Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
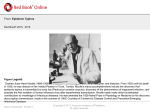
MURINE TYPHYS: AN EMERGING CAUSE OF NON-ERUPTIVE FEVER IN TRAVELERS RETURNING FROM TUNISIA Laura Gastellier, Fanny Lanternier, Aurélie Renvoisé, Sébastien Rivière, Didier Raoult, Olivier Lortholary and Marc Lecuit Université Paris Descartes, Hôpital Necker-Enfants Malades, Service des Maladies Infectieuses et Tropicales et Service de Microbiologie, Centre d'Infectiologie Necker-Pasteur, Assistance Publique-Hôpitaux de Paris, Paris, France WHO Collaborative Center for Rickettsioses (UMR CNRS 6236 – IRD 198), Marseille, France Institut Pasteur, Groupe Microorganismes et barrières de l’hôte, Paris France To whom correspondence should be addressed. E-mail: [email protected] Summary The prevalence of murine typhus in Tunisia is probably underestimated, because of its nonspecific signs and relatively benign evolution, and because of serum cross reactivity with Rickettsia conorii antigens. Mediterranean spotted fever is well known in Tunisia, whereas MT is mistakenly thought to have disappeared in the 1970’s.1 We report here a case of MT in a woman returning from Tunisia and hospitalized in France with acute non-eruptive fever. Murine typhus (MT), also known as endemic typhus, belongs to the typhus group of rickettsioses (TGR), together with epidemic typhus caused by Rickettsia prowazekii. TGR are louse- or flea-borne infections, whereas the other group of rickettsioses is the tick-borne group, responsible for Mediterranean spotted fever (MSF) caused by Rickettsia conorii. MT is caused by Rickettsia typhi, and its main vector is the rat flea Xenopsylla cheopis. Transmission of Rickettsia typhi to human may occur via fleabite and the feces of these fleas, whether inhaled or contaminating damaged skin. Nonetheless, more than half of the patients have no record of any contact with rats or fleas. MT incubation lasts from 7 to 14 days, and manifests as a usually mild disease, with nonspecific flu-like symptoms. It can occur worldwide, but most frequently in tropical coastal areas. Doxycycline is the treatment of choice and without antimicrobial therapy, fever lasts between 7 to 15 days whereas it resolves within 48 hours when doxycycline is used. A 41-year-old woman with no past medical history was hospitalized in August 2010 at the Centre d'Infectiologie Necker Pasteur, Paris, France for acute fever, just returning from a 5week stay in Tunisia. She had stayed in Mahdia, a rural zone in the Tunisian Sahel of Eastern Tunisia, approximately 15 km from the coast, where she had contacts with various domestic animals but did not recall of any fleabite. She reported a very abrupt onset of the first symptoms 7 days before admission: severe headache and vomiting but apyrexia, and became febrile with chills, sweating, nausea, myalgia and arthralgia, stiff neck, cough and abdominal pain 2 days thereafter. Clinical examination did not show any evidence of rash nor fleabite marks nor inoculation eschar but confirmed persistent high fever (39°C). Cerebrospinal fluid analysis was normal, as well as results of chest and abdominal CT scan, and standard biological analyses, except an increased CRP serum level (81 mg/L). Treatment with ceftriaxone was started 2 days after admission because typhoid fever was first suspected. Nonetheless, it was stopped on day 5 when no improvement was observed and blood cultures were negative and stool cultures were negative for Salmonella enterica. Two weeks after the onset of symptoms, a decrease in fever was observed and the patient was discharged. An immunofluroescence assay on a serum sample sent to the WHO collaborative Center for Rickettsioses in Marseille, France, found IgG and IgM antibodies to Rickettsia sp. Crossadsorption and Western blot analysis of a serum sample identified anti-R. typhi antibodies but not anti-R. prowazekii and anti-R. felis antibodies, establishing the diagnosis of MT in this patient2 []. Although malaria and arboviroses remain the most important causes of fever when returning from the tropics, rickettsial infections are of emerging importance in travelers,3 but very often the diagnosis is overlooked, either because the clinical presentation is non-specific and the diagnosis not evoked, or because no specific diagnostic tool is available to the clinician. Despite