Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
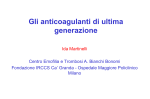
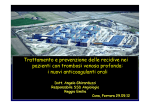
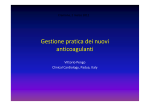
Simposio: Nuovi anticoagulanti orali: dai criteri di scelta all’esperienza sul campo Dabigatran Paolo Verdecchia, F.A.C.C., F.E.S.C., F.A.H.A. Hospital of Assisi Department of Medicine Via Valentin Müller, 1 06081 - Assisi PG E-mail: [email protected] Conflict of Interest Disclosure Travel grants/fee for membership on Advisory Committees and speaking at scientific meetings: • Boehringer-Inghelheim • Bayer • Daiichi-Sankyo • Stroder No honorarium for today’s talk Dabigatran 1. Lo studio RE-LY 2. Le indagini della Food and Drug Administration (FDA) 3. L’esperienza di Assisi Dabigatran 1. Lo studio RE-LY 2. Le indagini della Food and Drug Administration (FDA) 3. L’esperienza di Assisi Parametro RELY ROCKET-AF ARISTOTLE ENGAGE-AF N = 18 113 N = 14 264 N = 18 201 N = 21 105 Disegno dello studio: Multicentrico (951 centri), randomizzato, warfarin in aperto, dabigatran in doppia cecità (PROBE) Multicentrico (1178 centri), randomizzato, doppia cecità, double dummy Multicentrico (1030 centri), randomizzato, doppia cecità, double dummy Multicentrico (1393 centri), randomizzato, doppia cecità, double dummy Dose Dabigatran: 110 mg b.i.d.; 150 mg b.i.d. Rivaroxaban: 20 mg o.d. (15 mg o.d. se VFG 3049 cc/min) Apixaban: 5 mg b.i.d. (2.5 mg o.d. se età > 80, peso <60 o creatininemia > 1.5 mg/dl) Edoxaban: 60 mg od; 30 mg od. Dosi dimezzate se: VFG 30-50; peso <60, verapamil e/o chinidina Endpoint primario Composito di ictus (ischemico / emorragico) ed embolia sistemica Composito di ictus (ischemico / emorragico) ed embolia sistemica Composito di ictus (ischemico ed emorragico) ed embolia sistemica Composito di ictus (ischemico ed emorragico) ed embolia sistemica Durata follow-up 2.0 anni (mediana) 1.8 anni (mediana) 1.9 anni (mediana) 2.8 anni (mediana) Endpoint primario di sicurezza Sanguinamenti maggiori (inclusi i sanguinamenti pericolosi per la vita e quelli fatali) Composito di sanguinamenti maggiori e non maggiori clinicamente rilevanti Sanguinamenti maggiori (criteri ISTH) Sanguinamenti maggiori (criteri ISTH) Età (anni) 71.5 (media) 73 (mediana) 70 (mediana) 72 (mediana) CHADS2 Score 2.1 3.5 2.1 2.8 TTR (medio%) 64 55 62 65 Analisi statistica Intention to treat • Per protocol • Intention to treat Intention to treat • Per protocol • Intention to treat RE-LY: stroke or systemic embolism Rischio cumulativo 0.05 0.04 Dabigatran 110 mg BID vs. warfarin: RR 0.90 (95% CI: 0.74–1.10) Non inferiorità: p<0.001 Superiorità: p=0.30 Dabigatran 150 mg BID vs. warfarin: HR 0.65 (95% CI: 0.52–0.81) Non inferiorità: p<0.001 Superiorità: p<0.001 Warfarin Dabigatran 110 mg BID 0.03 Dabigatran 150 mg BID 0.02 0.01 0.00 0.0 0.5 1.0 Dabigatran 150 mg BID vs warfarin: -35% Dabigatran 110 mg BID vs warfarin: -10% 1.5 2.0 2.5 Anni di osservazione BID = 1 somministrazione ogni 12 ore Connolly SJ et al. N Engl J Med 2010;363:1875–6 6 Ischaemic Stroke 1.4 1.4 -24% vs warfarin P=0.03 1.2 1.2 1 1 0.8 0.8 0.2 1.34 0.92 1.21 0 Dabigatran Dabigatran Warfarin 110 mg 150 mg N Engl J Med 2010;363:1875–6 2 +41% vs warfarin P<0.001 1,8 1 1,4 0.8 1,2 1 0.6 0,8 0.4 0,6 0,2 0 Rivaroxaban Warfarin N Engl J Med 2011;365:883-91 1.2 1,6 0,4 1.42 0.4 0.4 0 p = 0.581 0.6 0.6 0.2 1.32 p = 0.42 0.97 1.05 Apixaban Warfarin 0.2 1.25 Edoxaban 60 mg 1.77 1.25 0 Edoxaban Warfarin 30 mg N Engl J Med 