Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Clinical Science (1971) 41, 419-439.
THE REFLEX STIMULATION OF CATECHOLAMINE
SECRETION DURING THE ACUTE STAGE OF
MYOCARDIAL INFARCTION IN THE DOG
JANINA STASZEWSKA-BARCZAK
Laboratory of Neurophysiology, Polish Academy of Sciences,
Medical Research Centre, Warsaw
(Received 13 Jtl1IUIlI'J' 1971)
SUMMARY
1. The mechanism of catecholamine secretion after coronary occlusion was
investigated in open-chest, anaesthetized dogs; the blood-bathed organ technique
was used for continuous measurement of the changes in concentration of circulating
catecholamines.
2. In dogs with increased output of adrenaline during the first hour after acute
coronary occlusion, topical application of lignocaine to the infarcted area of the
heart, spinal block at C t , bilateral section of thoracic splanchnic nerves, or ganglionic
blockade virtually abolished adrenaline secretion.
3. Adrenaline secretion was abolished by bilateral vagotomy in 50% of the dogs,
decreased in 28% and unchanged in the remaining 22%. Bretylium or guanethidine
had no effect on adrenaline secretion in the early stages of myocardial infarction.
4. Seventeen of nineteen reserpinized dogs failed to secrete catecholamines during
the first hour of coronary occlusion, even though the adrenal medulla responded to
bradykinin, acetylcholine or nicotine. Noradrenaline infused either into the unoccluded carotid artery or intravenously restored adrenal medullary secretion.
5. When a sustained noradrenaline release occurred after coronary ligation, it was
abolished by topical application of lignocaine to the ischaemic area of the heart or
by ganglionic blockade. Neither bilateral vagotomy nor section of both thoracic
splanchnic nerves suppressed noradrenaline liberation.
6. It is concluded that the adrenal medullary secretion of adrenaline which occurs
in the early stages of myocardial infarction in the dog is induced reflexly from
stimulation of cardiac receptors at the site and the boundary of the infarct. The
reflex involves vagal as well as extra-vagal pathways and supraspinal structures.
Enhanced liberation of noradrenaline in the early stage of infarction may reflect
release from postganglionic sympathetic nerve endings in the heart.
Correspondence: Dr J. Staszewska-Barczak, Laboratory of Neurophysiology, Polish Academy of Sciences,
Medical Research Centre, Warsaw 36, Dworkowa 3, Poland.
419
420
Janina Staszewska-Barczak
Several suggestions have been made to explain the increase in sympatheticoadrenal activity in
the acute stage of myocardial infarction. The increased discharge of catecholamines in man
could be due to severe pain, tissue damage or circulatory disturbances (Sofieva, 1965; Jewitt,
Mercer, Reid, Valori, Thomas & Shillingford, 1969). Because high concentrations of both
adrenaline and noradrenaline were found in patients with myocardial infarction associated
with pulmonary oedema, it was suggested that increased adrenergic drive could arise reflexly
from stimulation of receptors in the left atrium or pulmonary venous system (Jewitt et al.,
1969). Others have suggested that augmented adrenal medullary activity was related to a poor
perfusion of the adrenal glands, neurogenic influences, or unknown chemical factors (Hayashi,
Moss & Yu, 1969). Relatively little attention has been paid to the possibility of nervous
reflexes arising from the infarcted area of myocardium.
We have previously shown that within minutes of producing an experimental myocardial
infarct by acute coronary ligation in the dog, the adrenal medulla begins to secrete catecholamines, mainly adrenaline. It seemed unlikely that this outpouring of adrenaline, found
in about 60% of dogs, was due to baroreceptor activation, since it could occur without change
in the mean arterial blood pressure (Staszewska-Barczak & Ceremuzynski, 1968). In dogs
severe haemorrhage of up to a third of the calculated blood volume may fail to produce
detectable change of catecholamine secretion rate in spite of striking falls of arterial blood
pressure (Hodge, Lowe & Vane, 1966). Also strong baroreceptor reflex activation induced by
carotid occlusion in dogs was accompanied by a much smaller secretion of catecholamines
from the adrenal medulla (Hodge, Lowe & Vane, 1969) than we find after myocardial infarction. Thus, even in those experiments in which acute coronary occlusion was followed by a
transient or prolonged fall of arterial pressure, it is unlikely that baroreflex activation could
be responsible for sustained adrenaline secretion. We suggested that the excitation of the
adrenal medulla is mediated by undefined humoral changes, by reflexes arising from the
infarcted area of the myocardium, or by both mechanisms.
Increased adrenal medullary secretion can be evoked reflexly (Houssay & Molinelli, 1925a;
Kaindl & Euler, 1951; Euler & Folkow, 1953) as well as directly or indirectly by various
endogenous blood-borne substances such as bradykinin, angiotensin, histamine and 5-hydroxytryptamine (see Vane, 1969). Brown (1967) demonstrated an increased discharge of afferent
cardiac nerves within seconds of coronary ligation in cats, whereas in dogs increased firing
and other changes have been observed in afferent fibres of the cervical vagus which originated
from the myocardium in the area of a chemically induced infarct (Kolatat, Ascanio, Tallarida
& Oppenheimer, 1967). The concentration of 5-hydroxytryptamine in blood is elevated during
the first hours after acute coronary ligation in dogs (Senderoff, Warner & Baronofsky, 1962),
so that chemical stimulation of the adrenal medulla is also possible.
The following experiments were designed to define the role of reflex mechanisms in the
induction and maintenance of catecholamine secretion in the early stages of myocardial
infarction in the dog. As in our previous study (Staszewska-Barczak & Ceremuzynski, 1968)
we used the sensitive bioassay method of Vane (1964, 1969) to follow the release and disappearance of catecholamines in the circulating blood.
METHODS
Mongrel dogs of either sex weighing 6-15 kg were anaesthetized with hexobarbitone sodium
(40 mg/kg i.v.); anaesthesia was maintained with chloralose (100 mg/kg i.v.). Positive pressure
Catecholamines in myocardial infarction
421
respiration was maintained with a Starling pump and the chest was opened in the midline by
sternal section.
