Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
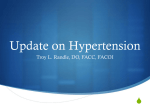
Seasonal Effects and Blood Pressure Blood Pressure Response to Patterns of Weather Fluctuations and Effect on Mortality Louise Aubinière-Robb,* Panniyammakal Jeemon,* Claire E. Hastie, Rajan K. Patel, Linsay McCallum, David Morrison, Matthew Walters, Jesse Dawson, William Sloan, Scott Muir, Anna F. Dominiczak, Gordon T. McInnes, Sandosh Padmanabhan Downloaded from http://hyper.ahajournals.org/ by guest on May 4, 2017 Abstract―Very few studies have looked at longitudinal intraindividual blood pressure responses to weather conditions. There are no data to suggest that specific response to changes in weather will have an impact on survival. We analyzed >169 000 clinic visits of 16 010 Glasgow Blood Pressure Clinic patients with hypertension. Each clinic visit was mapped to the mean West of Scotland monthly weather (temperature, sunshine, rainfall) data. Percentage change in blood pressure was calculated between pairs of consecutive clinic visits, where the weather alternated between 2 extreme quartiles (Q1–Q4 or Q4–Q1) or remained in the same quartile (Qn–Qn) of each weather parameter. Subjects were also categorized into 2 groups depending on whether their blood pressure response in Q1–Q4 or Q4–Q1 were concordant or discordant to Qn–Qn. Generalized estimating equations and Cox proportional hazards model were used to model the effect on longitudinal blood pressure and mortality, respectively. Qn–Qn showed a mean 2% drop in blood pressure consistently, whereas Q4–Q1 showed a mean 2.1% and 1.6% rise in systolic and diastolic blood pressure, respectively. However, Q1–Q4 did not show significant changes in blood pressure. Temperature-sensitive subjects had significantly higher mortality (1.35 [95% confidence interval, 1.06–1.71]; P=0.01) and higher follow-up systolic blood pressure (1.85 [95% confidence interval, 0.24–3.46]; P=0.02) compared with temperature-nonsensitive subjects. Blood pressure response to temperature may be one of the underlying mechanisms that determine long-term blood pressure variability. Knowing a patient’s blood pressure response to weather can help reduce unnecessary antihypertensive treatment modification, which may in turn increase blood pressure variability and, thus, risk. (Hypertension. 2013;62:190-196.) Online Data Supplement • Key Words: blood pressure ■ hypertension T here is growing evidence that outdoor temperature is a major determinant of the observed seasonal fluctuations in blood pressure (BP) with higher and lower BP in winter and summer, respectively.1–6 An inverse association between ambient temperature and BP has been observed in several studies.7–9 Thermoregulatory vasoconstriction, which increases arterial BP significantly,10 is an adaptive response to provide enhanced circulatory function for the protective mechanisms that are activated to maintain temperature in cold weather (nonshivering thermogenesis and increased metabolic rate).2,11 Elevation of BP induced by a longer period of cold exposure is not reversible after return to a thermo-neutral temperature in animal studies12 and may result in cold-induced hypertension. Although several studies explored the effects of seasonal variations on BP, few studies have looked at longitudinal BP changes in relation to fluctuations in weather patterns. To our knowledge, there are no studies that examined the role ■ mortality ■ temperature ■ weather of sunshine, rain, or air frost on BP. It is unclear whether BP response to weather parameters like temperature, rainfall, frost, and sunshine is similar in everybody. If there is heterogeneity in weather-related BP response, it would be important to know whether intraindividual and interindividual responsiveness to weather changes can predict long-term risk. The aim of this study was to determine the within-subject changes in BP in response to a range of weather patterns and test whether individual BP response to the weather is predictive of long-term mortality and BP control in a large hypertensive cohort. Methods Study Population The Glasgow Blood Pressure Clinic provides secondary and tertiary level service to individuals with hypertension from the West of Scotland. The details of the study population and settings, clinical Received December 18, 2012; first decision January 8, 2013; revision accepted April 15, 2013. From the BHF Glasgow Cardiovascular Research Centre, Institute of Cardiovascular and Medical Sciences, University of Glasgow, Glasgow, United Kingdom. *L.A.-R. and P.J. contributed equally to this article. This paper was sent to Gerald DiBona, Consulting editor, for review by expert referees, editorial decision, and final disposition. The online-only Data Supplement is available with this article at http://hyper.ahajournals.org/lookup/suppl/doi:10.1161/HYPERTENSIONAHA. 111.00686/-/DC1. Correspondence to Sandosh Padmanabhan, Institute of Cardiovascular and Medical Sciences, University of Glasgow, Glasgow G12 8TA, United Kingdom. E-mail [email protected] © 2013 American Heart Association, Inc. Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.111.00686 190 Aubinière-Robb et al Weather and Mortality 191 measurements, and outcome assessment are explained in the onlineonly Data Supplement and also described previously.13 individuals to show the BP changes were over and above the expected annual treatment–induced changes in BP. Results Weather Data The monthly average weather data for the West of Scotland were obtained from the UK meteorologic office (www.metoffice.gov.uk). The UK meteorologic office provides monthly average data sets of 13 climate variables that were generated for the periods 1961–2000 using a consistent analysis method. Values were produced for each station in the meteorologic Office’s observing network and for a 1×1 km grid of points covering the United Kingdom.14 The data generated for the West of Scotland region, available free of cost for research purposes, were used in the current study. Subject Visit Classification by Weather Conditions Downloaded from http://hyper.ahajournals.org/ by guest on May 4, 2017 Each clinic visit of the patient was mapped to the mean monthly weather (air frost, mean temp, sunshine, and rainfall) of the West of Scotland from meteorologic data. The mean monthly weather variables were categorized into quartiles. Further analyses were restricted to pairs of consecutive clinic visits within a 12-month period where the weather alternated between 2 extreme quartiles or remained in the same quartile. Thus, 3 groups were generated, Q1–Q4, where the first visit weather variable was in the lowest quartile (Q1) and the subsequent visit in the highest quartile (Q4); Q4–Q1, where the first visit was in the highest weather variable quartile (Q4) and the second visit in the lowest quartile (Q1); Qn–Qn, where both the first and the second visits were in the same weather variable quartile. All the clinic visits of each patient were thus classified throughout the entire follow-up period. Thus, BP changes in relation to weather changes were calculated every year, making these calculations specific for the weather conditions of the annual time-frame and BP control status of the patient in the same time frame. Statistical Analysis The baseline characteristics of the subjects were compared by independent t test for continuous variables and χ2 test for categorical variables. The traits analyzed were the percentage change in systolic BP, diastolic BP (DBP), and heart rate (HR) between 2 consecutive clinic measurements ≥30 days apart but within a 12-month period. The upper limit of time interval between each pair of BP measurements was 6 months. The direction and magnitude of ΔBP (ΔHR) in Qn–Qn were considered the weather independent effect on BP (ΔHR) between 2 visits and can reflect intrinsic BP (ΔHR) variability and effect of clinic interventions on BP (ΔHR). The ΔBP (ΔHR) values within each year were considered as paired measurements and were compared using paired t tests. Subjects were categorized into 2 groups based on the direction and magnitude of response in the Q1–Q4/Q4–Q1 groups compared with Qn–Qn. The 2 groups included a concordant response (same direction of response in Qn–Qn and Q1–Q4/Q4–Q1) group and a discordant response (opposite direction of response in Qn–Qn and Q1–Q4/Q4–Q1) group. The former group was termed the temperature, sunlight, or rain nonsensitive, and the latter group was termed the temperature, sunlight, or rain sensitive. Generalized estimating equations were used to model the longitudinal change, during the first 5 years of follow-up, in BP and HR in the weather-sensitive and weather-nonsensitive groups after adjustment for baseline variables. Kaplan–Meier survival and Cox proportional hazards models were set up to analyze differences in survival between the weather-sensitive and weathernonsensitive groups. The covariates included in the Cox proportional hazards models were baseline age, sex, body mass index, smoking status, systolic BP (SBP) or DBP, alcohol use, tobacco use, estimated glomerular filtration rate, and cardiovascular comorbidity. Because this is a real-life clinic setting, our strategies to ensure that the BP differences observed were over and above treatment-related BP changes included the following: (1) using pairwise BP differences obtained within a 12-month period, (2) using Qn–Qn BP change as the reference indicating the treatment-induced change in BP within the 12-month period, (3) restricting each pairwise comparison with the same 12-month period, and (4) using generalized estimating equations in temperature-sensitive and temperature-nonsensitive Baseline Characteristics of the Cohort The characteristics of the study cohort are presented in Table 1. More than half (53%) of the participants were women. The sample was middle aged (mean age, 51 years) and overweight (mean body mass index, 28 kg/m2). The average duration of follow-up was 6.5±5.8 years, during which BP changes in relation to weather fluctuations were analyzed. Twenty-eight percentage of patients attained target BP of <140/90 and maintained it at that level for ≥1 year. Effect of Weather Conditions on BP Trends in BP change by weather patterns (air frost, mean temperature, sunshine, and rainfall) are presented in Table 2, and annual SBP change by temperature is shown in Figure 1. There were 16 411 to 19 049 pairs of consecutive visits in the Qn–Qn group, 3115 to 6656 in the Q4–Q1 group, and 3916 to 6445 pairs of consecutive visits in the Q1–Q4 group. Qn–Qn showed an average of 2.1% (95% confidence interval [CI], 1.9–2.3), 2.2% (95% CI, 2.0–2.4), 1.7% (95% CI, 1.5– 1.9), and 2.2% (95% CI, 2.0–2.3) drop in SBP for air frost, temperature, rainfall, and sunshine, respectively. Similar drop in DBP was also observed for each weather variable. Q4–Q1 showed an average 2% increase in BP in response to temperature (2.1; 95% CI, 1.6–2.6) and sunshine (2.3; 95% CI, 1.9–2.6), but air frost and rainfall showed no significant difference. Q1–Q4 showed an average 1.4% (95% CI, 0.9–1.8) and 0.8% (95% CI, 0.5–1.1) increase in BP in response to air frost and rainfall, respectively. The temperature response of BP in Q1–Q4 was inconsistent across different years. Using the BP response in Qn–Qn as the reference trait, the differences in BP response to weather variation were assessed using paired t tests (Table 3). Compared with Qn–Qn, the change from the highest to the lowest quartile (Q4–Q1) elicited a 6% rise Table 1. Characteristics of the Cohort Variables Men (n=7574) Women (n=8436) Total (n=16 010) Age at first visit, years, mean (SD) 50.00 (13.40) BMI, kg/m2, mean (SD) 27.64 (5.19) 51.57 (15.60) 50.82 (14.63) 27.63 (6.27) 27.63 (5.79) 165.44 (30.76) 163.90 (29.23) 98.09 (15.21) 96.33 (23.11) 97.16 (19.79) Total cholesterol, mmol/L, mean (SD) 5.83 (1.56) 6.03 (1.34) 5.94 (1.45) eGFR <60 mL/min per 1.73 m2, n (%) 1158 (18.71) 1939 (28.36) 3097 (23.78) Alcohol use, n (%) 5001 (74.85) 3452 (46.00) 8453 (59.59) Tobacco use, n (%) 3393 (49.15) 3128 (40.32) 6521 (44.48) CVD, n (%) 1361 (19.21) 1172 (14.81) 2533 (16.89) 88 806.04 104 076.55 192 882.6 SBP, mm Hg, mean (SD) 162.18 (27.32) DBP, mm Hg, mean (SD) Time at risk (person-years), total BMI indicates body mass index; CVD, cardiovascular disease; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; and SBP, systolic blood pressure. 