2013;369:2093-104 N Engl J Med 2011;365:981-92 Haemorragic Stroke in RE-LY, ROCKET AF, ARISTOTLE, ENGAGE AF Warfarin Dabigatran 150 mg 0.5 Dabigatran 110 mg Rivaroxaban Apixaban Edoxaban 30 mg 0.47 0.47 0.45 0.4 Edoxaban 60 mg 0.44 0.76 0.35 Rate (x 100 0.3 patients 0.25 per 0.2 year) 0.26 HR 0.59 p=0.024 0.05 HR 0.51 p<0.001 HR 0.54 p<0.001 0.16 0.15 0.1 0.24 0.26 0.12 0.10 HR 0.33 p<0.001 HR 0.31 p<0.001 HR 0.26 p<0.001 0 RE-LY ROCKET-AF ARISTOTLE ENGAGE-AF Intracranial bleeding is less with dabigatran than with warfarin at any level of cTTR cTTR: Rate of intracranial bleeding (per 100 patients per year) 1 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 < 57.1% 57.1-65.5% 65.5-72.6% > 72.6% cTTR < 57.1% D 110 mg vs warfarin: HR 0.43 (0.19-1.00) D 150 mg vs warfarin: HR 0.53 (0.25-1.15) cTTR 57.1-65.5% D 110 mg vs warfarin: HR 0.31 (0.15-0.66) D 150 mg vs warfarin: HR 0.45 (0.24-0.88) cTTR 65.5-72.5% D 110 mg vs warfarin: HR 0.20 (0.07-0.58) D 150 mg vs warfarin: HR 0.35 (0.15-0.82) cTTR > 72.6% D 110 mg vs warfarin: HR 0.27 (0.11-0.66) D 150 mg vs warfarin: HR 0.39 (0.18-0.84) Dabigatran 110 mg BID Wallentin L et al. Lancet 2010;376:975–83 Dabigatran 150 mg BID Warfarin Major Bleedings in RE-LY, ROCKET AF, ARISTOTLE, ENGAGE AF Warfarin Dabigatran 150 mg 4 3.5 3 Dabigatran 110 mg 0.5 Rivaroxaban Apixaban Edoxaban 30 mg 3.60 3.57 3.43 3.45 3.31 3.09 2.87 2.75 HR 0.81 p=0.002 Rate 2.5 (x 100 patients 2 per year) 1.5 1 Edoxaban 60 mg HR 0.80 p<0.001 2.13 HR 0.71 p<0.001 1.61 HR 0.53 p<0.001 Lower with dabigatran 110 mg, apixaban and both doses of edoxaban versus warfarin 0 RE-LY ROCKET-AF ARISTOTLE ENGAGE-AF Gastrointestinal Bleedings in RE-LY, ROCKET AF, ARISTOTLE, ENGAGE AF Warfarin Dabigatran 150 mg 2 Dabigatran 110 mg Edoxaban 60 mg Rivaroxaban HR 1.49 p<0.001 1.62 1.6 Rate (x 100 1.2 patients 1 per 0.8 year) Edoxaban 30 mg 1.85 1.8 1.4 Apixaban 1.36 1.25 HR 1.09 P=0.44 1.51 HR 1.45 P<0.05 HR 1.23 P=0.03 1.23 1.12 0.86 0.76 HR 0.89 P=0.37 0.6 0.82 HR 0.67 p<0.001 0.4 Lower only with edoxaban 30 mg versus warfarin 0.2 Higher with dabigatran 150 mg, rivaroxaban and edoxaban 60 mg versus warfarin 0 RE-LY ROCKET-AF ARISTOTLE ENGAGE-AF Quindi, rispetto al warfarin, il dabigatran: • Riduce significativamente l’end-point primario e l’ictus ischemico (150 mg), o è equivalente al warfarin (110 mg) • Riduce drasticamente le emorragie endocraniche e l’ictus emorragico (110 mg e 150 mg) • Riduce significativamente le emorragie maggiori (110 mg), o è equivalente al warfarin (150 mg) • Aumenta le emorragie gastrointestinali (150 mg), o è equivalente al warfarin (110 mg) 0,9 Stroke/Systemic Embolism D150 ED30 0,8 Warf 0,7 0,6 0,5 ED60 0,4 Apix Riva D110 0,3 0,2 0,1 Probability of each rank Probability of each rank 1 1 2 3 4 5 6 ED30 Stroke D150 0,8 Warf 0,7 0,6 Apix 0,5 0,4 Riva ED60 D110 0,3 0,2 0,1 Ischaemic Stroke 0,9 ED30 D150 0,7 D110 0,6 0,5 Warf 0,4 Apix ED60 Riva 0,3 1 7 Probability of each rank 1 Probability of each rank 0,9 0 0 0,8 1 0,2 0,1 2 0,8 3 4 5 6 7 Warf Death 0,7 0,6 0,5 0,4 0,3 ED30 D150 ED60 0,2 Apix D110 0,1 Riva 0 0 1 2 3 Apixaban (Apix) 4 5 6 Dabigatran (D) 110 mg 150 mg 7 Edoxaban (ED) 30 mg 60 mg 1 2 3 4 Rivaroxaban (Riva) 5 6 7 Warfarin (Warf) Verdecchia P, Lip GYH, et al. Expert Opin Drug Saf. 2014 Oct 14:1-14. [Epub ahead of print] Major Bleeding ED30 0,9 Apix 0,8 D150 0,7 0,6 ED60 0,5 Warf D110 Riva 0,4 0,3 0,2 Probability of each rank Probability of each rank 1 Warf 0,8 0,7 0,6 D110 0,5 