Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
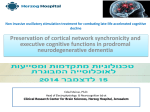
Section #: 66806 Deep Brain Stimulation: Reengineering the Electrical Impluses Behind Movement Disorders An Illumin Article Thomas Houser University of Southern California Dornsife School of Arts & Letters/ Viterbi School of Engineering Los Angeles, United States [email protected] Abstract – Much of the brain’s function, hidden deep within a vast array of electrical impulses, still remains a mystery. Millions of people are burdened with movement disorders such as Parkinson’s and dystonia, which stem form abnormal neural activity deep within the brain. Over the years there has been slow progress towards developing the most effective treatments, but in the past two decades deep brain stimulation has arisen as a promising avenue to pursue. Small high-frequency electrical impulses have allowed for the controlled manipulation of neural activity. The latest technological advances support the development of stimulating devices that utilize ultrasound to record and modulate the activity of the brain. These great strides in deep brain stimulation technology have provided us with a portal into the complex world of electrical neural activity, through which we can expect greater discoveries and the development of more effective medical technologies. Key Words – current; deep brain stimulation; dystonia; future; Parkinson’s disease; movement disorders; ultrasound neuromodulation Author Bio: Thomas Houser is a junior at the University of Southern California studying biomedical engineering and plans to graduate May 2015. He has a passion for the science of the human body and hopes to be at the cutting-edge of the health sciences of the future. Houser 2 I. Introduction Simply put, humans are nothing without electricity. If you are thinking this means humans are nothing without lights, computers or any of the latest electronics, you aren’t thinking deep enough and I challenge you generate a little more of your own electricity. All human functions, from seeing, breathing, moving and thinking are a product of electricity, all stemming from the brain. The human brain is constantly sending, receiving and interpreting electrical impulses carrying microscopic electrical potentials through an intricate maze of intertwined neurons (Fig. 1). This complex system allows the human brain to simultaneously carry out a multitude of unique tasks often without fail. Figure 1: Computer generated depiction of electrical impulses in the brain due to neural signals www.howitsworksdaily.com With such complexity comes the potential for failure. In the brain, this often takes the form of neurological conditions such as dystonia and Parkinson’s disease. All these conditions pertain to motor function and are therefore categorized as movement disorders [1]. Simply walking down the street or lifting a hand to grasp a cup, are seemingly simple tasks that millions of people suffering from these conditions struggle to do [2]. These physiological manifestations are a testament to the significance of the seemingly simple electrical impulses generated by our Houser 3 brain on our most basic functions. Our lack of complete understanding of the human brain has left people afflicted with these conditions to cope with the disease using slowly developing and less effective treatments [1]. The treatment of these diseases and our understanding of the brain are on the verge of phenomenal breakthrough with the introduction of new deep brain stimulation (DBS) devices. II. Condition’s Biological Background Each movement we make, conscious or not, relies on a series of neurological pathways that cascade signals throughout the body to induce a movement. When a person consciously decides to move a muscle, an executive decision is made within the sensory-motor cortex, generating your own electrical impulse [3]. This electrical impulse is channeled deeper into the brain to the forebrain and midbrain (Fig. 2). There this signal is split and captured by the basal ganglia and thalamus [3]. Within the basal ganglia the signal filtered and processed before being passed on to the thalamus, which shoots the signal down through the brain stem to the body [4]. http://deepblue.lib.umich.edu Figure 2: Image on the left displays the location of the basal ganglia in the brain. The schematic on the right depicts the mechanism of action within the basal ganglia. The green arrows designate excitatory signals (activate the receiving target) while the red arrows designate inhibitory signals (deactivates the receiving target). Houser 4 Mechanism of the Basal Ganglia The processing that takes place in the basal ganglia is the essential mechanism by which the brain filters movement signals [4]. Much like the processors found in my electronics we use today, the basal ganglia attempts to output a streamlined signal from a collection of messy inputs. The filtration occurs through two internal pathways, a direct pathway and an indirect pathway [3]. The direct pathway is also known as the excitatory pathway because it induces and excitatory action by the thalamus, promoting the passage of the signal onto the body. Conversely the indirect pathway is known as the inhibitory pathway, restriction the passage of signals onto the body [5]. These two pathways utilize four parts of the basal ganglia, the striatum, the subthalamic nucleus (STN), the internal globus pallidus (GPi) and the external globus pallidus (GPe) (Fig. 