192 Hypertension July 2013 Table 2. Change in Blood Pressure and Heart Rate in Response to Weather Conditions Qn–Qn Response SBP DBP HR Q4–Q1 Q1–Q4 Environment n Mean % Change (95% CI) n Mean % Change (95% CI) n Mean % Change (95% CI) Air frost 17 418 –0.021 (–0.023 to –0.019) 6656 –0.002 (–0.006 to 0.002) 3916 0.014 (0.009 to 0.018) Mean temp 16 411 –0.022 (–0.024 to –0.02) 3115 0.021 (0.016 to 0.026) 6445 0.001 (–0.004 to 0.005) 0.007 (0.004 to 0.011) Rain 19 378 –0.014 (–0.016 to 0.012) 4316 –0.016 (–0.02 to –0.012) 6226 Rainfall 19 049 –0.017 (–0.019 to 0.015) 3837 –0.017 (–0.021 to –0.013) 6357 0.008 (0.005 to 0.011) Sunshine 17 431 –0.022 (–0.023 to 0.02) 5113 0.023 (0.019 to 0.026) 4688 –0.006 (–0.012 to –0.001) Air frost 17 416 –0.019 (–0.021 to 0.017) 6654 3916 0.009 (0.003 to 0.015) Mean temp 16 410 –0.021 (–0.023 to 0.019) 3114 0.016 (0.009 to 0.023) 6444 –0.001 (–0.004 to 0.002) Rain 19 376 –0.014 (–0.015 to –0.012) 4316 –0.014 (–0.018 to –0.01) 6225 0.008 (0.005 to 0.011) Rainfall 19 049 –0.016 (–0.018 to –0.015) 3836 –0.014 (–0.018 to –0.01) 6355 Sunshine 17 429 –0.019 (–0.021 to –0.018) 5112 0.019 (0.015 to 0.024) 4688 –0.007 (–0.011 to –0.004) –0.003 (–0.006 to 0) 0.007 (0.004 to 0.01) Downloaded from http://hyper.ahajournals.org/ by guest on May 4, 2017 Air frost 7545 0.005 (0.002 to 0.008) 3258 0.007 (0.002 to 0.011) 2088 0.003 (–0.002 to 0.009) Mean temp 6929 0.006 (0.003 to 0.009) 1630 0.004 (–0.002 to 0.01) 3245 0.006 (0.001 to 0.01) Rain 8760 0.005 (0.002 to 0.007) 1487 0.006 (–0.001 to 0.013) 2238 0.007 (0.001to 0.012) Rainfall 8353 0.003 (0.001 to 0.006) 1452 0.003 (–0.004 to 0.01) 2139 0.006 (0 to 0.011) Sunshine 7704 0.007 (0.004 to 0.009) 2575 0.007 (0.002 to 0.012) 2322 0.006 (0 to 0.011) CI indicates confidence interval; DBP, diastolic blood pressure; HR, heart rate; n, number of pairs of BP measurements; and SBP, systolic blood pressure. in SBP (mean difference [95% CI], 6.2 [5.1–7.4]; P<0.0001) for temperature and sunshine (6.0 [5.0–7.0]; P<0.0001), and 4% rise in SBP for air frost (4.1 [3.0–5.1]; P<0.0001). DBP showed significant differences only for temperature and sunshine. Intraindividual differences in BP response between Qn–Qn and Q1–Q4 (change from the lowest to the highest quartile of weather) showed 2.0% to 6.6% increases in SBP for air frost, temperature, rainfall, and sunshine, which were statistically significant. For DBP, similar statistically significant responses were seen for temperature, rainfall, and sunshine (Table 3). Effect of Weather Variation on HR HR did not show any significant intraindividual differences for any weather pattern (Table 3). Longitudinal Outcomes by Response to Weather Changes Tables S1 to S3 in the online-only Data Supplement present the sample characteristics stratified according to the SBP response to temperature, sunshine, and rainfall. There were no major differences in baseline characteristics between study groups. Generalized estimating equation analyses performed for longitudinal BP change, during the first 5 years of followup after adjustment for all conventional covariates, showed a 4/2 mm Hg annual decrease in SBP/DBP, which reflects the average effect of treatment in the clinic aimed at lowering BP. Comparing Qn–Qn with Q4–Q1, temperature-sensitive individuals (discordant response between Qn–Qn and Q4–Q1) had a 2.68 mm Hg SBP rise (95% CI, 0.61–4.75; P=0.01) and 1.84 mm Hg DBP rise (95% CI, 0.78–2.91; P=0.001) longitudinally >5 years compared with the temperature-nonsensitive subjects after adjustment for all baseline covariates (Table 4). Similarly, a 1.31 mm Hg SBP rise (95% CI, –0.25 to 2.87) and a 1.22 mm Hg DBP rise (95% CI, 0.42–2.01) were observed for sunlight. Comparing Qn–Qn with Q4–Q1, temperature-sensitive individuals (discordant SBP change between Qn–Qn and Q4–Q1) showed a 1.85 mm Hg SBP rise (95% CI, 0.24–3.46) longitudinally >5 years for temperature, and 2.04 mm Hg SBP rise (95% CI, 0.82–3.27) for sunlight in comparison with temperature- or sunlight-nonsensitive individuals after adjustment for baseline covariates (Table 4). Kaplan–Meier survival analyses (Figure 2A), temperaturenonsensitive individuals (Qn–Qn versus Q4–Q1) showed longer Figure 1. Patterns of systolic blood pressure (SBP) change annually across sequential visits. Each point is the mean percentage change in BP between 2 sequential clinic visits for 3 temperature groups. Aubinière-Robb et al Weather and Mortality 193 Table 3. Intraindividual Change in Blood Pressure and Heart Rate in Response to Weather Conditions Trait SBP DBP HR Weather n Pairs QnQn–Q4Q1 QnQn–Q1Q4 Q1Q4–Q4Q1 Mean % Change (95% CI) P Value* n Pairs Mean % Change (95% CI) P Value* n Pairs Mean % Change (95% CI) P Value* Air frost 1690 0.041 (0.03 to 0.051) <0.001 1568 0.048 (0.038 to 0.058) <0.001 672 0.018 (0.001 to 0.035) 0.04 Mean temp 1124 0.062 (0.051 to 0.074) <0.001 1434 0.055 (0.043 to 0.066) <0.001 542 –0.018 (–0.037 to 0.001) 0.07 Rain 2014 0.006 (–0.003 to 0.015) 0.20 2704 0.029 (0.021 to 0.036) <0.001 1324 0.023 (0.012 to 0.035) <0.001 Rainfall 1755 0.004 (–0.005 to 0.013) 0.33 2856 0.028 (0.02 to 0.035) <0.001 1078 0.028 (0.016 to 0.041) <0.001 Sunshine 1480 0.06 (0.05 to 0.07) <0.001 1330 0.034 (0.023 to 0.045) <0.001 834 –0.046 (–0.061 to –0.032) <0.001 Air frost 1690 0.033 (0.023 to 0.043) <0.001 1568 0.035 (0.026 to 0.044) <0.001 672 0.012 (–0.003 to 0.027) 0.12 Mean temp 1124 0.046 (0.036 to 0.057) <0.001 1434 0.05 (0.04 to 0.061) <0.001 542 –0.015 (–0.033 to 0.003) 0.11 Rain 2014 0.005 (–0.003 to 0.013) 0.25 2703 0.027 (0.02 to 0.034) <0.001 1324 0.024 (0.013 to 0.035) <0.001 Rainfall 1755 0.004 (–0.004 to 0.012) 0.35 2855 0.025 (0.018 to 0.032) <0.001 1077 0.023 (0.011 to 0.034) <0.001 Sunshine 1480 0.053 (0.043 to 0.062) <0.001 1330 0.04 (0.03 to 0.051) <0.001 834 –0.036 (–0.05 to –0.022) <0.001 Downloaded from http://hyper.ahajournals.org/ by guest on May 4, 2017 Air frost 610 0.012 (–0.006 to 0.03) 0.185 762 –0.007 (–0.02 to 0.006) 0.29 328 0.008 (–0.013 to 0.03) 0.44 Mean temp 552 –0.016 (–0.032 to –0.001) 0.07 539 –0.007 (–0.025 to 0.011) 0.47 250 –0.011 (–0.037 to 0.015) 0.41 –0.004 (–0.028 to 0.02) Rain 515 0.003 (–0.014 to 0.021) 0.69 766 –0.008 (–0.022 to 0.006) 0.27 314 Rainfall 506 0 (–0.017 to 0.017) 0.99 791 0.001 (–0.013 to 0.014) 0.91 268 Sunshine 699 –0.013 (–0.029 to 0.004) 0.12 575 0.001 (–0.016 to 0.018) 0.93 406 0.012 (–0.013 to 0.038) 0 (–0.021 to 0.02) 0.75 0.35 0.98 CI indicates confidence interval; DBP, diastolic blood pressure; HR, heart rate; and SBP, systolic blood pressure. *Bonferroni P=0.0008. Discussion survival in comparison with temperature-sensitive individuals (log rank P=0.015). In the Qn–Qn versus Q1–Q4 comparison, the results were not statistically significant (Figure 2B). Similar results were seen in BP response to sunshine. In the Cox proportional hazard model, temperature-sensitive individuals (SBP change between Qn–Qn and Q4–Q1) showed a 35% (HR [95% CI], 1.35 [1.06–1.71]; P=0.01) increased all-cause mortality compared with temperaturenonsensitive individuals (Table 5). A similar effect was seen for sunshine. No significant difference was observed for Qn–Qn versus Q1–Q4. In this study, we show for the first time the magnitude of change in BP attributable to changes in weather between sequential clinic visits of treated patients with hypertension. The results for temperature and sunshine were similar, whereas those for rainfall were in the opposite direction to temperature. The BP response to temperature observed in our study is consistent with the findings of other observational studies. For example, in asymptomatic individuals every 10°C decrease in the minimum temperature was associated with a 1.85 and 1.18 mm Hg increase in SBP and DBP, respectively.7 Table 4. Blood Pressure Response to Weather Conditions in the First Year of Treatment and On-Treatment Changes in Blood Pressure Temperature Response SBP, mm Hg (Qn–Qn vs Q4–Q1) n/N Weather nonsensitive Weather sensitive 0.011 1.31 (–0.25 to 2.87) 1.00 1.85 (0.78 to 2.91) 0.31 (–1.37 to 2.00) 1.20 (–0.08 to 2.48) 0.066 609/2834 1.00 0.001 0.715 1.00 0.286 755/3511 470/2192 P 1136/5384 1.12 (–0.94 to 3.19) 1.00 GEE β (95% CI) 1.00 0.101 1.00 0.946 487/2241 Weather sensitive n/N 609/2834 474/2219 0.07 (–1.88 to 2.01) Weather nonsensitive P 1.00 470/2192 Weather sensitive GEE β (95% CI) Rain 755/3511 2.68 (0.62 to 4.75) Weather nonsensitive DBP, mm Hg (Qn–Qn vs Q1–Q4) n/N 1.00 Weather sensitive DBP, mm Hg (Qn–Qn vs Q4–Q1) P 487/2241 Weather nonsensitive SBP, mm Hg (Qn–Qn vs Q1–Q4) GEE β (95% CI) Sunlight 1.22 (0.42 to 2.01) 1.00 0.003 474/2219 0.88 (–0.01 to 1.78) 0.053 1136/5384 1.00 1.00 0.52 (–0.48 to 1.52) 1.27 (0.20 to 2.34) 1.00 0.020 0.65 (–0.03 to 1.33) 0.063 Individuals with ≥3 annual BP readings are included in the GEE analyses. GEE analyses is adjusted for age, sex, body mass index, smoking status, alcohol use status, eGFR, chronic kidney disease status, and year of blood pressure assessment. CI indicates confidence interval; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; GEE β, generalized estimating equations regression coefficient; n/N=number of groups/number of observations; Q1–Q1, consecutive visits in the same weather conditions; Q4–Q1, consecutive visits in contrasting weather conditions (high-low); Q1–Q4, consecutive visits in contrasting weather conditions (low-high); and SBP, systolic blood pressure. 194 Hypertension July 2013 Downloaded from http://hyper.ahajournals.org/ by guest on May 4, 2017 Figure 2. A, Kaplan–Meier plot of all-cause mortality in relation to systolic blood pressure (SBP) response to temperature (Q4–Q1). B, Kaplan–Meier plot of all-cause mortality in relation to SBP response to temperature (Q1–Q4). BP changes with temperature in similar magnitude have been observed in other cohorts as well.8,15,16 We also show that the effect of temperature on BP varies between individuals and, based on response, patients can be classified as either temperature sensitive or temperature nonsensitive. We show that temperature-sensitive individuals have a higher follow-up BP and poorer survival compared with temperature-nonsensitive individuals. To our knowledge, this is the first time that weather parameters, such as temperature, sunshine, and rainfall, have been shown to be determinants of BP changes in the population. However, only temperature response was an independent predictor of mortality, emphasizing the prognostic role of temperature changes. There are several physiological explanations for the effect of temperature on BP. Cold exposure activates the sympathetic nervous system, which, in turn, increases the activity of the renin–angiotensin system.17 The renin–angiotensin system suppresses endothelial NO synthase expression and decreases NO production,18 which contributes to the development of cold-induced hypertension. The renin–angiotensin system also mediates the cold-induced increase in endothelin-1 production,11 a potent regulator of vascular tone and BP. Cold exposure upregulates endothelin-A but downregulates endothelin-B receptors and mediates the thermoregulatory vasoconstriction. The Pressioni Arteriose Monitorate E Loro Associazioni (PAMELA) study showed that summer–winter differences in BP were seen not only in normotensive subjects, but also in untreated and treated subjects with hypertension, indicating that weather is a powerful determinant of BP variability (BPV).6 Other