The dogs were heparinized (Heparinum, Polfa 1000 units/kg i.v.) and the carotid artery was
cannulated with polyethylene tubing to supply blood to an extracorporeal circulation for
determination of catecholamine concentrations and to record arterial pressure by mercury
manometer. Electrocardiograms from standard leads (I, II and III) were recorded from needle
electrodes in the extremities with an Elema-Schonander Mingograf 42B. Coronary occlusion
was induced by ligation of the anterior descending branch of the left coronary artery.
The blood-bathed organ technique (Vane, 1964, 1969) was used to measure changes in the
concentration of adrenaline and noradrenaline in circulating blood which was taken at a rate
of 10 nil/min from the carotid artery. The blood superfused an isolated rat stomach strip
(Vane, 1957) which relaxes to both adrenaline and noradrenaline, and an isolated chick rectum
(Mann & West, 1950) which relaxes only to adrenaline. The blood was collected in a reservoir
and returned to the animal through a cannula in a jugular vein. When these assay tissues are
superfused in series it is possible to distinguish between the release of adrenaline and noradrenaline (Armitage & Vane, 1964). The concentrations of catecholamines in the circulation
are determined by comparing the effects of the released amines on the blood-bathed organs
with the effects of intravenous infusions of known quantities of either adrenaline or noradrenaline.
In dogs that showed increased output of catecholamines into the circulation during the first
hour after acute coronary occlusion the following procedures were applied.
Local epicardial application of lignocaine. A piece of gauze soaked with a solution of lignocaine (2% or 5%) was placed on the infarcted area of the left ventricle (including its borders)
for 5 min. In some experiments, lignocaine-soaked gauze pads were placed on the left lung
for 5 min, before epicardial application.
Vagotomy. Bilateral vagotomy was performed either by cutting the vagi in the neck or by
blocking conduction by surrounding the desheathed nerves for 5 min with cotton cuffs soaked
with lignocaine (5%).
Spinal block. At the beginning of the experiment the skin and muscles of the neck were
dissected to expose the atlanto-occipital membrane. Later spinal cord transmission was
interrupted by injecting 2 ml of lignocaine (5%) through the membrane into the cord.
Splanchnic nerve section. The thoracic splanchnic nerves were transected in the thorax on
both sides at the level of the ninth rib before their entry into the abdominal cavity.
Ganglionic blockade. Pentolinium tartrate (1-2 mg/kg) or chlorisondamine chloride (0'5
rug/kg) was injected intravenously.
Adrenergic neurone blockade. Bretylium tosylate (5 mg/kg) or guanethidine sulphate (5 mg/
kg) was injected intravenously either 1 h before coronary ligation or later in the experiment
at the time of increased catecholamine secretion.
Reserpinized dogs. Reserpine was injected intraperitoneally (0'25 or 0·5 mg/kg) on each of
the two days before the experiment.
Drugs
The following drugs were used; doses of salts are expressed as base: acetylcholine hydrochloride (British Drug Houses), (- )adrenaline bitartrate (British Drug Houses), bradykinin
(Sandoz), bretylium tosylate (Darenthin, Ciba), chlorisondamine chloride (Ecolid, Ciba) ,
Janina Staszewska-Barczak
422
guanethidine sulphate (Ismelin, Ciba), (- )noradrenaline bitartrate (Bayer Products), pentolinium tartrate (May and Baker), reserpine (Rausedyl, Gedeon Richter), lignocaine (Xylocaine,
Astra).
RESULTS
Effect of local application of lignocaine to the infarcted area of the myocardium
In seven dogs in which acute coronary ligation was followed by adrenaline release into the
circulation, the application of gauze soaked with lignocaine directly to the ischaemic region of
the myocardium resulted in a rapid decline of adrenaline secretion. In six of the seven dogs
this procedure led to complete cessation of adrenaline secretion for at least 45 min, and in
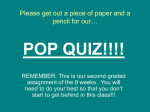
the remaining dog the release of adrenaline was greatly decreased. Fig. I shows an experiment
min
[TTTIl1TTTl
C.R.
RS.S
140!
flOO
8.P.
60
Ad
~
If'g/min
Lv.
•
•
Lig. Cor. occl,
Ad
L.-..,
L--...,
Lign.
2f'g/min
i.v,
FIG. 1. Release of adrenaline after coronary ligation with suppression of response after application
of lignocaine to the ischaemic myocardium. The tracings show from above down the responses
of the superfused chick rectum (C.R.) and rat stomach strip (R.S.S.), and arterial pressure (B.P.).
Ad = calibrating infusions of adrenaline. Lig, (dot) = insertion of ligature, with occlusion of
the artery at the arrow. Lign, = application of gauze soaked with 5% lignocaine to ischaemic
area. Further details are given in the text.
in which occlusion of the coronary artery led to a gradual relaxation of both isolated bloodbathed organs, indicating release of adrenaline into the circulation. Secretion was sustained at
a rate of 2 jig/min, but was abolished when lignocaine was applied to the ischaemic region of
the heart, as indicated by contraction and stabilization of the assay organs at the initial
baseline. To make sure that lignocaine applied locally does not have a direct contracting effect
on the assay organs as a result of absorption into the circulation, lignocaine-soaked gauze
pads were placed for 5 min on the lung surface before being placed on the epicardium. This
was done in three experiments in which adrenaline secretion had been induced by occlusion
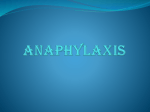
of the coronary artery. The results from one of these experiments is shown in Fig. 2: there was
no change in the assay tissues on application of lignocaine to the lung, showing that any
Catecholamines in myocardial infarction
423
lignocaine that might have been absorbed into the circulation did not reach a concentration
adequate to have a direct contracting action on the isolated assay tissues. Subsequent application of lignocaine-soaked gauze to the infarcted area of the myocardium for a similar period
of time (5 min) resulted in a rapid return of both assay organs to the initial base line, indicating
cessation of adrenaline secretion. Similar results were obtained in two other experiments.