2). Motor Stimulation Pathway The overall process begins when the motor cortex sends excitatory signals, signals that will promote the action of the part, to the STN, thalamus, and striatum simultaneously (Fig. 2). In the direct pathway, also known as the excitatory pathway, the striatum sends an inhibitory signal directly to the GPi, preventing it from sending an inhibitory signal to the thalamus [5]. Therefore the thalamus remains in an excited state from the initial signal sent by the motor cortex, and relaying signals onto the body, bypassing any form of signal filtration. Through the indirect pathway, also known as the inhibitory pathway, the striatum sends an inhibitory signal to the GPe. Therefore, the GPe fails to send its regular inhibitory signal to the STN. Since the STN is not deactivated it will send an excitatory signal to the GPi, which will send its inhibitory signal to the thalamus. The resulting deactivated thalamus fails to relay signals out to the body [5]. Houser 5 The overall result of this inhibition is that the muscle one intended to move does not respond to the initial conscious decision made in the motor cortex to contract the muscle. Biological Manifestations The imbalance of pathway stimulation is seen in dystonia and Parkinson’s. When the excitatory pathway, overpowers the inhibitory pathway there is no restriction on the excitation of the thalamus and thus over excitation occurs. Image trying to flex your bicep, but simultaneously flexing your tricep, forcing your arm straight instead of bent. This is a product of the over-excitation seen in dystonia [2]. The over activity of the inhibitory pathway, prevents the relay of signals from the thalamus to the body, is reduced motor stimulation in those with Parkinson’s [6]. This drastic change in motor control is attributed to the malfunction of a tiny brain structure, the substantia nigra. It fails to produce dopamine, the chemical key to proper function of the striatum, the pathway regulator. Without dopamine the striatum predominantly induces the inhibitory pathway. III. Progression of Treatments Parkinson’s Disease The 1930s and 40s were the closing decades of experimental and seemingly radical treatment methods, especially for neurological disorders. The brain remained somewhat of a black box, within which trail and error had rendered physical manipulation of brain structures a viable treatment option. In the case of Parkinson’s, these brain structures included the STN and GPi, both inhibitors of the thalamus (Fig. 2) [8]. They found that lesioning, cutting or burning, away portions these structures stopped their restrictive function, allowing movement signals to more readily be sent to the body. This approach, seen as reckless, largely stopped with the introduction of the drug levodopa, which reintroduced dopamine to the striatum and promoted the balanced regulation of signal pathways in the basal ganglia [3]. The continued use of Houser 6 levodopa began to present adverse effects such as the development of excessive involuntary movement and motor fluctuations. The discovery of these adverse side effects coincided with the introduction of deep brain stimulation as a novel means of treatment. While seemingly harsh, the original approach of physically manipulating the brain was effective. Lending to the idea that there is a degree of control achievable only through physically intervention with which a drug cannot compare. The use of deep brain stimulation provided a novel means of less drastic, but more controlled and direct physical intervention through the use of small electrode stimulators implanted in the brain [6]. The development of implantable stimulation devices negated the practice of permanently damaging the basal ganglia, and turned to the basis of brain communication, electricity, as a means of manipulation [7]. Insolated nanowires connected to electrodes were surgically placed deep in the brain, on the surface of the STN or GPi, where they could provide modulated electrical stimulation, suppressing the output of the stimulated structure. Dystonia Given the opposing characteristic of dystonia and Parkinson’s, over stimulation and under stimulation, the progressions of treatments were quite similar. Opposed to inhibitory structures, excitatory structures were manipulated, such as the GPe or the thalamus (Fig. 2). Greater understanding of the neurological system lead to the development and implementation of novel drugs that manipulated the neurological system by suppressing the excessive activation signals being sent to the muscles from the unregulated thalamus [9]. Deep brain stimulation once again came along as a less destructive, but precise means of controlling the brain’s actions in comparison to lesioning. Unlike their use for Parkinson’s the electrodes for treating dystonia were placed on the GPe and thalamus. The use of deep brain stimulation has consistently produced the most effective and consistent results for treatment of both movement disorders [6]. Houser 7 IV. How Current Deep Brain Stimulation Devices Works Structural Design The deep brain stimulation, DBS, neurostimulators act much like a pacemaker, producing and sending high-frequency electric pulses to targeted structures within the brain [9]. The main device is often the size of a large rubber eraser, which houses its electronics and a battery pack. This rather large device is implanted underneath the skin just below the collarbone [5]. Thin, insolated wires