mechanisms postulated to account for the BP increase in cold weather include alterations in skin vasomotor tone, resulting in a marked increase in vascular peripheral resistance; decreased sweating and, therefore, salt loss, increasing the load of sodium on the kidneys, thus, further contributing to the increase in BP; increased norepinephrine and epinephrine concentrations in plasma and urine accompanying the BP increase during the cold season; increased erythrocyte deformability and blood viscosity, a major determinant of systemic vascular resistances; a reduced intensity in ultraviolet light during winter has been shown to reduce the epidermal photosynthesis of vitamin D3 and parathyroid hormone, which was shown in turn to be associated with elevated BP levels.19–22 Table 5. Cox-PH Model for All-Cause Mortality and Blood Pressure/Pulse Rate Response to Weather Conditions Temperature Response SBP (Qn–Qn vs Q4–Q1) Deaths (n) Weather nonsensitive Weather sensitive 0.01 1.18 (0.98–1.44) 1.00 1.17 (0.94–1.47) 0.95 (0.82–1.10) 1.00 1.14 (0.90–1.46) 1.00 0.28 0.83 (0.68–1.00) 0.06 772 1.00 0.72 0.48 405 1.00 0.18 0.38 1.00 188 1.04 (0.82–1.32) 0.92 (0.75–1.09) 0.37 265 284 P Value 772 0.90 (0.71–1.13) 1.00 HR (95% CI) 1.00 0.09 1.00 0.49 291 Weather sensitive Deaths (n) 405 297 0.92 (0.73–1.16) Weather nonsensitive P Value 1.00 284 Weather sensitive HR (95% CI) Rain 391 1.35 (1.06–1.71) Weather nonsensitive DBP (Qn–Qn vs Q1–Q4) Deaths (n) 1.00 Weather sensitive DBP (Qn–Qn vs Q4–Q1) P Value 291 Weather nonsensitive SBP (Qn–Qn vs Q1–Q4) HR (95% CI) Sunlight 0.97 (0.73–1.30) 1.00 0.86 1.03 (0.86–1.25) 0.72 HRs are adjusted for age, sex, alcohol use, smoking status, estimated glomerular filtration rate, chronic kidney disease status, and baseline systolic blood pressure. CI indicates confidence interval; Cox-PH, Cox proportional hazards; DBP, diastolic blood pressure; HR, hazard ratio; Q1–Q1, consecutive visits in the same weather conditions; Q4– Q1, consecutive visits in contrasting weather conditions (high-low); Q1–Q4, consecutive visits in contrasting weather conditions (low-high); and SBP, systolic blood pressure. Aubinière-Robb et al Weather and Mortality 195 Downloaded from http://hyper.ahajournals.org/ by guest on May 4, 2017 Our finding that temperature-sensitive individuals have higher mortality is in line with current data on visit-tovisit BPV, which is associated with increased mortality.23–25 It is difficult to determine whether the high risk seen in temperature-sensitive individuals is attributable to BPV or to the physiological mechanisms activated in response to temperature changes. There is evidence for both mechanisms. Temperature influences BPV,26 and BPV has an impact on survival.27 In summer, a reduction in cardiovascular mortality has also been observed with a reduction in the occurrence of stroke in patients with hypertension.28–31 The cardiovascular morbidity and mortality associated with seasonal changes may be mediated through BP response to temperature changes. In a study conducted among 1222 consecutive individuals who sought medical consultation in hypertension outpatient clinics, lower ambient temperature was associated with increased aortic pulse pressure and poor subendocardial viability ratio.32 Low environmental temperature has been strongly associated with increased hospital admissions for acute myocardial infarction, stroke, and higher cardiovascular mortality.33,34 The strengths of the current study include the following: a large cohort of ≈16 000 adults with hypertension, >169 000 clinic visits, the availability of repeat BP measurements, 35 years of follow-up for mortality with median survival time of 32 years, and the ability to link clinic visits with mean monthly weather changes. Although the previous studies compared the BP changes recorded in different subjects in different seasons, we have compared changes in the same individual. We were strictly limited to analyze the weather-related variables in their range observed in the region of West of Scotland and the availability of informative BP data based on clinic visits occurring in the right sequence with each weather condition. Our study has limitations. We have used the average of 2 clinic BP measurements obtained under indoor clinic conditions. This is likely to have underestimated the weather effects on BP. Also ambient conditions in clinic will be different from those at work and at home for each patient. We are also limited by the unavailability of ambulatory BP monitoring or home BP readings to correlate out of office BP with clinic BP measurements and their response to weather conditions. Ambulatory BP monitoring would offer a more reliable assessment of the actual effect of changing weather conditions on daily life BP, including the separate assessment of weatherinduced changes on daytime and nighttime BP.6,26 Although we used BP measurements within a 12-month period, the limitation of studying a real-life cohort of patients is the absence of a fixed interval for assessment of BP, because BP changes over a longer period of time may be significantly influenced by seasonal weather changes in contrast to BP changes over a shorter period of time. The age-related increase in BP and the effect of other baseline variables may confound longitudinal assessment of BP response to temperature, despite our strategy to use BP difference within each year. We have not been able to study the role of antihypertensive agents in modulating the BP response to weather changes because of incomplete prescribing data available for this analysis. Furthermore, we did not have reliable physical activity data to include in our models. Finally, our study cohort comprised treated patients with hypertension, and the results may not be generalizable. Perspectives Response to weather (especially temperature) can be reflected in BP and is specific to the individual. BP response to temperature may be one of the underlying