The effects of local application of lignocaine to the ischaemic heart were also studied in two
dogs which showed an elevated release of noradrenaline after coronary ligation. In one of
min
rmrrmn
C.R.
R.S.S.
f
140
B P.
100F
60
E
~
~
4jLg/min 2jLg/min
IV
IV.
.~
,Lign;
,Lign:
~
on the
lung
on the
heart
2jLg/min
I.V.
FIG. 2. Lack of effect on adrenaline secretion of lignocaine applied to lung, with subsequent
complete suppression after application to ischaemic area. Tracings, calibration and abbreviations
as in Fig. I.
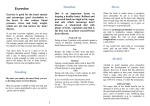
these dogs (Fig. 3) occlusion of the coronary artery led to almost immediate relaxation of the
rat stomach strip but not of the chick rectum, though both tissues were relaxed by intravenous
infusions of adrenaline. This differential effect on the rat stomach strip showed secretion of
noradrenaline into the circulation. The first application of lignocaine to the ischaemic heart
led to a partial decrease of noradrenaline secretion; 40 min later a second application of
lignocaine completely abolished the noradrenaline release. This experiment also shows that
any lignocaine that might have been absorbed into the circulation did not have a direct
contracting action on the assay tissues. In the other dog, the first application of lignocaine to
the infarcted myocardium completely suppressed noradrenaline liberation.
Effect of bilateral vagotomy
Both vagi were sectioned in twelve dogs which had undergone coronary ligation and were
showing substantial and sustained release into the circulation of adrenaline (eight dogs),
noradrenaline (two dogs) or a mixture of both amines (two dogs). In five of the ten dogs in
which adrenaline was secreted, either alone or as a mixture with noradrenaline, vagotomy
induced complete cessation of adrenaline release after a delay of 25-30 min. In three dogs the
Ad.
4,u.g/min
i.v
I
I...-,
Lign.
Nor
I...-,
L...-,
Nor
..\1.
I.v.
Lign. 4,u.q/min 8,u.<J/min
L...-,
90min
min
Lign.
L....,
jliliiiiili
L...,
2,u.g/min
Lv.
Ad
RS.S.
FIG. 3. Release of noradrenaline after coronary ligation with decrease and subsequent abolition of secretion after application of
lignocaine to the ischaemic myocardium. Tracings, calibration and abbreviations as in Fig. 1. Note that application of lignocaine
to ischaemic myocardium at the end of the experiment had no effect on the assay organs.
E 60
E 40
~ 100~
80
50m[
50 min
~
~
~
~
~
~
~
e
~
~
;::s
~.
~
Catecholamines in myocardial infarction
425
secretion of adrenaline was decreased by vagotomy to about one-half of the previous rate; in
the other two dogs it remained unchanged. No decline in the concentration of circulating
noradrenaline was detected after bilateral vagotomy when this amine was secreted either alone or
mixed with adrenaline (four dogs). Both adrenal glands were removed at the end of the experiment in two of these four dogs; this neither decreased nor abolished noradrenaline secretion.
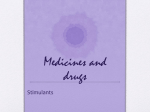
The decrease or abolition of adrenaline release did not immediately follow vagotomy, but
was delayed by up to 30 min (Fig. 4). This delay may have arisen as a result of injury currents
at the cut end of the nerve which enabled it to continue to generate impulses that were transmitted centrally. To avoid an effect of this sort, experiments were performed in which vagal
traffic was interrupted chemically with 5% lignocaine.
Eight dogs were studied in which increased liberation of adrenaline had been induced in
six and of adrenaline and noradrenaline in two. In four dogs, blockade of the vagus nerves
with lignocaine rapidly and completely abolished the adrenaline secretion (Fig. 5). In two dogs
adrenaline secretion was decreased but not abolished, and in the remaining two animals
despite blockade and subsequent section of both vagi increased release of adrenaline persisted
until the end of the experiment. Noradrenaline secretion was not abolished by blockade of
the vagus nerves with lignocaine. In one dog bilateral adrenalectomy also failed to abolish
noradrenaline release.
Thus, interruption of both cervical vago-sympathetic nerves either by nerve section or by
blockade with lignocaine effectivelyabolished adrenaline secretion evoked by coronary ligation
in nine out of eighteen dogs; it decreased adrenaline release in five dogs but was without effect
in the remaining four (Table 1). Vagotomy was ineffective in suppressing elevated noradrenaline
secretion.
Effect of spinal block
Four dogs showing sustained increases in concentration of adrenaline in the blood during
the first hour of coronary ligation were injected with 2 ml of lignocaine (5%) into the spinal
cord at C 1 • In all animals there was a rapid return of assay tissues to their initial baseline
showing that adrenal medullary secretion had been stopped (Fig. 6).
Effect of thoracic splanchnic nerve section
Transection of the thoracic splanchnic nerves abolished the secretion of adrenaline induced
by coronary ligation (three dogs).
In one dog coronary occlusion evoked liberation of noradrenaline at a rate of 2 p.g/min.
This secretion was unaffected by section of the splanchnic nerves.
Effect ofganglion-blocking agents
In eight dogs with sustained secretion of adrenaline (0'5-4 p.gfmin) induced by coronary
ligation, pentolinium (1-2 mgfkg i.v.) abolished the secretion. In the experiment shown in
Fig. 7, for example, adrenaline secretion occurred when the ligature was merely inserted under
the coronary artery; the secretion was maintained at about 1 p.g/min for approx. 15 min and
then waned; it reappeared after coronary occlusion. During the next 35 min the rate of
adrenaline secretion gradually increased and when it was at about 4 p.g/min, pentolinium was
injected intravenously. This produced immediate contraction and then stabilization of both
isolated organs at their initial baseline, showing a complete inhibition of adrenaline release.
<m[
E
<,
0>
<,
(\J
::l
0'
J-
'E
Ad
c
Ad
c
'f
L.....,
L-.,
i.v.
::l
ot
0>
'f<,
L....,
Nor
c
Ad
::l
"0'
'f
c
•
Lig.
