Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
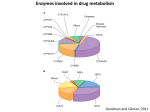
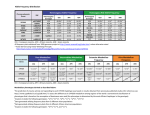
Farmacogenetica e farmacogenomica nell’anziano Dott. Davide Seripa Biologo Dirigente di Ricerca Laboratorio di Gerontologia-Geriatria ISTITUTO DI RICOVERO E CURA A CARATTERE SCIENTIFICO Ospedale “Casa Sollievo della Sofferenza” Opera di San Pio da Pietrelcina San Giovanni Rotondo (FG) http://www.operapadrepio.it In VI century B.C. Pythagoras reported that the adverse reaction to the ingestion of fava beans was attributable to a inter-individual differences! Ad personam optimization of drug treatments (Meyer, Nature Rev Genet 2004;5:669-676) 1866: Mendel establishes rules of heredity. 1959: Vogel coins the term pharmacogenetics (how genetics may influence drug response). 1962: Kalow publishes the first monograph on pharmacogenetics. 1987: First nomenclature of Cytochrome P450 (CYP) gene superfamily. 1988: Gonzalez and Meyer collaborate to clone CYP2D6 and characterize the genetic defect of the debrisoquine/sparteine polymorphism. 1997: The term pharmacogenomics first appears in the literature. 2003: The human genome sequence was completed. Future prospects for pharmacogenetics in the quest of personalized medicine (Howland, J Psychosoc Nurs Ment Health Serv 2012;50:13-16) The potential role of genome and its mechanism of maintenance, interactions and modifications in pharmacogenetics and adverse drug reactions is immense… but immense is complexity than assessing the role of a SNP. Pharmacogenomics: challenges and opportunities (Roden, Ann Internal Med 2006;145:749-757) Small effect Pharmacogenomics We are here! Large effect Pharmacogenetics Single gene Small number of genes Great number of genes Whole genome Evolution of the Cytochrome P450 (CYP) gene superfamily La vita conquista l’ambiente terrestre Gli animali diventano erbivori, assumono tossine vegetali, e muoiono. Innesco della pressione selettiva Duplicazione dei 3 geni CYP ancestrali Evidence for the evolution of CYP gene superfamily by gene duplications CYP3A3 CYP3A4 CYP3A5 CYP3A5P1 CYP3A5P2 Chromosome 7 CYP2C8 CYP2C9 CYP2C18 CYP2C19 Chromosome 10 CYP2D6 CYP2D7P CYP2D8P Chromosome 22 Variability of the CYP gene superfamily CYP3A4 20 allele families / 41 alleles CYP2D6 73 allele families / 120 alleles CYP2C9 34 allele families / 41 alleles. CYP2C19 26 allele families / 32 alleles. Nomenclature of the CYP gene superfamily Nomenclatura per gli alleli (isoenzimi) del Citocromo P450 (CYP) secondo il Comitato Internazionale per la Nomenclatura degli alleli del Citocromo 450 (*) CYP Citocromo P450 (superfamiglia genica) 2 Questo numero identifica la famiglia del gene D Questa lettera identifica la sottofamiglia del gene 6 Questo numero identifica il gene specifico (l’isoenzima proteico) * Tutto quello dopo l’asterisco riguarda l’identificazione dell’allele 4 Questo numero identifica la famiglia allelica A Questa lettera identifica l’allele specifico Maggiori famiglie geniche del CYP Famiglia CYP1: CYP1A1; CYP1A2; CYP1B1 Famiglia CYP2: Famiglia CYP3: CYP2A6; CYP2A13; CYP2B6; CYP2C8; CYP2C9; CYP2C19; CYP2D6; CYP2E1; CYP2F1; CYP2J2; CYP2R1; CYP2S1 CYP3A4; CYP3A5; CYP3A7; CYP3A43 Famiglia CYP4: CYP4A11; CYP4A22; CYP4B1 (*) Human Cytochrome P450 (CYP) Allele Nomenclature Committee (http://www.imm.ki.se/CYPalleles/) Substrates of the CYP gene system Is not a chance if most of drugs currently used in clinical practice are lipofilic compound derived from plant metabolites, and if about 80% of these drugs are metabolized by the CYP system. 