Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
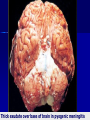
Pathology of Nervous System (I) -3 2016 Dr. Mohammed Alorjani, MD. EBP. INFECTIONS OF CNS IMPORTANT FACTORS Route: Hematogenous (most common), Direct (trauma & iatrogenic…), Local extension from adjacent focus, e.g. air sinuses & congenital malformations, Peripheral nerves Agent: Bacteria, Viruses, Fungi, Parasites, or immune process Normal or immunocompromised host SITES of INFECTIONS Epidural & Subdural infections Meningitis Cerebral abscess Encephalitis, mainly viral Epidural & Subdural Infections: Staph., Strep., Gram neg. bacilli, Mixed. Direct local spread Epidural Localized space occupying lesion Subdural empyema Spreading infection & ↑ICP Involvement of subdural vessels may lead to cerebral cortical thrombophlebitis and arteritis infarction Meningitis: Inflammation of leptomeninges & CSF 1- Acute Bacterial Meningitis: - Neonates: Group B Streptococci & E. coli 6M: H. influenza, S. pneumoniae Adolescents & young adults: N. meningitidis Elderly: S. pneumoniae & L.monocytogenes Shunt operations: Staphylococci Clinical picture: Fever, headache, vomiting, photophobia, neck rigidity. In N. meningitidis, may be accompanied by skin rash & complicated by septicemic shock Waterhouse Friderichsen Syndrome C.S.F. findings: ↑Pressure, ↑Protein, ↓sugar, numerous neutrophils, demonstrable bacteria Morphology: Exudate in subarachnoid space, especially around base, full of neutrophils & organisms Severely congested meningeal vessels, surrounded by neutrophils Sometimes superficial cerebritis & ventriculitis Abscesses may occur May show phlebitis, venous occlusion & hemorrhagic infarction of underlying brain. PURULENT (BACTERIAL) MENINGITIS Thick exudate over base of brain in pyogenic meningitis PURULENT MENINGITIS 2- Acute Aseptic Meningitis (Viral Meningitis): Enterovirus, echovirus, coxackie & mumps v. EBV, HIV Hematogenous spread Mild self-limiting often seasonal Brain edema, mild mononuclear cell infiltration of meninges & superficial brain cortex CSF is clear, slight protein, normal sugar, lymphocytes ASEPTIC (VIRAL) MENINGITIS 3. CHRONIC Meningitis/meningoencephalits TB, brain and meninges SYPHILIS, gummas in brain LYME DISEASE (Neuro-borreliosis) transmitted by ticks. – aseptic meningitis – facial nerve palsies – polyneuropathies – mild encephalopathy. Chronic Meningitis: 1- Tuberculous Meningitis: Hematogenous spread from lung → brain Direct spread from Tuberculous vertebra Result: meningitis or tuberculoma Morphology: Thick cheesy exudate, thick meninges, tubercles on surface. ( Caseating Granulomas) Basal cisterns & sulci most affected May show obliterative endarteritis & infarction CSF: Protein, lymphocytes, sugar N or TUBERCULOMA 2- Neurosyphilis: caused by spirochete (T. pallidum) Meningovascular syphilis: Meningeal chronic infection with obliterative endarteritis & cerebral gummas. – usually base of brain Plasma cells characteristically in lesions Paretic neurosyphilis: Invasion of frontal lobe by spirochetes, loss of neurons & proliferation of microglia (ROD CELLS) & gliosis ± granular ependymitis Result: progressive mental deficits, mood alteration → severe dementia – General Paresis of the Insane (GPI) Tabes Dorsalis: Involves spinal cord → damage to sensory nerves in dorsal columns: loss of pain sensation and joint position sense & locomotor ataxia → skin and joint damage (Charcot joints), characteristic "lightning pains” & absence of deep tendon reflexes Acute syphilitic meningitis: HIV infected patients who have ↑risk for