L-.,
•
Cor. occl.
y
}(
Vagofomy
}(
R.S.S.
C.R.
FIG. 4. Release of adrenaline after coronary ligation with abolition of response 25 min after vagotomy. Tracings and abbreviations as in Fig. I. Calibration includes noradrenaline (Nor) in addition to adrenaline (Ad) and differential sensitivity of assay
tissues is shown.
60
~12°f
E 80
5
min
TTTT"
~
I
~
Ia
~.
~
~
~
427
Catecholamines in myocardial infarction
min
rrrrrrrrrn
C.R.
B,P'
~
Lign.-Vog.
FIG. 5. Release of adrenaline after coronary ligation with rapid suppression of response after
blockade of vagi with 5% lignocaine. Tracings, calibration and abbreviations as in Fig. I, except
that rat stomach strip is not shown. Lign.-Vag. = application of 5% lignocaine to both vagi.
C.R.
R.S.S.
B.P.
Li9.·~
Cor. occl,
L,
Spinal
block
Ad
l..---,
Ad
L..--,
2jLg/min IjLg/min
i.v
i.v
FIG.6. Release of adrenaline after coronary ligation with suppression after spinal block. Tracings,
calibration and abbreviations as in Fig. 1. Spinal block = injection of 2 ml of 5% lignocaine into
cord at C 1 •
Janina Staszewska-Barczak
428
In a ninth dog the effect of pentolinium was not maintained and after a few minutes release of
adrenaline recommenced. In this dog pentolinium induced a fall in arterial blood pressure to
about 20 mmHg.
In three dogs showing sustained release of noradrenaline at a rate of 2-4 pg/min, the secretion
was also abolished by intravenous pentolinium.
C.R.
RS.S.
_ _ _ B.P.
Ad
~
c
'E
<,
'"
::1..
Ad
~
c
·E
L.,
Pento.
<,
'":I..
~
N
l.v,
i.v.
FIG. 7. Release of adrenaline after coronary ligation with suppression after giving pentolinium.
Tracings, calibration and abbreviations as in Fig. 1. Pento. = injection of pentolinium (2 mg/kg
i.v.),
Chlorisondamine (0'5 mg/kg i.v.) abolished secretion of adrenaline (one dog), of noradrenaline (one dog) and of a mixture of both amines (one dog).
Effect of adrenergic neurone blocking agents
In three dogs given bretylium (5 mg/kg i.v.) I h before, coronary ligation led to an increased
output of adrenaline. In two of these dogs sustained secretion of adrenaline at a maximum
rate of I pg/min was then abolished by pentolinium (Fig. 8).
In five dogs with infarction-induced adrenaline secretion bretylium (5 mg/kg i.v.) did not
decrease the concentration of circulating catecholamine. In three of these dogs the rat stomach
strip, after a transient contraction due to the direct action of bretylium, relaxed even more,
suggesting enhanced noradrenaline release. In none of these experiments did bretylium suppress
or decrease ventricular ectopic activity.
In two dogs given guanethidine (5 rug/kg i.v.) I h before, coronary occlusion induced an
output of adrenaline into the circulation; there were also disturbances of cardiac rhythm. In
another experiment guanethidine was given I h before coronary occlusion and a second
E
Lv.
'it
Lv.
N
Lv.
V
:t.
01
:t.
<,
01
c
'<,E
c:
E
:t.
co
.....
c:
'E
i.v.
LO
E
01
0'
oX
<,
0'
i.v,
N
E
Cl
<,
oX
Lv.
.:!-
<,
0'
C
'E
FIG, 8. Release of adrenaline after coronary ligation in dog pretreated with bretylium and subsequent suppression after pentolinium.
Tracings, calibration and abbreviations as in Fig. 1. Bretyl, = injection ofbretylium (5 mgJkg i.v.), Pento.= injection ofpentolinium
(2 mgJkg i.v.). Relaxation of rat stomach strip after bretylium probably reflects release of noradrenaline. Coronary ligation took
place 1 h after administration of bretylium.
80
120~
~IOO
50m [
R.S.S.
C.R.
s
~
-
~
~
§'
[
~o
~
~'
S'
~
o
is"
~
~
430
Janina Staszewska-Barczak
injection was given after the ligation when there was adrenaline release associated with cardiac
rhythm disorders. This had no effect on either adrenaline release or rhythm disturbances.
Guanethidine was also given to a dog in which, despite consecutive occlusion of the three
branches of the left coronary artery, no increase in catecholamine secretion occurred. The
injection of guanethidine, apart from its usual effect on heart rate and blood pressure with
transient relaxation of assay organs, did not induce any other evident changes.
Effect ofpretreatment with reserpine
Myocardial infarction was produced in nineteen reserpinized dogs in each of which typical
electrocardiographic signs of acute myocardial ischaemia developed. There was an increased
output of adrenaline into the blood stream (1 Jlg/min) during the first hour of occlusion in
only two dogs. The other seventeen dogs failed to secrete detectable amounts of catecholamines, even though in eight of them, one or two other branches of the left coronary artery
were subsequenly tied off. Cardiac rhythm disturbances occurred in only three of the nineteen
dogs. In one of these dogs the development of severe ventricular arrhythmias was associated
with secretion of adrenaline. Transient ventricular arrhythmias were also observed during
intravenous infusions of adrenaline at a rate of 2-4 Jlg/min.
Failure to secrete catecholamines in response to coronary ligation in reserpinized dogs might
result from either severe depletion of catecholamine stores in the adrenal medulla or inhibition
of central adrenergic transmission. Bradykinin stimulates adrenal medullary secretion in the
dog through a direct action on the chromaffin cells (Staszewska-Barczak & Vane, 1967). In
nine of the eleven dogs which failed to secrete catecholamines during the first hour of coronary
occlusion, bradykinin (5 or 10 Jig) was injected through a fine polyethylene catheter into the
aorta just above the origin of the adrenal arteries and regularly induced release of 1-3 Jig of
adrenaline into the blood stream. Similarly, nicotine (50 Jig) injected intra-arterially in two
dogs provoked the release of about 5 Jig of adrenaline. Fig. 9 shows the tracing from a reserpinized dog. There was no release of catecholamines during the first hour of coronary ligation.