run, beneath the skin, from the device up along the neck and through tiny boreholes at the top of the skull where they meet up with the electrodes that extend deep into the brain to the target structure (Fig. 3 & 4)[10]. www.webmd.com Figure 3: An X-ray image of the extension wires running beneath the skin from the implanted neurostimulator in the chest, through a borehole in the skull, and to electrodes implanted deep in the brain. Houser 8 Device Acclimation Following the surgical implantation, the device’s internal processor has to become acclimated the electrical environment of each patient’s brain. It does this with the help of a technician who runs diagnostic tests to measure the electrical signal patterns within the brain. These tests provide feedback information as to the specific amplitude, frequency, and pulsewidth that can alleviate the patient’s Parkinson’s or dystonia symptoms [5]. Once the device is fully functional it can recognize when the patient is entering a Parkinson’s or dystonia state and stimulate the appropriate structure with a pulse within the programmed parameters. Signal Recognition and Pulse Generation The most common sign of the brain entering a Parkinson’s or dystonia state is a change in the electrical signals produced within the deep brain. In the abnormal state both the amplitude and frequency of the neural signals increase beyond normal levels. These differences in signal are measured by additional microprobes that measure the electrical signals produced by neurons surrounding the target structures [8]. These differences cause the neurostimular to produce an electrical pulse that deactivates the target structures and returns the neural signal to its normal pattern, all at a moments notice. V. The Future of Deep Brain Stimulation Through years of analysis and attempted manipulation, scientists have discovered how complex and volatile a system the brain can be. Scientific advancement has guided us down an interesting road from killing, to drugging, to shocking the brain. One may ask what kind of crazy idea might emerge from the sparks of our minds next. The success of DBS in the treatment of movement disorders is indisputable, and a powerful guide to the next generation of neuromodulation. It is easy to see the weaknesses in the current method of stimulation, requiring Houser 9 such invasive procedures. Imagine a system that went no deeper than the skin, but conjured electrical stimulation deep within the brain. Step outside the electrical world of the brain and into the realm of ultrasound. Historically used for medical imaging, ultrasound has been shown to noninvasively stimulating brain activity. Figure 4: A depiction of the electrical field activity picked up by transducers on the surface of the skull. http://www.tylerlab.com/projects/ultrasound This groundbreaking development has provided mechanism by which ultrasound transducers can regulate the activity of targeted regions of the brain. Taking full advantage of the electronic world of the brain the transducers can monitor electrical activity within the deep brain from the surface of the skull [9]. Upon sensing changes in the magnetic fields generated by the brain, the transducers can identify abnormal activity and emit ultrasound signals into the deep brain generating counter electrical signals that return brain activity to its normal state [9]. This new technology will allow the scientific community to noninvasively explore the brain’s signaling processes like never before. By better understanding the electrical activity within the brain we can begin to devise unique therapies for a multitude of neurological disorders that have long plagued humanity. This developing technology breaks down barriers and provides promise to our understanding of the complex electrical world we call the human brain. Like with many things, sometimes the greatest perspective is the one you get when you step outside the box. Houser 10 VI. References [1] S. Young. “New Implantable Device Can Manipulate and Record Brain Activity.” Internet: http://www.technologyreview.com/news/517871/new-implantable-device-canmanipulate-and-record-brain-activity/, August 9, 2013 [October 10, 2013]. [2] M. Hariz et al. “Future of Brain Stimulation: New Targets, New Indications, New Technology.” Movement Disorders. Vol. 00, pp 1-9. [2013]. [3] J.L. Vitek. “Deep brain stimulation: How does it work?” Cleveland Clinic Journal of Medicine. Vol. 75 pp. 59-65. [4] M. Potter-Nerger & J. Volkmann.“Deep brain stimulation for gait and postural symptoms in Parkinson's disease.” Movement Disorders.Vol. 28, pp 1609-15. [5] J. Lee. “A Closed-Loop Deep Brain Stimulation Device with a Logarithmic Pipeline ADC.” Internet: http://deepblue.lib.umich.edu/bitstream/handle/2027.42/60733/milaca_1.pdf?seq uence=1, October 12, 2013. [2008] [6] F. Weaver et al. “Bilateral Deep Brain Stimulation vs Best Medical Therapy for Patients With Advanced Parkinson Disease” The Journal of the American Medical Association. Vol. 301, pp 63-73. [2009] [7] Mayo Clinic Staff. “Parkinson’s Disease” Mayo Clinic. Internet: http://www.mayoclinic.com/ health/parkinsons-disease. October 12, 2013. [May 12, 2012]. [8] H. Lee et al. “Electrical engram: how deep brain stimulation affects memory.” German Center for Neurodegenerative Diseases. [2011]. [9] Li, M. Monica, Pati, Sandipan, Tufail, Yusuf, and Yoshihiro, Anna. “Ultrasonic neuromodulation by brain stimulation with transcranial ultrasound.” Nature Protocols. [2012].