mechanisms that determine long-term BPV. Knowing a patient’s BP response to weather can help reduce unnecessary antihypertensive treatment modification, which may in turn increase BPV and, thus, risk. It remains to be established whether BP response to temperature or BPV is the causal determinant of increased risk, or whether it is the underlying autonomic function status of the individual that is causal and BPV is just a reflection of this. Acknowledgments We thank the patients and staff at the Glasgow Blood Pressure Clinic at the Western Infirmary in Glasgow and National Health Service Greater Glasgow and Clyde. Sources of Funding P. Jeemon is supported by a Wellcome Trust Capacity Strengthening Strategic Award to the Public Health Foundation of India and a consortium of UK universities. Disclosures None. References 1.Brook RD, Weder AB, Rajagopalan S. “Environmental hypertensionology” the effects of environmental factors on blood pressure in clinical practice and research. J Clin Hypertens (Greenwich). 2011;13:836–842. 2. Adamopoulos D, Vyssoulis G, Karpanou E, Kyvelou SM, Argacha JF, Cokkinos D, Stefanadis C, van de Borne P. Environmental determinants of blood pressure, arterial stiffness, and central hemodynamics. J Hypertens. 2010;28:903–909. 3.Giaconi S, Ghione S, Palombo C, Genovesi-Ebert A, Marabotti C, Fommei E, Donato L. Seasonal influences on blood pressure in high normal to mild hypertensive range. Hypertension. 1989;14:22–27. 4. Kent ST, Howard G, Crosson WL, Prineas RJ, McClure LA. The association of remotely-sensed outdoor temperature with blood pressure levels in REGARDS: a cross-sectional study of a large, national cohort of AfricanAmerican and white participants. Environ Health. 2011;10:7. 5. Lewington S, Li L, Sherliker P, et al; China Kadoorie Biobank study collaboration. Seasonal variation in blood pressure and its relationship with outdoor temperature in 10 diverse regions of China: the China Kadoorie Biobank. J Hypertens. 2012;30:1383–1391. 6.Sega R, Cesana G, Bombelli M, Grassi G, Stella ML, Zanchetti A, Mancia G. Seasonal variations in home and ambulatory blood pressure in the PAMELA population. Pressione Arteriose Monitorate E Loro Associazioni. J Hypertens. 1998;16:1585–1592. 7.Hong YC, Kim H, Oh SY, Lim YH, Kim SY, Yoon HJ, Park M. Association of cold ambient temperature and cardiovascular markers. Sci Total Environ. 2012;435–436:74–79. 8.Alpérovitch A, Lacombe JM, Hanon O, Dartigues JF, Ritchie K, Ducimetière P, Tzourio C. Relationship between blood pressure and outdoor temperature in a large sample of elderly individuals: the Three-City study. Arch Intern Med. 2009;169:75–80. 9.Barnett AG, Sans S, Salomaa V, Kuulasmaa K, Dobson AJ; WHO MONICA Project. The effect of temperature on systolic blood pressure. Blood Press Monit. 2007;12:195–203. 10.Greif R, Laciny S, Rajek A, Doufas AG, Sessler DI. Blood pressure response to thermoregulatory vasoconstriction during isoflurane and desflurane anesthesia. Acta Anaesthesiol Scand. 2003;47:847–852. 11. Sun Z. Cardiovascular responses to cold exposure. Front Biosci (Elite Ed). 2010;2:495–503. 12.Shechtman O, Papanek PE, Fregly MJ. Reversibility of cold-induced hypertension after removal of rats from cold. Can J Physiol Pharmacol. 1990;68:830–835. 196 Hypertension July 2013 Downloaded from http://hyper.ahajournals.org/ by guest on May 4, 2017 13. Paul L, Jeemon P, Hewitt J, McCallum L, Higgins P, Walters M, McClure J, Dawson J, Meredith P, Jones GC, Muir S, Dominiczak AF, Lowe G, McInnes GT, Padmanabhan S. Hematocrit predicts long-term mortality in a nonlinear and sex-specific manner in hypertensive adults. Hypertension. 2012;60:631–638. 14. Perry M, Hollis D. The development of a new set of long-term climate averages for the UK. Int J Climatol. 2005;25:1023–1039. 15. Kimura T, Senda S, Masugata H, Yamagami A, Okuyama H, Kohno T, Hirao T, Fukunaga M, Okada H, Goda F. Seasonal blood pressure variation and its relationship to environmental temperature in healthy elderly Japanese studied by home measurements. Clin Exp Hypertens. 2010;32:8–12. 16. Madsen C, Nafstad P. Associations between environmental exposure and blood pressure among participants in the Oslo Health Study (HUBRO). Eur J Epidemiol. 2006;21:485–491. 17. Sun Z, Cade R, Morales C. Role of central angiotensin II receptors in cold-induced hypertension. Am J Hypertens. 2002;15(1 pt 1):85–92. 18.Sun Z, Cade R, Zhang Z, Alouidor J, Van H. Angiotensinogen gene knockout delays and attenuates cold-induced hypertension. Hypertension. 2003;41:322–327. 19.Hata T, Ogihara T, Maruyama A, Mikami H, Nakamaru M, Naka T, Kumahara Y, Nugent CA. The seasonal variation of blood pressure in patients with essential hypertension. Clin Exp Hypertens A. 1982;4:341–354. 20. Rostand SG. Ultraviolet light may contribute to geographic and racial blood pressure differences. Hypertension. 1997;30(2 pt 1):150–156. 21. Sharma BK, Sagar S, Sood GK, Varma S, Kalra OP. Seasonal variations of arterial blood pressure in normotensive and essential hypertensives. Indian Heart J. 1990;42:66–72. 22. Cuspidi C, Ochoa JE, Parati G. Seasonal variations in blood pressure: a complex phenomenon. J Hypertens. 2012;30:1315–1320. 23. Mancia G, Bombelli M, Facchetti R, Madotto F, Corrao G, Trevano FQ, Grassi G, Sega R. Long-term prognostic value of blood pressure variability in the general population: results of the Pressioni Arteriose Monitorate e Loro Associazioni Study. Hypertension. 2007;49:1265–1270. 24. Rothwell PM, Howard SC, Dolan E, O’Brien E, Dobson JE, Dahlöf B, Sever PS, Poulter NR. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet. 2010;375:895–905. 25.Rothwell PM, Howard SC, Dolan E, O’Brien E, Dobson JE, Dahlöf B, Poulter NR, Sever PS; ASCOT-BPLA and MRC Trial Investigators. Effects of β blockers and calcium-channel blockers on within-individual variability in blood pressure and risk of stroke. Lancet Neurol. 2010;9:469–480. 