However, stimulation of the adrenal medulla by bradykinin (5 Jig) released about 1 Jig of
adrenaline. Acetylcholine (loo Jlg) was much less potent and released only about 0'1 Jlg of
adrenaline. In this dog spontaneous transient outbursts of adrenaline secretion occurred after
intravenous infusions of noradrenaline (2 Jig/min for 5 min). Fig. 10 shows another experiment
in a reserpinized dog. During the second hour after coronary occlusion, which was not
followed by increased secretion of catecholamines, both adrenaline and noradrenaline were
infused in graded doses. The noradrenaline infusion was followed by spontaneous repetitive
bursts of adrenaline secretion into the circulation. This secretion became continuous and then
gradually waned after bilateral vagal section. Intravenous infusions of noradrenaline were
followed by transient or prolonged outpourings of adrenaline in seven of ten reserpinized
dogs.
Three reserpinized dogs and one normal dog which did not liberate catecholamines after
coronary occlusion were given noradrenaline infusions (2 Jlg/min for 5 min) directly into the
unoccluded carotid artery. Similar infusions were also given intravenously. In all three reserpinized dogs intracarotid infusions of noradrenaline were followed by a prolonged release of
adrenaline into the circulation. After intravenous administration of noradrenaline at a similar
rate, this effect was much less pronounced and occurred only in two dogs; a typical experiment
is shown in Fig. II. In the non-reserpinized dog there was no increased adrenaline release into
E
E
x:
01
5
i.v.
Lv.
I.v.
•
0·5p.g
Ad
•
Ip.g
Ad
•t
p.g/min
Ad
~
2
~L...,
::L p.g/min
~
o Ad
.
Ad
I.V.
x
Ach
100JLg
La.
p.g /min
Nor
I.v.
2
L....-,
Lv.
p.g/Ad
2 4
8
~
0·5
B.P.
R.S.S.
C.R.
tv,
FIG.9. Absence of catecholamine release after coronary ligation in dog pretreated with reserpine; adrenaline release after
aortic injection of bradykinin and acetylcholine in the vicinity of the adrenal gland, and after intravenous infusion of
noradrenaIine. Tracings, calibration and abbreviations as in Fig. 1. Bk (two dots) = intra-aortic injection of 5 J.lg of bradykinin. Ach (cross) = intra-aortic injection of 100 J.lg of acetylcholine.
cm[
:
Bk
5JLg
i.a.
~
W
-
.§:
~
§.
§:
~
("')
~c
S·
~
S·
~
S'
C
~
~
g.
Janina Staszewska-Barczak
432
the blood stream after either intracarotid or intravenous infusions of noradrenaline, and
noradrenaline infused by either route produced the expected, dose-dependent relaxation of the
rat stomach strip. In the reserpinized animals, however, there was virtually no relaxation of
this assay tissue when noradrenaline was infused into the unoccluded carotid artery (Fig. 11).
This suggests that all the infused amine was removed from the blood before it reached the
contralateral carotid artery from which the blood was taken for assay.
C.R.
RS.S.
"'IIOf
90
E
E 70
I
B.P
50
•f
I
0'5
~
~
of Ad/min
of Nor/min
}Lg
L.,
Vogot,
}Lg
i.v.
i.v,
FIG. 10. Absence of catecholamine release after coronary ligation in dog pre-treated with reserpine; repetitive discharge of adrenaline after intravenous noradrenaline. Tracings, calibration
and abbreviations as in Fig. 1. Vagct. = bilateral vagotomy.
DISCUSSION
There are several advantages in using the blood-bathed organ technique (Vane, 1964)to study
the mechanisms underlying adrenal medullary activation. The method is sensitive and specific
(Vane, 1958, 1966, 1969)and differentiates between the release of adrenaline and noradrenaline
(Armitage & Vane, 1964). Its dynamic nature makes it well suited to the study of both transitory and prolonged changes in blood catecholamine concentrations.
In a previous study in which this bioassay method was used, we showed that when coronary
occlusion is followed by catecholamine secretion, the response is usually maintained for 2 h
or more (Staszewska-Barczak & Ceremuzynski, 1968). Our present results (summarized in
Table I) show that the sustained secretion of adrenaline induced by infarction could be
abolished by application of lignocaine to the infarcted area of the heart, by spinal block at
C I , by bilateral section of thoracic splanchnic nerves, by ganglionic blockade, and in some
experiments also by bilateral vagotomy. These results indicate that the enhanced adrenal
medullary activity which occurs in the early stage of myocardial infarction is evoked reflexly.
Lignocaine, which acts by preventing the generation and conduction of impulses from sensory
m
cm[
i.v.
Lv.
2P.92p.9
• • •
Ad Nor
2P.9
Lv.
•
Ad
Nor
L.-.-,
5p.9/5min
L cor. o.
Nor
L.-.-,
5p.9 /5min
i.v.
0'5P.~
Ad
R.S.S.
. B.P.
lp.g/4min
Lv.
FIG.11. Absence of catecholamine release after coronary ligation in dog pretreated with reserpine; adrenaline release after infusion
of noradrenaline into carotid artery with much smaller release after infusion intravenously. Tracings, calibration and abbreviations as in Fig. 1. Note absence of relaxation of rat stomach strip during intracarotid infusion of noradrenaline and failure of
intravenous adrenaline to induce spontaneous secretion of catecholamines.
E 60
tOO~
E 80
5
C.R.
W
W
~
~
§.
~
~
§:
~
g
~
S·
~.
~
is"
~
~
g.
