fever)
4-8 wks after skin invasion
Fever .lymphadenopathy .
Hepato- splenomegaly . Eosinophilia .
Generally benign
Death occasionally reported in heavy exposure
Chronic Schistosomiasis
Intestinal & Hepatosplenic Diseases :
S . japonicum .S.mansoni .S.intecalatum .
S .mekonky
– Intestinal diseases :
Colicky abdominal pain .Bloody diarrhea .Colonic polyposis
– Hepatosplenic Diseases :
Urinary tract Diseases
15-20 % of infected patients
Portal hypertension
Cirrhosis
S.haematobium
Hemturia .Dysuria .Bladder granoloma .Hydronephrosis Bladder CA
CNS Schistosomiasis
Pulmonary Schistosomiasis
Treatment
Liver Flukes
Fasciola Hepatica
Clonorchis Sinensis
Fascioliasis
• Causal Agent:
•
The trematodes Fasciola hepatica (the sheep liver
fluke) and Fasciola gigantica, parasites of
herbivores that can infect humans accidentally.
• Geographic Distribution:
•
Fascioliasis occurs worldwide. Human infections with F.
hepatica are found in areas where sheep and cattle are
raised, and where humans consume raw watercress,
including Europe, the Middle East, and Asia. Infections
with F. gigantica have been reported, more rarely, in Asia,
Africa, and Hawaii.
Fasciola hepatica Life cycle :
Fascioliasis
•
Clinical Features:
•
During the acute phase (caused by the migration of
the immature fluke through the hepatic
parenchyma), manifestations include abdominal
pain, hepatomegaly, fever, vomiting, diarrhea,
urticaria and eosinophilia, and can last for months.
In the chronic phase (caused by the adult fluke
within the bile ducts), the symptoms are more
discrete and reflect intermittent biliary obstruction
and inflammation.
Occasionally, ectopic locations of infection (such as
intestinal wall, lungs, subcutaneous tissue, and
pharyngeal mucosa) can occur.
Fascioliasis
o Laboratory Diagnosis:
o
Microscopic identification of eggs is useful in the
chronic (adult) stage. Eggs can be recovered in the
stools or in material obtained by duodenal or biliary
drainage.
False fascioliasis (pseudofascioliasis) refers to the
presence of eggs in the stool resulting not from an
actual infection but from recent ingestion of infected
livers containing eggs. This situation (with its
potential for misdiagnosis) can be avoided by having
the patient follow a liver-free diet several days
before a repeat stool examination.
Antibody detection tests are useful especially in the
early invasive stages, when the eggs are not yet
apparent in the stools, or in ectopic fascioliasis.
Fascioliasis (4):
Wet mounts with iodine.
The eggs are ellipsoidal.
They have a small, barely
distinct operculum Size range:
120 to 150 µm by 63 to 90 µm.
Treatment:
Unlike infections with other flukes, Fasciola
hepatica infections may not respond to
praziquantel. The drug of choice is
triclabendazole with bithionol as an alternative.
Intestinal Flukes
Fasciolopsis Buski
Heterophyes Heterophyes
Lung Flukes
Paragonimus Westermani
Paragonimus Africanus
Cestods
Teniasis Saginata
Teniasis Solium &Cysticercosis
Hymenolepiasis Nana
Echinococcosis
Taeniasis
Causal Agent:
The cestodes (tapeworms) Taenia saginata (beef tapeworm) and T.
solium (pork tapeworm). Taenia solium can also cause cysticercosis.
Geographic Distribution:
Both species are worldwide in distribution. Taenia solium is
more prevalent in poorer communities where humans live in
close contact with pigs and eat undercooked pork, and in very
rare in Muslim countries.
Life cycle of Taenia saginata
and Taenia solium :
Taeniasis
•
Clinical Features:
• - Taenia saginata taeniasis produces only mild abdominal
symptoms. The most striking feature consists of the passage
(active and passive) of proglottids. Occasionally, appendicitis
or cholangitis can result from migrating proglottids.
•
- Taenia solium taeniasis is less frequently symptomatic
than Taenia saginata taeniasis. The main symptom is
often the passage (passive) of proglottids. The most
important feature of Taenia solium taeniasis is the risk
of development of cysticercosis.
Taeniasis
Laboratory Diagnosis:
- Microscopic identification of eggs and
proglottids in feces is diagnostic for taeniasis,
but is not possible during the first 3 months
following infection, prior to development of
adult tapeworms.
- Microscopic identification of gravid
proglottids(or,more rarely,examination of the
scolex)allows species determination.
- Antibody detection may prove useful
especially in the early invasive stages
Taeniasis
Treatment:
Treatment is simple and very effective.
Praziquantel (10mg /kg)is the drug of
choice.
NICLOSAMIDE (4 tab single dose)
Cycticercosis
echinococcosis
Causal Agent:
•
Human echinococcosis (hydatidosis, or hydatid
disease) is caused by the larval stages of cestodes
(tapeworms) of the genus Echinococcus.
• - Echinococcus granulosus causes cystic
echinococcosis, the form most frequently
encountered;
• - E. multilocularis causes alveolar echinococcosis; E.
vogeli causes polycystic echinococcosis; and E.
oligarthrus is an extremely rare cause of human
echinococcosis.
Echinococcus Life Cycle:
echinococcosis
Geographic Distribution:
•
occurs practically worldwide, and more frequently in rural,
grazing areas where dogs ingest organs from infected
animals. E. multilocularis occurs in the northern hemisphere,
including central Europe and the northern parts of Europe, Asia,
and North America.