its global distribution, R. typhi has been primarily identified in coastal urban regions among rats and their fleas. Yet, this classic cycle has broadened to peridomestic animals including cats, dogs, opossums and their fleas. Thus, MT should be considered not only in travelers back from tropical countries with a dense rat population (Sub-Saharan Africa, Southeast Asia) but also in travelers back from developed areas worldwide including the USA (California, Texas, Hawaii),4 the Mediterranean area3 such as Greece, Cyprus, Italy (mainly in Sicily), Spain, Croatia, Slovenia, Algeria, Tunisia, Morocco, Egypt, Israel and pacific islands (Australia,5 New-Zealand,6 or Japan7). Angelakis et al. also recently reported 3 other cases of MT diagnosed in France in travelers returning from Tunisia.3 MT is usually a mild disease with non-specific symptoms including fever, headache, maculopapular rash, arthralgia and myalgia. MT is sometimes associated with more severe symptoms such as prostration and focal neurological deficits.8 Biological features also have a very poor specificity. Complete blood count can show anemia, early leukoneutropenia sometimes followed by polymorphonucleosis (most frequently the white blood cell count is normal) and thrombocytopenia. Elevated liver enzymes and elevated erythrocyte sedimentation rate as well as hyponatremia or hypokaliemia have been reported.9 In recent years, a wide array of rickettsioses has emerged throughout the world, because of improved clinician awareness and development of modern diagnostic tools (cross-adsorption and Western blotting assays, cell-based cultures and molecular methods such as PCR)10 Because results of serological testing allow a presumptive diagnosis, more sophisticated and direct methods are critical for the diagnosis and description of new rickettsial diseases, especially in atypical cases.11 A positive immunofluorescence assay for Rickettsia sp. can determine the genus but not the species, a cross-adsorption followed by Western blot has to be performed to determine the species. Therefore, in febrile returned travelers, when malaria and arboviroses have been eliminated, MT should be considered and the appropriate diagnostic tools be used in order to come up with a positive diagnosis ruling out other causes of fever, and help manage potential severe cases with appropriate doxycycline therapy. Figure 1: Cross-adsorption and immunoblotting Legend: The immunoblot signal observed on R. typhi, R. prowazekii and R. felis antigen extract lanes is abolished after cross adsorption on R. typhi antigens, demonstrating the presence of anti-R. typhi antibodies in the tested serum. NA: non-adsorbed; Rt, R. typhi; Rp, R. prowazekii; Rf. R. felis References 1.Kennou MF, Edlinger E., 1984. Current data on rickettsial diseases in Tunisia. Arch Inst Pasteur Tunis: 61(4):427-33. 2 La Scola B, Raoult D., 1997. Laboratory diagnosis of rickettsioses: current approaches to the diagnosis of old and new rickettsial diseases. J Clin Microbiol, 35:2715-27. 3.Angelakis E, Botelho E, Socolovschi C, Sobas CR, Piketty C, Parola P, Raoult D, 2010. Murine typhus as a cause of Fever in travelers from Tunisia and mediterranean areas. J Travel Med.: 17(5):310-5. 4. Adjemian J, Parks S, McElroy K, Campbell J, Eremeeva M, Nicholson W, McQuinston J and Taylor J, 2010. Murine Typhus in Austin, Texas, USA, 2008. Emerging Infectious Diseases: vol. 16, No. 3. 5. Graves S, Stenos J. Ann, 2009. Rickettsioses in Australia. N Y Acad Sci: 1166:151-5. 6. Sekra A, Irwin J, Reeve P, 2010. Urban rickettsiosis in the Waikato region of New Zealand. N Z Med J.;123(1315):71-4. 7. Sakaguchi S, Sato I, Muguruma H, Kawano H, Kusuhara Y, Yano S, Sone S, Uchiyama T, 2004. Reemerging murine typhus, Japan. Emerg Infect Dis: 10(5):964-5. 8. Civen Rachel and Ngo Van, 2008. Murine Typhus: An unrecognized suburban vectornorne disease. CID: 46 . 9. Letaïef A, Kaabia N, Chakroun M, Khalifa M, Bouzouaia N, Jemni L, 2005.Clinical and laboratory features of murine typhus in central Tunisia: a report of seven cases. Int J Infect Dis.;9(6):331-4. 10. Raoult D, Roux V., 1997. Rickettsioses as paradigms of new or emerging infectious diseases. Clin Microbiol Rev.; 10:694-719. 11. Rolain JM, Jensenius M, Raoult D, 2004. Rickettsial infections--a threat to travellers?. Curr Opin Infect Dis.;17(5):433-7.