neurosyphilis & may develop severe rapidly progressive disease Complications of Bacterial Meningitis 1- Obstructive hydrocephalus 2- Cerebral infarction 3- Cerebral abscess 4- Epilepsy 5- Cranial nerve palsy 6- Deafness ** Prognosis depends on rapidity of proper antibiotic therapy Parenchymal Infections: Localized: abscess, tuberculoma, toxoplasmosis, parasites Diffuse: encephalitis, usually viral Brain Abscess: – Usually bacterial but may be fungal – Direct implantation – Local extension: from paranasal sinusitis, mastoiditis & middle ear infection Frontal or temporal lobes – Hematogenous route: usually with predisposing conditions... May be multiple – Morphology: Localized suppuration & liquefactive necrosis, surrounded by granulation tissue, reactive astrocytes & severe edema leading to ICP. Later Fibrous capsule & gliosis – CSF: protein, cells, normal sugar – Complications: Meningitis, Venous sinus thrombosis, Ventriculitis, Focal neurological defects, epilepsy. PURULENT CEREBRAL ABSCESS VIRAL Encephalitis ARBO VIRUSES (West Nile, Equines,… etc) HSV1 & HSV2 Herpes Zoster CMV POLIO RABIES HIV Progressive Multifocal Leukoencephalopathy (JC) Subacute Sclerosing Panencephalitis (Measles) May be sporadic in healthy subjects May only affect immunocompromised subjects Some are selective to the CNS while others affect other tissues VIRAL ENCEPHALITIS & MYELITIS: Sporadic infection: HSV encephalitis Latent infections: Herpes Zoster Neurotropic: Poliovirus, Rabies Antenatal: CMV, Rubella Immune deficiency: HIV, CMV, PML, Herpes Zoster Some systemic viral infections do not infect the CNS, but initiate immune mechanisms in CNS e.g. Influenza virus Some viruses have selective sites: – – – – CMV -Ventricles HSV -Temporal lobe & orbital frontal area Polio - Anterior horn cells of spinal cord Herpes Zoster - Thoracic dorsal root ganglia Features common to most viral infections: 1- Perivascular mononuclear infiltrate 2- Cell lysis, neuronophagia 3- Microglial nodules 4- Nuclear or cytoplasmic inclusions e.g. Cytoplasmic negri bodies in rabies, nuclear inclusions in CMV …etc. Microglia showing neuronophagia Perivascular cuffs of lymphocytes Microglial nodules RABIES CMV 1- Herpes Simplex Virus type 1 & 2 Normal host: children or adults Hemorrhagic necrotizing inflammation in temporal lobe & orbital gyri of frontal lobe HSV-2 in adults may cause meningitis All common features of viral encephalitis seen with eosinophilic intranuclear viral inclusions (Cowdry type A) in neurons & glial cells. HERPES ENCEPHALITIS 2- Varicella –Zoster Virus (Herpes-Zoster) Chicken pox in children but latent infection in dorsal root ganglia in adults Self-limited skin eruption along a dorsal nerve dermatome (Shingles) or Postherpetic Neuralgia In immunosuppressed patients, may show acute encephalitis. Lesion is typical of viral infection ± granulomatous arteritis & infarction 3- Cytomegalovirus (CMV) AIDS patients: subacute encephalitis any region & any cell but mainly ependymal & subependymal cells. There is hemorrhagic periventricular necrosis with large cytoplasmic & intranuclear inclusions Fetus: intrauterine infection. Changes similar to above + brain destruction, microcephaly & calcification 4- Rabies Severe often fatal, encephalitis – bite of a canine or others – ascending along peripheral nerve from bite, incubation period may last months Neuronal degeneration and inflammatory reaction, most severe in midbrain, & floor of 4th. Ventricle Presence of Negri bodies: cytoplasmic, eosinophilic inclusions in pyramidal neurons of the hippocampus & Purkinje cells of cerebellum 