~
1
2
3
5
Neurone blocking agents
Bretylium
Before infarction
During infarction
Guanethidine
Before infarction
During infarction
9
2
0
0
0
0
8
2
3
3
Ganglion-blocking agents
Pentolinium
Chlorisondamine
4
4
Spinal block
Thoracic splanchnic
nerves section
6
9
7
No. of Abolished
dogs
0
0
0
0
0
1
0
1
2
3
5
0
0
0
0
0
4
0
No change
5
I
Decreased
Adrenaline secretion
18
Bilateral vagotomy
Lignocaine topically on
infarcted myocardium
Procedure
3
2
0
0
0
-
0
-
3
1
2
-
0
0
1
-
6
0
0
6
0
0
2
2
No change
Decreased
Abolished
No. of
dogs
Noradrenaline secretion
TABLE 1. Effects of various surgical procedures and blocking agents on sustained catecholamine secretion induced by acute
coronary occlusion
~
~
~
~
.,~
l::l
I
~
~
~
~
S
c.,
V:l
l::l
~
;:s
S·
~
Yo)
Catecholamines in myocardial infarction
435
nerve endings (Strobel & Wollman, 1969), abolished the adrenaline secretion when applied
topically to the ischaemic myocardium, and this indicates that the reflex originates in cardiac
receptors at the site of, or near to, the infarct.
The extrinsic innervation of the heart comes from the vagus and cardiac sympathetic nerves
(Woollard, 1926; Nettleship, 1936; Hirsch, Nigh, Kaye & Cooper, 1964; Abraham, 1969). In
our experiments bilateral vagotomy suppressed infarction-induced adrenaline secretion in 50%
of the dogs, decreased it to about one-half in a further 28% and had no effect on adrenaline
liberation in the remaining 22%. These results suggest that the afferent arm of the reflex arc
from the heart to the adrenals may take either a vagal, or an extra-vagal path via cardiac
sympathetic nerves, or both these pathways.
The suppression of adrenaline secretion after spinal block at C 1 indicates that the pathway
for the reflex discharge of adrenal medullary hormones in the early stages of myocardial
infarction is confined to supraspinal structures, most probably in the hypothalamus and brainstem reticular formation. Liberation of catecholamines from the adrenal medulla on stimulation of the hypothalamus (Houssay & Molinelli, 1925b; Briicke, Kaindl & Mayer, 1952;
Redgate & Gellhorn, 1953; Folkow & Euler, 1954) and brain-stem reticular formation
(Marley, 1960) has been repeatedly demonstrated in dogs and cats. Liberation of adrenal
catecholamines by stimulation of brain-stem reticular formation could not be demonstrated
after section of the spinal cord at C 1 and was virtually abolished by splanchnic nerves section
if the spinal cord was intact (Marley, 1960). In the present study transection of both thoracic
splanchnic nerves, the major neural supply to the adrenal glands (Mizeres, 1955), also abolished
infarction-induced adrenaline secretion showing that the adrenaline release was evoked entirely
by nervous impulses conducted along the splanchnic nerves.
Unlike ganglion-blocking agents the adrenergic neurone-blocking agents were effective
neither in prevention nor in suppression of adrenaline secretion after coronary occlusion.
This is understandable because neither bretylium (Boura & Green, 1959) nor guanethidine
(Page & Dustan, 1959) inhibit stimulation of the adrenal medulla by the splanchnic nerves or
by injection of dimethylphenylpiperazinum iodide. Bretylium but not guanethidine prevents
and abolishes various types of experimental and clinical ventricular arrhythmias, including
those due to myocardial infarction (Bacaner, 1968a, b). Our results do not confirm these
observations, but are consistent with those reported by Allen, Shanks & Zaidi (1969) which
showed potentiation of the arrhythmogenic effect of adrenaline during the first hour after
bretylium administration.
In seventeen out of nineteen reserpinized dogs, coronary ligation failed to induce secretion
of catecholamines. These results are in striking contrast with those in unreserpinized dogs, in
which 66% secrete catecholamines after acute coronary occlusion (Staszewska-Barczak &
Ceremuzynski, 1968; Ceremuzynski, Staszewska-Barczak & Herbaczynska-Cedro, 1969). This
failure of reserpinized dogs to liberate adrenaline could not be attributed to depletion of
catecholamine stores in the adrenal medulla, since stimulation of the adrenal glands with
bradykinin, acetylcholine or nicotine regularly resulted in a transient output of adrenaline into
the blood stream.
Although the reflex control mechanisms for the adrenal medulla are still not fully understood, it is believed that the hypothalamus and reticular formation play an important role in
the regulation of its function. Reserpine produces severe and long lasting depletion of noradrenaline stores in the hypothalamus (Holzbauer & Vogt, 1956) which suggests that impair-
436
Janina Staszewska-Barczak
ment of central adrenergic transmission is due to transmitter deficiency. However, both a
decrease (Bein, 1955, 1957)and an increase (Iggo & Vogt, 1960)in central sympathetic outflow
have been reported in reserpinized animals. Our results suggest that the failure of reserpinized
dogs to secrete adrenaline in response to myocardial infarction was mainly due to a failure of
central adrenergic transmission resulting from noradrenaline deficiency. The hypothalamus is
the only part of the brain that takes up a significant amount of catecholamines from the
circulation (Weil-Malherbe, Axelrod & Tomchick, 1959; Weil-Malherbe, 1960). Administration of noradrenaline to reserpinized animals at a time when brain catecholamine concentrations are severely depressed leads to rapid recovery of brain noradrenaline stores (Glowinski,
Iversen & Axelrod, 1966). It thus appears probable that the restoration of adrenal medullary
secretion observed after noradrenaline administration in reserpinized dogs with coronary
occlusion was due to the temporary restoration of central adrenergic transmission for the
reflexes arising from receptors at the site of infarction.
Infarction-induced secretion of adrenaline comes from the adrenal medulla, as shown by its
cessation after bilateral adrenalectomy (Staszewska-Barczak & Ceremuzynski, 1968) and, as
is confirmed in the present study, by its abolition after bilateral transection of splanchnic
nerves. The noradrenaline, however, may be released from several sources. StaszewskaBarczak & Ceremuzynski (1968) described a single experiment in which noradrenaline
secretion was abolished by bilateral adrenalectomy. The heart releases relatively large amounts
of noradrenaline with appropriate stimulation (Richardson & Woods, 1959) and after acute
coronary occlusion (Lammerant, De Herdt & De Schryver, 1966). Myocardial stores may thus
be an important source for infarction-induced secretion of noradrenaline into the circulation.