2E1 2B6 2C19 4% 3% 8% P2A6 3% 3A4/A5 36% 1A2 11% 2C8/9 16% 2D6 19% Association between CYP2C9 genetic variants and warfarin-related outcomes 1.40 CYP2C9*2 (R144C) (Higashi, JAMA 2002) 2.39 CYP2C9*3 (I359L) (Higashi, JAMA 2002) 1.8 CYP2C9*2 (R144C) (Lindh, Clin Pharm Ther 2005) 2.2 CYP2C9*3 (I359L) Severe bleeding (Lindh, Clin Pharm Ther 2005) 2.57 CYP2C9*2 or *3 (R144C or I359L) Risk of bleeding (Margaglione, Thromb Haemost 2000) CYP2C9 *1/*1 wild type 0 1 2 3 4 No bleeding Vitamin K Oxide Reductase Complex 1 (VKORC1) polymorphisms and warfarin dose (Rieder, NEJM 2005;352: 2285-93) Maintenance dose of warfarin (mg/daily) 70% 0,62 60% 0,47 50% 40% 30% 0,27 20% 10% 0% A/A A/B A = low-dose haplotype group B = high-dose haplotype group B/B A genome-wide association study confirms VKORC1, CYP2C9 and CYP4F2 as principal genetic determinants of warfarin dose The first genome-wide association study (GWAS) on 1053 Swedish subjetcts (325.997 SNPs). The results were confirmed in 588 additional swedish patients (p < 0.0029) (Takeuchi, PLos Genet 2009;5:e1000433) CYP2C9 and VKORC1 genotypes explain about 30-40% of the total variation in the final warfarin dose The International Warfarin Pharmagenetics Consortium Estimation of the warfarin dose with clinical and pharmacogenetic data (New Engl J Med 2009;361:753-764) Derivation cohort = 4043 subjects Validation cohort = 1009 subjects Warfarin genotyping reduces hospitalization rates (Epstein, J Am Coll Cardiol 2010;55:2804-2812) ~ 900 patients with information on CYP2C9 and VKORC1 available to prescribing physicians versus historical control group 6 months after the initiation of warfarin therapy, hospitalizations for hemorrhage were 28% less common in the intervention than in control group Association of Cytochrome P4502C19 genotype with the antiplatelet effect and clinical efficacy of Clopidogrel (Shuldiner, JAMA 2009;302:849-858) rs12777823 polymorphism CYP2C19*2 variant in 227 patients undergoing percutaneous coronary intervention treated for 1-year with clopidogrel Platelet aggregation CV events and/or death p=0.02; HR=2.42,95%CI 1.18-4.99 p=0.02 50% 25% 40% 20% 30% 15% 20% 10% 10% 5% 0% 2C19*1/*1 2C19*1/*2 2C19*2/*2 (Ref.) 0% 2C19*1 (Ref.) 2C19*2 Reduced-function CYP2C19 genotype and risk of adverse outcomes in patients treated with clopidogrel (Mega, JAMA 2010;304:1821-1830) Meta-analysis of 9 studies evaluating 9685 patients (91.3% with PIC and 54.5% with acute coronary syndrome) 1.55 CYP2C19*1/*2 Risk of CV, MI or stroke 1.76 CYP2C19*2/*2 2.67 CYP2C19*1/*2 Risk of stent thrombosis 3.97 CYP2C19*2/*2 0.2 1 2 3 4 FDA Drug Safety Communication (Available at URL http://www.fda.gov/) February 2010 The FDA revised the label on Warfarin providing genotype-specific ranges of doses and suggesting that genotypes be taken into consideration when the drug is prescribed. The FDA added a boxed warning to prescribing information for clopidogrel: “persons with a CYP2C19 variant encoding a form of the enzyme associated with a low rate of metabolism might require dose adjustment or the use of a different drug” I FANS e l’emorragia gastroduodenale Reclutati (n = 78) Bleeding (n = 26) No bleeding (n = 52) Allele SNP-ID DNA change Protein change Enzyme activity CYP2C9*2 rs1799853 C430T Arg144Cys Decreased CYP2C9*3 rs1057910 A1075C Ile359Leu Decreased CYP2C9 genotyping may identify subgroups of persons who potentially are at increased risk of gastroduodenal bleeding when treated with NSAIDs metabolized by CYP2C9. I FANS e l’emorragia gastroduodenale p = 0.034 OR = 4.2 (1.1 - 16.2) Reference p < 0.001 OR = 15.8 (1.1 - 16.2) Il donepezil nel trattamento dell’Alzheimer 1) Lo SNP rs1080985 nel gene CYP2D6 può influenzare l’efficacia clinica del donepezil in pazienti con malattia di Alzheimer di grado lieve/moderato. 