ED60 ED30 0,4 D150 Apix 3 4 0,3 0,2 0 0 2 3 4 5 6 Gastrointestinal Bleeding ED30 0,9 0,8 Apix 0,7 Riva Warf ED60 0,6 D150 D110 0,5 0,4 0,3 0,2 2 1 7 Probability of each rank 1 Probability of each rank Riva 0,9 0,1 0,1 1 Intracranial Bleeding 1 6 5 7 Myocardial Infarction 0,7 Riva 0,6 Warf 0,5 ED30 D110 D150 Apix 0,4 ED60 0,3 0,2 0,1 0,1 0 0 1 2 3 Apixaban (Apix) 4 5 6 Dabigatran (D) 110 mg 150 mg 7 Edoxaban (ED) 30 mg 60 mg 1 2 3 4 Rivaroxaban (Riva) 5 6 7 Warfarin (Warf) Verdecchia P, Lip GYH, et al. Expert Opin Drug Saf. 2014 Oct 14:1-14. [Epub ahead of print] Dabigatran 1. Lo studio RE-LY 2. Le indagini della Food and Drug Administration (FDA) 3. L’esperienza di Assisi Event Rates with Dabigatran (75 mg or 150 mg bid) vs Warfarin in 134 000 patients with AF aged ≥ 65 years Event Dabigatran (x 100 patient-years) (N=67 207) Warfarin (reference) (N=67207) Adjusted HR (95% CI) Ischemic stroke 1.13 1.39 0.80 (0.67-0.96) Intracranial hemorrhage 0.33 0.96 0.34 (0.26-0.46) Major Gastrointestinal bleeding Acute Myocardial Infarction 3,42 2,65 1.28 (1.14-1.44) 1,57 1,69 0.92 (0.78-1.08) Death 3,26 3,78 0.86 (0.77-0.96) Graham DJ et asl. Circulation 2014; October 30 -20% Adjusted HR: 0.80 (0.67-0.96); p=0.02 -66% Adjusted HR: 0.34 (0.26-0.46); p<0.001 Graham DJ et asl. Circulation 2014; October 30 +28% Adjusted HR: 1.28 (1.14-1.44); p=0.006 -14% Adjusted HR 0.86 (0.77-0.96); p=0.006 Dabigatran 1. Lo studio RE-LY 2. Le indagini della Food and Drug Administration (FDA) 3. L’esperienza di Assisi L’esperienza di Assisi Maria Gabriella Molini Claudia Bartolini Francesca Valecchi Adolfo Aita Letizia Di Giacomo Stefania Martone Paolo Verdecchia www.umbriafa.it Main Characteristics of Patients (1) Number 115 Age (years) 78.3 (8) Weight (Kg) 75.6 (13) Height (cm) 166.3 (10) Sex (% women) 53 Classification of AF (N, %) - New-onset 24 (21%) - Paroxysmal 12 (10%) - Persistent 30 (26%) - Permanent 49 (43%) Verdecchia P et al. Curr Op Drug Saf 2014 (in press) Distribution of CHA2DS2VASc 35 31 30 28 25 Per cent 20 of 15 Patients 10 16 10 10 5 3 1 0 2 3 4 5 6 7 8 CHA2DS2VASc Group Verdecchia P et al. Curr Op Drug Saf 2014 (in press) Terapie antitrombotiche/antiaggreganti assunte in precedenza Nulla 21% Warfarin 52% 18% Aspirina 9% Eparina Verdecchia P et al. Curr Op Drug Saf 2014 (in press) Sospensione Definitiva Trattamento Totale: 115 pazienti Sospeso Continuato N = 18 (16%) Cause sospensione definitiva: N = 97 (84%) Sospensione definitiva by Dabigatran dose: 11 su 76 pazienti (14%) con Dabigatran 110 mg 7 su 39 pazienti (18%) con Dabigatran 150 mg Sospensione definitiva: In media, 76 giorni dopo l’inizio del trattamento • Distress epigastrico: • Sanguinamento GI: • VFG < 30 ml/min: • Prurito intenso: • By pass aorto-coronarico: • Polmonite: Totale 10 pazienti 1 paziente 3 pazienti 1 paziente 2 pazienti 1 paziente 18 pazienti Dopo la sospensione: Warfarin: 7 pazienti; Altro NAO: 7 pazienti Né anticoagulanti né ASA: 4 pazienti Verdecchia P et al. Curr Op Drug Saf 2014 (in press) Tollerabilità Distress epigastrico Presente (N=25 21,7%) Assente (N=90) Diarrea Sanguinamenti Minori Presenti (N=9; 7,8%) Assente (N=106) Sanguinamenti Maggiori Presente (N=3 2,6%) Presenti (N=2; 1,7%) Assente (N=112) Assenti (N=113) Verdecchia P et al. Curr Op Drug Saf 2014 (in press) A che punto siamo con l’antidoto ? Idarucizumab An Antidote Specific to Dabigatran Restoration of coagulation Potent binding affinity ~350 times higher than the binding of