It has also been suggested that the elevated plasma noradrenaline concentrations found 24 h
after coronary occlusion in dogs were derived from postganglionic sympathetic nerves
(Richardson, 1963).
Enhanced liberation of noradrenaline, either alone or in a mixture with adrenaline, was
detected in fourteen dogs in the present study (Table 1). Bilateral adrenalectomy (three dogs)
and transection of thoracic splanchnic nerves (one dog) failed to abolish noradrenaline
secretion which indicates that the amine did not come from the adrenal medulla. We cannot
say whether the noradrenaline was released from the heart or from other stores in the body.
If it came from the heart, its appearance could not simply be due to local damage and subsequent leakage of the transmitter, since the release was abolished by local application of
lignocaine and by intravenous ganglion-blocking agents.
Malliani, Schwartz & Zanchetti (1969) showed that T 3 sympathetic fibres, which probably
contribute to the efferent innervation of the heart, are frequently activated when myocardial
ischaemia is induced by coronary occlusion. The most frequent reflex response to coronary
occlusion consisted of an increase in firing rate. This increased sympathetic discharge was
independent of sinoaortic reflexes, for it occurred also in spinal animals. These results, together
with those of Brown (1967) showing increased discharge in sympathetic afferent fibres at the
time of coronary occlusion, suggest that in some of our experiments at least enhanced noradrenaline release could arise from cardiac postganglionic sympathetic nerve terminals, activated through a cardio-cardiac reflex at a spinal level. This would also explain why bilateral
vagotomy was ineffective in abolishing infarction-induced noradrenaline secretion.
In conclusion, our results point to the essential role of nervous reflexes arising from the site
and the boundary of the infarct in eliciting enhanced liberation of catecholamines during the
Catecholamines in myocardial infarction
437
early stage of myocardial infarction. In later stages of infarction other factors, such as circulatory disturbances due to cardiac insufficiency and the release of humoral and chemical agents
from the necrotic myocardium or poorly perfused peripheral organs, might also participate,
or even predominate, in the induction and maintenance of increased sympatheticoadrenal
activity.
ACKNOWLEDG MENTS
I wish to express my gratitude to Professor John R. Vane for his continuous support and
encouragement during this work, as well as for his valuable help in preparing the manuscript.
I also wish to thank Miss Kinga Sroczynska for her excellent technical assistance.
REFERENCES
ABRAHAM, A. (1969) Microscopic Innervation of the Heart and Blood Vessels in Vertebrates including Man,
pp. 160-161. Akademiai Kiad6, Budapest.
ALLEN, J.D., SHANKS, R.G. & ZAIDI, S.A. (1969) A comparison of the effects of bretylium, lignocaine and
propranolol on experimental cardiac arrhythmias. British Journal ofPharmacology, 37, 526p-527p.
ARMrrAGE, A.K. & VANE, J.R. (1964) A sensitive method for the assay of catecholamines. British Journal of
Pharmacology, 22, 204--210.
BACANER, M.B. (1968a) Quantitative comparison of bretylium with other antifibrillatory drugs. American
Journal of Cardiology, 21, 504--512.
BACANER, M.B. (1968b) Treatment of ventricular fibrillation and other acute arrhythmias with bretylium
tosylate. American Journal of Cardiology, 21, 530-543.
BEIN, RJ. (1955) Significance of selected central mechanisms for the analysis of the action of reserpine. Annals
of the New York Academy of Sciences, 61, 4-16.
BEIN, RJ. (1957) Effects of reserpine on the functional strata of the nervous system. Psychotropic Drugs, pp.
325-331. Ed. by Garattini, S. and Ghetti, W. Elsevier, Amsterdam.
BoURA, A.L.A. & GREEN, A.F. (1959) The actions of bretylium; adrenergic neurone blocking and other effects.
British Journal ofPharmacology, 14, 536-548.
BROWN, A.M. (1967) Excitation of afferent cardiac sympathetic nerve fibers during myocardial ischaemia.
Journal of Physiology, 190, 35-53.
BRUCKE, F.V., KAiNDL, F. & MAYER, H. (1952) Uber die Verlinderung in der Zusammensetzung des
Nebennierenmarkinkretes bei elektrischer Reizung des Hypothalamus. Archives lntemationales de Pharmacodynamie et de TMrapie, 88, 407-412.
CEREMUZYNSKI, L., STASZEWSKA-BARCZAK, J. & HERBACZYNSKA-CEDRO, K. (1969) Cardiac rhythm disturbances
and the release of catecholamines after acute coronary occlusion in dogs. Cardiovascular Research, 3,
190-197.
EULER, U.S. & FOLKOW, B. (1953) Einftus verschiedener afferenter Nervenreize auf die Zusammensetzung des
Nebennierenmarkinkretes bei der Katze. Archi» fiir experimentelle Pathologie und Pharmakologie, 219,
242-247.
FOLKOW, B. & EULER, U.S. (1954) selective activation of noradrenaline and adrenaline producing cells in the
eat's adrenal gland by hypothalamic stimulation. Circulation Research, 2, 191-195.
GLOWINSKI, J., IVERSEN, L.L. & AxELROD, J. (1966) Storage and synthesis of norepinephrine in the reserpinetreated rat brain. Journal of Pharmacology and Experimental Therapeutics, 151, 385-399.
HAYASHI, K.D., Moss, A.J. & Yu, P.N. (1969) Urinary catecholamine excretion in myocardial infarction.
Circulation, 40, 473-481.
HIRSCH, E.F., NIGH, C.A., KAYE, M.P. & CooPER, T. (1964) Terminal innervation of the heart. Archives of
Pathology, 77, 86-187.
HODGE, R.L., LOWE, R.D. & VANE, J.R. (1966) The effects of alteration of blood-volume on the concentration
of circulating angiotensin in anaesthetized dogs. Journal ofPhysiology, 185, 613-626.