2) L’analisi dei genotipi del CYP2D6 può essere utile per identificare sottogruppi di pazienti con differente risposta terapeutica. • Mantenimento o miglioramento dello stato cognitivo (valutato tramite ADAS-Cog e MMSE) • Miglioramento dello stato funzionale (valutato tramite ADL o IADL) Le fenocopie Fenocopia Un fenotipo che somiglia ad un fenotipo genetico ma che ha cause ambientali. Inibitori del CYP2D6 Fenocopia (rispetto EM) Induttori del CYP2D6 Fenocopia (rispetto EM) Forti Moderati Deboli Bupropion Duloxetine Amiodarone PM Dexamethasone UM Fluoxetine Sertraline Cimetidine PM Rifampin UM Paroxetine Terbinafine Quinideine PM PM http://medicine.iupui.edu/clinpharm/ddis/table.asp Replication study confirm the role of CYP2D6 polymorphism rs1080985 on donepezil efficacy in Alzheimer’s disease patients (Albani, J Alzheimers Dis 2012;30:745-749) Multicenter, 415 AD patients, donepezil 10mg/day, 6 months follow-up Responders = 172; Non-responders = 243 ----- Multivariate analysis corrected for age, gender, MMSE at baseline, APOE-ε4 status. Results confirm the association between rs1080985 and response to donepezil after 6 months of treatment p < 0.05; OR 1.74, 95% CI 1.01-3.00 Il donepezil nel trattamento dell’Alzheimer Da 552 pazienti arruolati nello studio sono stati selezionati 37 responders e 19 non-responders p = 0.005; OR = 6.286 (1.828 - 21.667). Potenza dell’analisi = 84.87%. Pharmacogenomic protocols in CNS disorders and dementia (Cacabelos, Neurodegenerative Dis 2010;7:167-169) About 25% of the 100 most prescribed drugs in USA and western countries are psychotropic drugs currently used in dementia. A trigenic cluster integrating CYP2D6+CYP2C19+CYP2C9 polymorphic variants yealds 82 different genetic profiles in wich only 26% are normal (EM). These data clearly indicate that the incorporation of pharmacogenomic protocols to dementia reserach and clinical trials can foster therapeutics optimization by helping to develop cost-effective pharmaceuticals and improve drug eccicacy and safety Pharmacogenetics of risperidone and haloperidol CYP2D6 genotype and plasma concentration of psychotropic drugs RISPERIDONE (Scordo, Psychopharmacology 1999;147:300-305) HALOPERIDOL (Bertilsson, Br J Clin Pharmacol 2002;53:111-122) p<0.01 30 20 29,4 16,3 % 10 0 EM PM Defining the opportunity for pharmacogenetic intervention in primary care (Grice, Pharmacogenomics 2006;7:61-65) 607 patients in primary care (USA), 16 drugs cause ADRs Antidrepressants 9,60% Anti-hypertensive 14,30% Analgesics 88,50% 0% 20% 40% 60% 80% 100% 28.6% took > 1 of pharmacogenetic ADR-associated drugs Risk factors for ADRs: - Old age (p<0.001); Chronic disease (p<0.001); Number of drugs (p<0.001) Farmacogenetica dell’analgesia post-operatoria Dolore post-operatorio - protocolli terapeutici - L1 Lieve 40 pazienti consecutivi in terapia antidolorifica post-operatoria L2 M1 Moderato M2 Grave G Artrosilene Zantac Contramal Plasil Fentanest Morfina Protocollo terapeutico L1 L2 M1 M2 X X X X X X X X X X X X X X X X - A volte - G X X X X X Farmacogenetica dell’analgesia post-operatoria - protocolli terapeutici, farmaci e citocromi - Artrosilene (ketoprofene) Zantac (ranitidina) Contramal (tramadolo) Plasil (metoclopramide) Fentanest (fentanile) Morfina CYP1A2 - S+I - - - - CYP2B6 - - S - - - CYP2C8 I - - - - S CYP2C9 S+I - - - - - CYP2C19 - S - - - - CYP2D6 - S+I S+I S+I - S CYP3A4 - I S+I - S+I S CYP3A5 - I - - S - CYP3A7 - - - - S - CYP17A1 - - - I - - S: Substrato; I: Inibitore. http://www.drugbank.ca/ Farmacogenetica dell’analgesia post-operatoria - risposta terapeutica e fenotipo metabolico Medie stimate 5 4.5 4 Punteggio VAS 3.5 3 EM 2.5 IM 2 PM 1.5 1 0.5 0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Tempo (ore) EM versus IM: p = 0.015 – EM versus PM: p = 0.024 – IM vs PM: p < 0.001 Farmacogenetica dell’analgesia post-operatoria - considerazioni - 1. La sovrapposizione di substrati suggerisce che, probabilmente, in questi protocolli terapeutici non si ottiene una piena azione dei diversi farmaci (come se venissero usati singolarmente!). 2. La concomitante presenza di un azione inibitoria dei substrati verso l’enzima suggerisce un ulteriore diminuzione dell’azione dei diversi farmaci. 3. Visto che i protocolli terapeutici differiscono solo per il dosaggio dei diversi farmaci, come è possibile valutare con accuratezza l’effetto terapeutico dei diversi protocolli? 4. Queste considerazione suggeriscono con forza: a) L’impiego di un farmaco principale che non abbia una concomitante azione inibitoria per l’enzima; b) L’impiego di farmaci secondari che non presentino una sovrapposizione dei substrati con il farmaco principale. 5. In questo caso si otterrebbe: a) Una piena azione farmacologica; b) La possibilità di identificare e studiare in maniera inequivocabile la risposta al trattamento terapeutico, incluse le reazioni avverse. Risk of sudden death from cardiac causes according to use of CYP3A4 inhibitors and antibiotics in 1476 cases (Ray, New England J Med 2004;351:1089-1096) CYP3A4 INHIBITORS (nitroimidazole antifungal agents, diltiazem, verapamil, troleandomycin) 1.79 Erythromycin 1.48 Amoxicillin 5.35 Erythromycin + CYP3A4 inhibitors 0.2 1 3 5 7 Pharmacogenetics of acetaminophen I 1 2 ? II 1 ? 2 ? CYP2D6*1/*XN Although CYP2D6 metabolizes paracetamol into NAPQI (N-acetyl-p-benzoquinone imine) to a lesser extent than other P450 enzymes, its activity may contribute to paracetamol toxicity in extensive and ultrarapid metabolizers. Public Health Genomics Pharmacogenetics in Europe: Barriers and Opportunities European Commission Joint Research Center Challenges and measures in PGx development (Gurwitz, Public Health Genomics 2009; 12: 134-41) La farmacogenetica nella clinica geriatrica - prospettive futureCurrent Drug Metabolism 2011:12;621-634 Pharmacogenetics in Geriatric Medicine: Challenges and Opportunities for Clinical Practice Alberto Pilotto, Francesco Panza, and Davide Seripa In clinical practice several factors may explain the variable response to drug treatments, including functional and cognitive disabilities, malnutrition, organspecific failures, concomitant diseases, and concomitant therapies. This may seriously limiting the pharmacogenetic approach to drug prescription. Geriatric patients need a multidimensional approach to optimize their clinical care including treatments. The introduction in clinical practice of pharmacogenetics may be useful to improve the “clinical decision making” in drug treatments. PHARMACOGENETICS AS A “DOMAIN” OF THE MULTIDIMENSIONAL ASSESSMENT Davide Seripa ([email protected]) Laboratorio di Gerontologia-Geriatria Sig.ra Carolina Gravina Sig.ra Maria Urbano Dott.ssa Giulia Paroni Dott.ssa Grazia D’Onofrio Dott. Alberto Pilotto U.O.C. di Geriatria Dott. Antonio Greco Laboratorio Analisi Cliniche Dott. Lazzaro Di Mauro Sig.ra Antonietta P. Gallo Rianimazione 1 Dott.ssa Paola Latina U.O.C. Neurologia Policlinico Universitario “A. Gemelli” Prof. Carlo Masullo Dott. Antonio Daniele Istituto di Gerontologia e Geriatria Università degli Studi di Perugia Prof.ssa Patrizia Mecocci