5- Poliovirus Enterovirus causing mild gastroenteritis Involvement of CNS in the non-immunised Acute: mononuclear cell perivascular cuffs and neuronophagia of the anterior horn motor neurons of the spinal cord Chronic: Atrophy of the anterior (motor) spinal roots, and neurogenic atrophy of denervated muscle. Postpolio syndrome Rare cases develop paralysis of respiratory muscles 6- Human Immunodeficiency Virus (HIV) At least 60% of AIDS pts. develop CNS dis. Early: aseptic viral meningitis in 10% Chronic HIV: Meningoencephalitis: Progressive → HIV encephalopathy, affecting motor control, memory, incontinence Commonest cause of dementia in the young (HAND) Demyelination: Vacuolar myelopathy affecting spinal cord nerve tracts. Pathology: – Mainly white matter & basal ganglia, & spinal cord. – Demyelination, microglial nodules with multinucleated giant cells … – Brain atrophy 7- JC virus →PML (Progressive Multifocal Leukoencephalopathy) Caused by JC virus (a polyomavirus) exposure during childhood AIDS patients & other immunosuppressed patients Infect oligodendrocytes: Enlarged nuclei with inclusions. Large astrocytes are also seen. RESULT: Progressive demyelination of white matter PRION DISEASES SPONGIFORM ENCEPHALOPATHIES: Caused by prion variants not containing RNA nor DNA TRANSMISSIBLE FATAL Disease, NO Rx Prion proteins are present in normal brains ( PrP) Abnormal folding (mutation) of PrP → (PrPsc ) → (PrPsc, PrPsc, PrPsc …etc) Mutation can be sporadic, familial or iatrogenic acquired via infected material Include a variety of conditions: * * * * * * Kuru Creutzfeldt-Jacob Disease ‘New Variant’ CJD Fatal Familial Insomnia Scrapie in sheep Bovine spongiform encephalopathy (Mad Cow Disease) CJD (Creutzfeldt-Jakob) 1 per million incidence, 7th decade Sporadic cases, not epidemic Iatrogenic Transmitted ! Contaminated material Familial cases well documented – PRNP mutation (15%) Rapidly progressive dementia FATAL, no treatment known, like ALL prion diseases Creutzfeldt-Jacob Disease: – Rapidly progressive – Usually older people – Younger in familial cases Variant CJD = Mad Cow Disease – usually acquired through cattle & recently, blood transfusion. Pathology: Multifocal spongiform transformation of cortex & deep grey matter→ multiple cysts, most in caudate & putamen. No inflammatory response. Microscopic findings: – Neuronal loss – Gliosis – Atrophy – Amyloid deposits may be present (v.CJD) FUNGAL ENCEPHALITIS: Candida, Cryptoccocus, Aspergillus, & Mucor Normal or Immunocompromised patient sp. Cryptoccocus Hematogenous or direct spread Diabetics with ketoacidosis are especially prone to Mucormycotic infection from nose or sinuses AIDS patients are prone to cryptococcal meningoencephalitis Blood vessel invasion with hemorrhagic infarction especially found in Aspergillus Morphology of fungal infections: Microabscesses in brain or poorly formed granulomas ± meningitis. Fungi can be demonstrated by PAS or Silver stain OPPORTUNISTIC INFECTIONS Fungal cerebritis: Aspergillus OPPORTUNISTIC INFECTIONS Fungal cerebritis: Aspergillus Other infections: Cerebral Toxoplasmosis: occurs in immuno-compromised patients (AIDS), produces small, usually multiple, abscesses & necrotic foci which contain toxoplasma pseudocysts in microglial nodules Toxoplasma Pseudocyst Amebic meningoencephalitis Cysticercosis: Tapeworm Tenia Solium – Man is the intermediate host: Ova are ingested Larvae Cysts – Anywhere in the body ! – Mass lesion – Death intense inflammation & eosinophils Echinococcosis: Echinococcus granulosus Tapeworm Hydatid Cyst Hydatid Cyst Wall