26. Modesti PA, Morabito M, Bertolozzi I, Massetti L, Panci G, Lumachi C, Giglio A, Bilo G, Caldara G, Lonati L, Orlandini S, Maracchi G, Mancia G, Gensini GF, Parati G. Weather-related changes in 24-hour blood pressure profile: effects of age and implications for hypertension management. Hypertension. 2006;47:155–161. 27. Muntner P, Shimbo D, Tonelli M, Reynolds K, Arnett DK, Oparil S. The relationship between visit-to-visit variability in systolic blood pressure and all-cause mortality in the general population: findings from NHANES III, 1988 to 1994. Hypertension. 2011;57:160–166. 28. van Rossum CT, Shipley MJ, Hemingway H, Grobbee DE, Mackenbach JP, Marmot MG. Seasonal variation in cause-specific mortality: are there high-risk groups? 25-year follow-up of civil servants from the first Whitehall study. Int J Epidemiol. 2001;30:1109–1116. 29. Donaldson GC, Robinson D, Allaway SL. An analysis of arterial disease mortality and BUPA health screening data in men, in relation to outdoor temperature. Clin Sci (Lond). 1997;92:261–268. 30. Jakovljević D, Salomaa V, Sivenius J, Tamminen M, Sarti C, Salmi K, Kaarsalo E, Narva V, Immonen-Räihä P, Torppa J, Tuomilehto J. Seasonal variation in the occurrence of stroke in a Finnish adult population. The FINMONICA Stroke Register. Finnish Monitoring Trends and Determinants in Cardiovascular Disease. Stroke. 1996;27:1774–1779. 31. Sheth T, Nair C, Muller J, Yusuf S. Increased winter mortality from acute myocardial infarction and stroke: the effect of age. J Am Coll Cardiol. 1999;33:1916–1919. 32. Adamopoulos D, Vyssoulis G, Karpanou E, Kyvelou SM, Argacha JF, Cokkinos D, Stefanadis C, van de Borne P. Environmental determinants of blood pressure, arterial stiffness, and central hemodynamics. J Hypertens. 2010;28:903–909. 33. Danet S, Richard F, Montaye M, Beauchant S, Lemaire B, Graux C, Cottel D, Marécaux N, Amouyel P. Unhealthy effects of atmospheric temperature and pressure on the occurrence of myocardial infarction and coronary deaths. A 10-year survey: the Lille-World Health Organization MONICA project (Monitoring trends and determinants in cardiovascular disease). Circulation. 1999;100:E1–E7. 34.Dilaveris P, Synetos A, Giannopoulos G, Gialafos E, Pantazis A, Stefanadis C. CLimate Impacts on Myocardial infarction deaths in the Athens TErritory: the CLIMATE study. Heart. 2006;92:1747–1751. Novelty and Significance What Is New? Summary • The effect of temperature on blood pressure varies between individuals Response to weather (especially temperature) can be reflected in BP and is specific to the individual. Individuals with temperaturesensitive BP are at higher risk of early death. It remains to be established whether BP response to temperature or BP variability induced is the causal determinant of increased risk. and, based on response, patients can be classified as either temperature sensitive or temperature nonsensitive. Temperature-sensitive individuals have a higher follow-up blood pressure (BP) and poorer survival compared with temperature-nonsensitive individuals. What Is Relevant? • Intraindividual BP change in response to ambient temperature may identify patients with hypertension at high risk. Blood Pressure Response to Patterns of Weather Fluctuations and Effect on Mortality Louise Aubinière-Robb, Panniyammakal Jeemon, Claire E. Hastie, Rajan K. Patel, Linsay McCallum, David Morrison, Matthew Walters, Jesse Dawson, William Sloan, Scott Muir, Anna F. Dominiczak, Gordon T. McInnes and Sandosh Padmanabhan Downloaded from http://hyper.ahajournals.org/ by guest on May 4, 2017 Hypertension. 2013;62:190-196; originally published online May 6, 2013; doi: 10.1161/HYPERTENSIONAHA.111.00686 Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2013 American Heart Association, Inc. All rights reserved. Print ISSN: 0194-911X. Online ISSN: 1524-4563 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://hyper.ahajournals.org/content/62/1/190 Data Supplement (unedited) at: http://hyper.ahajournals.org/content/suppl/2013/05/06/HYPERTENSIONAHA.111.00686.DC1 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Hypertension is online at: http://hyper.ahajournals.org//subscriptions/ Supplementary Material Blood Pressure Response to Patterns of Weather Fluctuations and Effect on Mortality Louise Aubinière-Robb,* Panniyammakal Jeemon,* Claire E Hastie, Rajan K Patel, Linsay McCallum, David Morrison, Matthew Walters, Jesse Dawson, William Sloan, Scott Muir , Anna F Dominiczak, Gordon T McInnes, Sandosh Padmanabhan Expanded methods: Study Population The Glasgow Blood Pressure Clinic (GBPC) provides secondary and tertiary level service to individuals with hypertension from the West of Scotland. All patients referred to the BP clinic had a diagnosis of hypertension made in primary care using definitions of hypertension based on contemporaneous guidelines and if appropriate treatment commenced in primary care. All patients were treated at GBPC until their BP control was stabilized with continuing follow-up at the BP clinic or in primary care. The frequency of visits to GBPC mainly depended on individual patient BP levels and presence of other co-morbidities. The West of Scotland research ethics service (WoSRES) of National Health Service approved the study in GBPC database (11/WS/0083). Clinical Measurements The GBPC employs specialist hypertension nurses who are experienced and highly trained in BP measurement. The procedure required subjects to rest for 5 minutes in a seated position before BP was manually measured using standardized mercury sphygmomanometers. Three BP measurements were performed, one minute apart, and the mean of the second and third measurements was recorded. Blood pressure was measured consistently in the same arm for each patient at every visit. No assessment of inter-arm BP difference was possible as the data was not available in the database. Heart rate was measured over one minute manually. Patients attending the clinic were advised to take their regular medications as usual. Each patient