Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
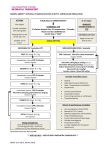
ACLS Review Jack Hornick 7/28/15 Announced overhead… DR Heart First floor Atrium … DR Heart First floor Atrium Who goes to the code • Interns, senior residents, AIs, and 3rd year medical students on Long Call on wards and in MICU • DACR/VACR/NACR • Anesthesia team • Respiratory Therapists • Critical care nurses (from MICU/CICU) • Critical care pharmacist (sometimes) Who runs the code? • First resident on the scene, or DACR/VACR/NACR • The leader of the code assigns roles and responsibilities to the other residents and interns available Roles during the code • • • • • • • • Stabilizing/managing airway Line for chest compressions Recording timing of events Managing code cart/ Medication administration Checking labs and past medical history, telemetry Obtaining emergency access Thinking through Hs and Ts Calling the patient’s family Code Blue You are the Naff intern on call, working on notes in the Naff team room. Code Blue is called for a patient on Lakeside 20. Your senior is MIA. You run down the hall and are the first on the scene. What do you do? Scenario 1 • You feel a thready femoral pulse, the patient feels tachycardic • Automatic blood pressure cuff is not reading • Patient is agonal breathing, not responding to verbal or painful stimuli • The nurses look to you and say “Doctor, what do we do?” • On arrival, you do a quick initial assessment while assessing his responsiveness and vital signs and immediately instruct someone to begin compressions. • While compressions are occurring you ask the nurse to apply pads and electrodes to the patient to analyze the rhythm. • In addition, you ask that oxygen be applied to the patient • You ask about any complaints the patient may have had and find that minutes ago he was complaining of chest pain, palpitations, and dizziness. • Being a very keen intern, you recognize this may be Acute Coronary Syndrome causing arrest. Cardiac Arrest, 4 rhythms • As you pause during compressions you analyze the rhythm… the patient is in Ventricular Fibrillation • The DACR runs into the room, you notify him/her of the patient’s rhythm and • ANALYZE.. CLEAR…SHOCK DELIVERED • Resume CPR! Wait to reanalyze the rhythm after the next round of CPR • The patient receives a dose of Epinephrine in addition to another shock and has conversion to sinus rhythm. He has ROSC. His vitals begin to improve and he is rushed to the Cardiac Catherization Lab. • Nice Work! High quality CPR is key • Rate approx 100/min • Compression depth >2 inches (5cm) in adults • Allow complete chest recoil after each compression • Minimize interruptions • Rotate every 2 minutes Scenario 2 • One of your many pagers on Intern Nightfloat goes off. • “There’s a Code White on your patient in Lakeside 55 her heart rate is a little low and she’s feeling dizzy” • You ask the nurse to get a full set of vitals as you head towards the patient’s room. • As you’re headed over you hear the overhead announcement “CODE BLUE, CODE BLUE, CODE BLUE..LAKESIDE 55” • You arrive at the patient’s room and the nurse informs you that the patient’s HR was 60-70’s during the day but suddenly decreased from 48 to 35bpm. • Current vitals: HR 35bpm, SBP 70/DBP is undetectable RR 16/min, and O2 saturation 93%. • The patient was initially complaining of lightheadedness but now is more lethargic. • You take a look at the EKG that was obtained. • You request oxygen be applied to the patient and the pads for transcutaneous pacing be applied. • Just as you are doing so, additional help arrives and your Nightfloat senior assists you. • Atropine is obtained from the crashcart and the patient is bolused 0.5mg. • The patient’s HR slightly improves to 49bpm but he remains somewhat confused and lethargic. • Transcutaneous pacing is started with a target HR of 60bpm. She begins to wake up and her BP improves to 110/57. • EP is consulted and the patient receives a transvenous and ultimately an implanted pacemaker. Last Scenario • You are on Hellerstein waiting to sign out at 630 pm on a Sunday when you’re paged about a patient with past hx of SVT here for CP now has a HR of 160. • BP 125/80, narrow complex tachycardia as below • After attempting vagal maneuvers (unsuccessful) you give adenosine 6mg IV push, and then 12 mg IV push • Now the patient develops severe chest pain, He 220, BP not obtainable, pulse weak. The patient begins losing consciousness. What do you do next? • Synchronized cardioversion is unsuccessful. Patient now is pulseless and unconscious. What next? Time to shock! (unsynchronized 120-200 J) Synchronized vs unsynchronized cardioversion Synchronized Low energy shock delivers shock w/ peak of QRS Indications: unstable A fib, A flutter, SVT If shock occurs on t-wave, high likelihood of VF Unsynchronized High energy shock delivers as soon as shock button is pushed Indications: pulseless VT/VF • After 5 cycles of CPR, the rhythm check suggests a second shock. Now with 200 J. Which medications should you be giving? • Epinephrine 1mg IV q3min and/or vasopressin 40 U IV to replace first or second epi dose • Amiodarone after 3rd shock in pulseless VT (300 mg IV x1, then consider 150 mg IV x1 • SROC! The patient was intubated by anesthesia at the scene, and is not responding to verbal commands. Patient transported to CICU. What post cardiac arrest intervention would this patient benefit from? What Is ACLS? • ACLS guidelines first published 1974 by AHA, most recent update 2010 • A series of interventions for urgent treatment of cardiac arrest, stroke, and life threatening medical emergencies • Several algorithms for VF/Pulseless VT, Bradycardia, Suspected Stroke • An essential part of using the algorithm correctly is to search for and correct potentially reversible causes of arrest • Performing high quality CPR, identifying arrhythmias and understanding the pharmacology behind key drugs are central to ACLS. H’s and T’s Treatable causes of cardiac arrest • • • • • • Hypoxia Hypovolemia Hydrogen ion (acidosis) Hypokalemia Hyperkalemia Hypothermia • Thrombosis (pulmonary) • Thrombosis (coronary) • Tamponade • Tension pneumothorax • Toxins Things to discuss with patients • All patients admitted to the hospital should be asked about their code status • It’s important to discuss the morbidity associated with ACLS • Statistics regarding survival after arrest • Adverse outcomes of CPR and Advanced Airway Support Don’t forget to pick up your ACLS cards from the chiefs office! Remember to check your own pulse first.