dabigatran to thrombin No procoagulant or anticoagulant effects Short half-life Fully humanized antibody fragment (Fab) Easy and rapid administration IV administration, immediate onset of action Low risk of adverse reactions – No Fc receptor binding – No endogenous targets Idarucizumab is currently in development and is not approved for use in any country. The information presented here is intended for medical education purposes only Glund S et al. AHA 2013; abstract 17765; van Ryn J. AHA 2012; Presentation 9928; van Ryn J et al. Circulation 2012;126:A9928 Sept 2014 Healthy volunteer study: immediate, complete, and sustained reversal of dabigatran anticoagulation End of idarucizumab injection (5 min infusion) 70 Dabigatran plus: Placebo (n=9) 1 g idarucizumab (day 4) (n=9) 2 g idarucizumab (day 4) (n=9) 4 g idarucizumab (day 4) (n=8) Normal upper reference limit (n=86) Mean baseline (n=86) 65 dTT (s) 60 55 Dabigatran + placebo 50 45 40 35 30 –2 Dabigatran 0 2 4 6 8 10 12 24 36 48 60 72 Time after end of infusion (hours) Antidote Idarucizumab is currently in development and is not approved for use in any country. The information presented here is intended for medical education purposes only ‘Normal upper reference limit’ refers to (mean+2SD) of 86 predose measurements from a total of 51 subjects Glund S et al. AHA 2013; abstract 17765 29 Sept 2014 First patient trial of a NOAC-specific antidote Study to evaluate reversal of the anticoagulant effects of dabigatran with idarucizumab in: Bleeding patients – overt bleeding judged by the physician to require a reversal agent Surgical patients – require an emergency surgery or procedure for a condition other than bleeding Started in April 2014, currently recruiting in >35 countries worldwide Idarucizumab is currently in development and is not approved for use in any country. The information presented here is intended for medical education purposes only NCT02104947: Available at http://www.clinicaltrials.gov/ct2/show/NCT02104947; Accessed August 2014 30 Sept 2014 Grazie per la vostra attenzione Concomitant Use of Antiplatelet Therapy with Dabigatran or Warfarin 6.3 5.5 4.8 Rate of Major Bleeding (% per year) 4.6 4.4 5.4 4.3 3.9 2.8 3.8 2.6 2.2 Of 18 113 patients, 6952 (38.4%) received concomitant aspirin or clopidogrel, or both, at some time during the study (in 1 out of 5 for the total study duration). Dans M et al. Circulation 2013;127:634-640 La dose 75 mg bid (pazienti con VFG < 30 ml/min) è equivalente al warfarin per ictus ischemico, sanguinamenti GI e mortalità, ma pur sempre migliore del warfarin per emorragie endocraniche La dose 150 mg bid (pazienti con VFG > 30 ml/min) è migliore del warfarin per ictus ischemico, emorragie endocraniche e mortalità, e peggiore del warfarin per emorragie gastrointestinali Graham DJ et asl. Circulation 2014; October 30 Limitations 1. Lack of adjustment for confounders 2. Lack of detailed medical records review Drug-safety investigation, focused on the occurrence of bleeding, promoted by Food and Drug Administration (FDA) over the period October 19, 2010 to December 31, 2011. Southworth MR et al. N Engl J Med 2013 Effect of Dabigatran Plasma Concentrations and Patient Characteristics on Ischemic Stroke and Major Bleeding in AF Patients Reilly PA et al. J Am Coll Cardiol 2014;63:321–8 Italia: 60.600.000 individui Umbria: 897.000 individui (1,5% della popolazione Italiana) 2.730/135.000 piani terapeutici = 2.0% (rispetto ad 1,5% atteso)