attended the same clinic, therefore at each visit their BP measurement would occur in the same 3 hour time window either in the morning or afternoon. Consumption of food and drink, and level of physical exertion before each clinic appointment, could not be controlled. Drug substitution, addition and dose adjustment occurred during follow-up and in accordance with clinical guidelines.14,15 Prescribed medications were cross checked with patients at each clinic visit, and they were advised to comply with their treatment at all times. However formal concordance testing was unavailable. Outcome Assessment Record linkage with the General Register Office for Scotland ensured notification of a subject’s death (provided that it occurred in the United Kingdom) together with the primary cause of death according to the International Classification of Diseases, 10th Revision, Version for 2007 (ICD-10) codes. We considered cardiovascular deaths (CVD mortality; ICD-10 codes I00-I99), ischemic heart disease deaths (IHD mortality; ICD-10 codes 120I25), and stroke deaths (stroke mortality; ICD-10 codes I60-I69) in the analysis. Deaths other than due to cardiovascular causes are classified as non-CVD deaths. Mortality data were collected up to April 2011 allowing a maximum of 35 years for participants who had been under follow up for the longest time. Table S1: Characteristics of study populations stratified by groups based on blood pressure response to temperature Clinical Variable SBP mmHg (Qn-Qn Vs Q4-Q1) SBP mmHg (Qn-Qn Vs Q1-Q4) Same Direction Opposite Same Direction Opposite Direction (n=473) Direction (n=544) P Value (n=532) (n=596) P Value 51.97 (14.16) 53.18 (13.04) 0.156 51.30 (14.32) 52.40 (14.71) 0.203 Age at first visit (years), mean (SD) 230 (48.63) 283 (52.02) 0.281 254 (47.74) 289 (48.49) 0.802 Men, n (%) 27.77 (5.55) 27.67 (6.04) 0.791 28.07 (6.82) 27.95 (5.38) 0.753 BMI (Kg/m2), mean (SD) 167.06 (29.06) 167.73 (28.94) 0.714 162.69 (26.09) 162.10 (29.21) 0.726 SBP (mmHg), mean (SD) 98.02 (14.89) 99.41 (14.76) 0.136 96.57 (13.49) 96.23 (14.97) 0.691 DBP (mmHg), mean (SD) 5.94 (1.33) 0.232 5.79 (1.21) 5.92 (1.24) 0.106 Total cholesterol (mmol/l), mean (SD) 5.84 (1.13) 118 (25.17) 0.436 107 (22.86) 118 (22.82) 0.988 eGFR <60 mL/min per 1.73 m2, n(%) 108 (27.62) 231 (57.32) 287 (61.59) 0.201 276 (59.74) 315 (60.11) 0.905 Alcohol Use, n (%) Tobacco Use, n (%) 185 (44.79) 242 (46.69) 0.143 202 (42.17) 235 (43.84) 0.591 106 (25.30) 113 (23.01) 0.422 92 (18.81) 119 (21.64) 0.259 CVD, n (%) 147.63 (24.37) 150.42 (23.92) 0.067 145.01 (21.47) 147.99 (21.78) 0.021 Achieved SBP (mmHg), mean (SD) 88.13 (13.53) 88.81 (12.63) 0.407 86.92 (10.90) 87.32 (12.18) 0.566 Achieved DBP (mmHg), mean (SD) SBP=systolic blood pressure, SD=standard deviation, BMI=body mass index, DBP=diastolic blood pressure, eGFR=estimated glomerular filtration rate, CVD=cardiovascular disease. Table S2: Characteristics of study populations stratified by groups based on blood pressure response to sunshine Clinical Variable SBP mmHg (Qn-Qn Vs Q4-Q1) SBP mmHg (Qn-Qn Vs Q1-Q4) Same Direction Opposite Same Direction Opposite Direction (n=650) Direction (n=710) P Value (n=493) (n=541) P Value 51.02 (14.47) 52.21 (13.97) 0.125 52.80 (14.91) 51.98 (13.20) 0.351 Age at first visit (years), mean (SD) 297 (45.69) 332 (46.76) 0.693 229 (46.45) 274 (50.65) 0.177 Men, n (%) 27.73 (5.50) 27.39 (5.23) 0.247 27.90 (6.10) 27.79 (5.46) 0.752 BMI (Kg/m2), mean (SD) 165.33 (28.55) 166.14 (28.68) 0.603 168.06 (27.50) 164.63 (30.01) 0.057 SBP (mmHg), mean (SD) 97.64 (14.90) 98.22 (14.29) 0.459 98.02 (14.87) 98.44 (14.67) 0.648 DBP (mmHg), mean (SD) 5.91 (1.25) 0.727 5.86 (1.31) 6.02 (1.24) 0.058 Total cholesterol (mmol/l), mean (SD) 5.93 (1.26) 180 (26.71) 0.927 112 (26.23) 130 (26.80) 0.845 eGFR <60 mL/min per 1.73 m2, n(%) 161 (26.48) 358 (57.84) 412 (60.77) 0.283 262 (59.68) 311 (63.60) 0.22 Alcohol Use, n (%) Tobacco Use, n (%) 271 (42.54) 314 (45.31) 0.31 190 (41.39) 223 (44.07) 0.401 129 (20.03) 164 (23.40) 0.135 105 (22.53) 95 (18.48) 0.116 CVD, n (%) 146.17 (21.12) 148.91 (22.22) 0.02 148.43 (23.89) 150.17 (23.11) 0.236 Achieved SBP (mmHg), mean (SD) 87.40 (11.77) 88.47 (11.52) 0.093 87.90 (11.55) 89.40 (11.61) 0.039 Achieved DBP (mmHg), mean (SD) SBP=systolic blood pressure, SD=standard deviation, BMI=body mass index, DBP=diastolic blood pressure, eGFR=estimated glomerular filtration rate, CVD=cardiovascular disease. Table S3: Characteristics of study populations stratified by groups based on blood pressure response to rainfall Clinical Variable SBP mmHg (Qn-Qn Vs Q4-Q1) SBP mmHg (Qn-Qn Vs Q1-Q4) Same Direction Opposite Same Direction Opposite Direction (n=581) Direction (n=631) P Value (n=982) (n=1182) P Value 51.19 (13.57) 50.51 (13.64) 0.385 51.02 (13.94) 51.56 (13.76) 0.366 Age at first visit (years), mean (SD) 275 (47.33) 312 (49.45) 0.462 483 (49.19) 587 (49.66) 0.825 Men, n (%) 27.65 (6.11) 27.37 (5.28) 0.398 27.48 (5.42) 27.36 (5.46) 0.622 BMI (Kg/m2), mean (SD) 171.98 (26.41) 168.56 (29.28) 0.034 171.16 (28.42) 170.38 (29.51) 0.532 SBP (mmHg), mean (SD) 99.73 (13.78) 101.36 (14.28) 0.261 100.50 (14.72) 100.88 (15.65) 0.567 DBP (mmHg), mean (SD) 6.20 (1.31) 0.682 6.10 (1.33) 6.09 (1.23) 0.867 Total cholesterol (mmol/l), mean (SD) 6.17 (1.35) 129 (21.72) 0.768 226 (25.34) 268 (24.32) 0.601 eGFR <60 mL/min per 1.73 m2, n(%) 117 (21.01) 374 (68.25) 400 (66.33) 0.49 593 (64.95) 740 (66.31) 0.522 Alcohol Use, n (%) Tobacco Use, n (%) 254 (42.28) 302 (49.27) 0.171 456 (48.82) 515 (45.02) 0.084 127 (22.36) 135 (21.74) 0.797 223 (23.60) 275 (23.83) 0.901 CVD, n (%) 149.19 (20.88) 150.04 (22.28) 0.493 149.46 (21.59) 151.72 (23.65) 0.022 Achieved SBP (mmHg), mean (SD) 87.63 (9.95) 88.90 (11.25) 0.038 88.97 (11.62) 89.68 (12.27) 0.169 Achieved DBP (mmHg), mean (SD) SBP=systolic blood pressure, SD=standard deviation, BMI=body mass index, DBP=diastolic blood pressure, eGFR=estimated glomerular filtration rate, CVD=cardiovascular disease.