438
Janina Staszewska-Barczak
HODGE, R.L., LoWE, R.D. & VANE, J.R. (1969) The role of circulating catecholamines in arterial baroceptor
reflexes in the dog and in man. Clinical Science, 37, 69-77.
HOLZBAUER, M. & VOOT, M. (1956) Depression by reserpine of the noradrenaline concentration in the hypothalamus of the cat. Journal of Neurochemistry, 1, 8-11.
HOUSSAY, B.A. & MOLINELLI, E.A. (1925a) secretion reflexe d'adrenaline. Comptes Rendus de la Societe de
Biologie, 93, 881-883.
HOUSSAY, B.A. & MOLINELLI, E.A. (1925b) Centre adrenalino-secreteur hypothalamique. Comptes Rendus de
la Societe de Biologie, 93, 1454-1455.
IGGO, A. & VOOT, M. (1960) Preganglionic sympathetic activity in normal and in reserpine-treated cats. Journal
of Physiology, 150, 114-133.
JEWITT, D.E., MERCER, C.J., REID, D., VALORI, C., THOMAS, M. & SHILLINGFORD, J.P. (1969) Free noradrenaline
and adrenaline excretion in relation to the development of cardiac arrhythmias and heart failure in patients
with acute myocardial infarction. Lancet, i, 635-641.
KAINDL, F. & EULER, U.S. (1951) Liberation of noradrenaline and adrenaline from the suprarenals of the cat
during carotid occlusion. American Journal 0/ Physiology, 166, 284-288.
KOLATAT, T., ASCANIO, G., TALLARIDA, R.J. & OPPENHEIMER, M.J. (1967) Action potentials in the sensory
vagus at the time of coronary infarction. American Journal of Physiology, 213, 71-78.
LAMMERANT, J., DE HERDT, P. & DE SCHRYVER, C. (1966) Direct release of myocardial catecholamines into
the left heart chambers: the enhancing effect of acute coronary occlusion. Archives internationales de
Pharmacodynamie et de Therapie, 163, 219-226.
MALLIANI, A., SCHWARTZ, P.J. & ZANCHETTI, A. (1969) Reflex activity of single preganglionic sympathetic
fibers during coronary occlusion. Experientia, 25, 152-153.
MANN, M. & WEST, G.B. (1950) The nature of hepatic and splenic sympathin. British Journal ofPharmacology,
5,173-177.
MARLEY, E. (1960) Release of adrenaline substance by electrical stimulation of the brain stem. Adrenergic
Mechanisms, pp, 424-427. CIBA, Churchill, London.
MIZERES, N.J. (1955) The anatomy of the autonomic nervous system in the dog. American Journal of Anatomy,
96, 285-318.
NETTLESHIP, W.A. (1936) Experimental studies on the afferent innervation of the eat's heart. Journal of Comparative Neurology, 64, 115-131.
PAGE, I.H. & DUSTAN, H.P. (1959) A new, potent antihypertensive drug. Preliminary study of [2-(octahydro-lazocinylj-ethyll-guanidine sulphate (guanethidine). Journal of the American Medical Association, 170, 12651271.
REDGATE, E.S. & GELLHORN, E. (1953) Nature of sympathetico-adrenal discharge under conditions of excitation
of central autonomic structures. American Journal of Physiology, 174, 475--480.
RICHARDSON, J.A. (1963) Plasma catecholamine concentration in acute infarction. Coronary Heart Diseases,
pp. 273-277. Ed. by Likoff, W. and Moyer, J.H. Grune & Stratton, New York.
RICHARDSON, J.A. & WOODS, E.F. (1959) Release of norepinephrine from the isolated heart. Proceedings of the
Society for Experimental Biology and Medicine, 100, 149-151.
SENDERROFF, E., WARNER, R.R.P. & BARONOFSKY, J.D. (1962) Blood serotonin levels in dogs with acute
myocardial infarction produced by coronary ligation. Journal of Thoracic and Cardiovascular Surgery, 44,
78-83.
SOFIEVA, I.E. (1965) Excretion of catecholarnines in urine of patients with myocardial infarction. Terapevteecheskij Arkhiv, 37, 81-87 [in Russian],
STASZEWSKA-BARCZAK, J. & CEREMUZYNSKI, L. (1968) The continuous estimation of catecholamine release in
the early stages of myocardial infarction in the dog. Clinical Science, 34, 531-539.
STASZEWSKA-BARCZAK, J. & VANE, J.R. (1967) The release of catecholamines from the adrenal medulla by
peptides. British Journal ofPharmacology, 30, 655-667.
STROBEL, G.E. & WOLLMAN, H. (1969) Pharmacology of anesthetic agents. Federation Proceedings. Federation
of the American Societies for Experimental Biology, 28, 1386-1403.
VANE, J.R. (1957) A sensitive method for the assay of 5-hydroxy-tryptamine. British Journal of Pharmacology,
12,344-349.
VANE, J.R. (1958) The blood-bathed isolated organ: a method of testing the circulating blood for active substances. Journal ofPhysiology, 143, 75p-76p.
Catecholamines in myocardial infarction
439
VANE, J.R. (1964) The use of isolated organs for detecting active substances in circulating blood. British Journal
ofPharmacology, 23, 360-373.
VANE, J.R. (1966) The estimation of catecholamines by biological assay. Pharmacological Reviews, 18, 317-324.
VANE, J.R. (1969) The release and fate of vaso-active hormones in the circulation. British Journal of Pharmacology, 35, 209-242.
WEIL-MALHJlRBE, H. (1960) The passage of catecholamines through the blood-brain barrier. Adrenergic
Mechanisms, pp. 421-423. ClBA, Churchill, London.
WJlIL-MALHJlRBE, H., AxELROD, J. & TOMCHICK, R. (1959) Blood-brain barrier for adrenaline. Science, 129,
1226-1227.
WOOLLARD, H.H. (1926) The innervation of the heart. Journal of Anatomy, 60, 345-373.