E. vogeli and E. oligarthrus occur in
Central and South America.
Clinical Features:
– Echinococcus granulosus infections remain silent for years
before the enlarging cysts cause symptoms in the affected
organs.
• Hepatic involvement can result in abdominal pain, a mass in
the hepatic area, and biliary duct obstruction.
• Pulmonary involvement can produce chest pain, cough, and
hemoptysis. .
• Rupture of the cysts can produce fever, urticaria,
eosinophilia, and anaphylactic shock, as well as cyst
dissemination.
• In addition to the liver and lungs, other organs (brain, bone,
heart) can also be involved, with resulting symptoms.
• Echinococcus multilocularis affects the liver as a slow
growing, destructive tumor, with abdominal pain, biliary
obstruction, and occasionally metastatic lesions into the lungs
and brain.
• Echinococcus vogeli affects mainly the liver, where it acts as
a slow growing tumor; secondary cystic development is
common
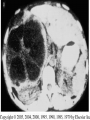
Laboratory Diagnosis:
The diagnosis of echinococcosis relies mainly on
findings by ultrasonography and/or other imaging
techniques supported by positive serologic tests. .
- In seronegative patients with hepatic image findings
compatible with echinococcosis, ultrasound guided fine
needle biopsy may be useful for confirmation of
diagnosis; during such procedures precautions must be
taken to control allergic reactions or prevent secondary
recurrence in the event of leakage of hydatid fluid or
protoscolices
Treatment:
- Surgery is the most common form of treatment for
echinococcosis, although removal of the parasite mass
is not usually 100% effective. After surgery,
medication may be necessary to keep the cyst from
recurring.
- The drug of choice for treatment echinococcosis is
albendazole (Echinococcus granulosus). Some reports
have suggested the use of albendazole or mebendazole
for Echinococcus multilocularis infections.
Hymenolepiasis(1):
Causal Agents:
Hymenolepiasis is caused by two cestodes
(tapeworm) species:
- Hymenolepis nana (the dwarf tapeworm,
adults measuring 15 to 40 mm in length)
- Hymenolepis dimnuta (rat tapeworm,
adults measuring 20 to 60 cm in
length). Hymenolepis diminuta is a cestode
of rodents infrequently seen in humans and
frequently found in rodents.
Hymenolepis nana Life Cycle:
Hymenolepiasis(2):
Geographic Distribution:
Hymenolepis nana is the most common cause
of all cestode infections, and is encountered
worldwide. In temperate areas its incidence is
higher in children and institutionalized groups.
Hymenolepis diminuta, while less frequent, has
been reported from various areas of the world.
Hymenolepiasis(3):
•Clinical Features:
Hymenolepis nana and H. diminuta infections
are most often asymptomatic. Heavy infections
with H. nana can cause weakness, headaches,
anorexia, abdominal pain, and diarrhea.
•Laboratory Diagnosis:
The diagnosis depends on the demonstration of eggs in
stool specimens. Concentration techniques and
repeated examinations will increase the likelihood of
detecting light infections.
Egg of Hymenolepis
diminuta,round or slightly oval,
size 70 to 86 µm X 60 to 80 µm,
with a striated outer membrane and
a thin inner membrane. The space
between the membranes is smooth
or faintly granular. The oncosphere
has six hooks.
Egg of Hymenolepis nana,oval
or subspherical and smaller than
those of H. diminuta, their size being
40 to 60 µm X 30 to 50 µm. On the
inner membrane are two poles, from
which 4 to 8 polar filaments spread
out between the two
membranes. The oncosphere has six
hooks.
Hymenolepiasis(4):
Treatment:
- Praziquantel (25mg/kg once, F.C. Tab.
600mg ) is the drug of choice.
- NICLOSAMIDE (4 tab daily for 5-7
days,Chewable Tab 500 mg)
Diphyllobothriasis(1):
Causal Agent:
The cestode Diphyllobothrium latum (the fish
or broad tapeworm), the largest human
tapeworm. Several other Diphyllobothrium
species have been reported to infect humans,
but less frequently; they include D. pacificum,
D. cordatum, D. ursi, D. dendriticum, D.
lanceolatum, D. dalliae, and D. yonagoensis.
Diphyllobothrium latum Life Cycle:
Diphyllobothriasis(2):
Geographic Distribution:
Diphyllobothriasis occurs in areas where lakes and rivers
coexist with human consumption of raw or undercooked
freshwater fish. Such areas are found in the Northern
Hemisphere (Europe, newly independent states of the
former Soviet Union (NIS), North America, Asia), and in
Uganda and Chile.
Clinical Features:Diphyllobothriasis can be a long-
lasting infection(decades).
- Most infections are asymptomatic.
- Manifestations may include abdominal discomfort,
diarrhea, vomiting, and weight loss.
-Vitamin B12 deficiency with pernicious anemia may occur.
- Massive infections may result in intestinal obstruction.
- Migration of proglottids can cause cholecystitis or
cholangitis.
Diphyllobothriasis(3):
Laboratory Diagnosis:
- Microscopic identification of eggs
in the stool is the basis of specific
diagnosis.Eggs are usually numerous
and can be demonstrated without
concentration techniques.
- Examination of proglottids passed
in the stool is also of diagnostic value.
Treatment:
Praziquantel is the drug of
choice.
Alternatively, Niclosamide
can also be used to
treat diphyllobothriasis.
oval or
ellipsoidal,
with at one
end an
operculum.
The eggs are
passed in the
stool
unembryonat
ed. Size
range: 58 to
76 µm by 40
to 51 µm