Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
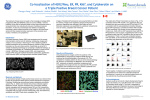
Klauschen et al. Computer assisted Ki67 scoring in the GeparTrio breast cancer study cohort Supplemental methods Comparison of different intensity classes Ki67 stained histological images are characterized by the presence of more than two intensity classes, such as no tissue, tissue but no cell nuclei, Ki67 negative cell nuclei and Ki67 positive cell nuclei each showing a certain haematoxylin intensity (Fig. 1A and B). Supp. Figure 1: A) Ki67 stained breast cancer tissue. B) Haematoxylin Signal derived from color deconvolution (1) and C) histogram showing frequencies (y axis) of specific heamatoxylin intensities (x axis) of the image background (red) and foreground (green). Arrows show representative locations of different intensity classes: no tissue (red), tissue but no cell nuclei (blue), Ki67 negative cell (green) and Ki67 positive cell nuclei (orange). Ki67 threshold finding method The threshold finding method presented in this study is based on the assumption that the “real” Ki67 staining fits the positive cell nuclei. That means that IHC staining signal that is found within the image background or only partly matches the cell nuclei is considered a “false” (or unspecific) signal. To compute the best matching Ki67 threshold first, the IHC- and Hematoxylin counter-stain are separated through color deconvolution (1). Consecutively, all possible thresholds ti (1..255) are tested and true positive (tp), false positive (fp) and false negative (fn) events are computed as follows: tp: number of Ki67 positive pixels that belong to a cell nucleus fp: number of Ki67 positive pixels that belong to the image background fn: number of Ki67 negative pixels that belong to a cell nucleus with at least one Ki67 positive pixel Then the precision and recall measures are computed (Eq. 1 and 2) and outlined to the F-score (Eq. 3) which is the harmonic mean of precision and recall. 𝑃𝑟𝑒𝑐𝑖𝑠𝑖𝑜𝑛 = 𝑡𝑝 𝑡𝑝 + 𝑓𝑝 (1) Klauschen et al. Computer assisted Ki67 scoring in the GeparTrio breast cancer study cohort 𝑅𝑒𝑐𝑎𝑙𝑙 = 𝐹 =2∗ 𝑡𝑝 𝑡𝑝 + 𝑓𝑛 𝑃𝑟𝑒𝑐𝑖𝑠𝑖𝑜𝑛 ∗ 𝑅𝑒𝑐𝑎𝑙𝑙 𝑃𝑟𝑒𝑐𝑖𝑠𝑖𝑜𝑛 + 𝑅𝑒𝑐𝑎𝑙𝑙 (2) (3) In rare cases a moderate Ki67 “background” staining may occur that nearly perfectly fits the cell nuclei, which results in a high F-score. Therefore, this (low intensity) signal would lead to an incorrectly high number of Ki67 positive cells which is, however, not plausible. To avoid using too low thresholds caused by this phenomenon we compute a plausibility measure, which combines the threshold level and the resulting relative number of Ki67 positive cells. Therefore, a border line is constructed were the relative threshold tRel (Eq. 4) and the resulting ratio of positive cells are equal (Fig. 2) and where Imax is the maximum immune signal occurring in the corresponding image. 𝑡𝑖 𝑡𝑟𝑒𝑙 = 𝑀𝑖𝑛( , 1) 𝐼𝑚𝑎𝑥 (4) All thresholds that result in a ratio of positive cells below this border line are considered plausible (plausibility=1) or not plausible otherwise (plausibility=1-[Distance to borderline]). Figure 2: Construction of the borderline between plausible and non-plausible thresholds by combining the threshold and the resulting ratio of positive cells. Finally, local maxima in the one-dimensional function F(i) are calculated and the corresponding thresholds are used as potential thresholds. The threshold ti is selected where the corresponding score (Eq. 5) is maximal. Klauschen et al. Computer assisted Ki67 scoring in the GeparTrio breast cancer study cohort 𝑆𝑐𝑜𝑟𝑒𝑖 = 𝐹(𝑖) ∗ 𝑃𝑙𝑎𝑢𝑠𝑖𝑏𝑖𝑙𝑖𝑡𝑦(𝑖) (5) Study population In the neoadjuvant GeparTrio study (NCT00544765) patients with untreated unilateral or bilateral primary breast cancer were enrolled after given written informed consent. Eligibility required tumor diagnosis by core biopsy, plus at least one of the following risk factors: age <36 years, clinical tumor size >5 cm, estrogen (ER) and progesterone (PR) receptor negativity, clinical axillary node involvement, or tumor grade 3 (2-5). An overview on the baseline clinicopathological parameters is given in (2) and Table S1. Patients received between 2002 and 2005 six to eight cycles of docetaxel, doxorubicin and cyclophosphamide (TAC) or a sequence of two cycles TAC followed by vinorelbine/capecitabine depending on clinical response after two cycles. At the time of the GeparTrio study there was not established central pathology for the GBG trials, therefore the local data was used for hormone receptor status (in line with the study protocol). For HER2 we have added data on some cases based on central testing, as HER2 testing was not fully established at the time the study was conducted. No patient received trastuzumab during neo- or adjuvant treatment. Postoperative radiotherapy and endocrine treatment was given according to national guidelines. Ethic committee approval was obtained for all centers participating in the clinical studies and from the institutional review board of the Charité hospital. Klauschen et al. Computer assisted Ki67 scoring in the GeparTrio breast cancer study cohort Supplementary table S1: Clinico-pathological data of the study cohort No. of samples Age group < 40 years ≥ 40 years Tumor type Ductal/other lobular missing Tumor grade G1-G2 G3 missing ER/PR Status (IHC) ER-/PRER+ and/or PR+ HER2 status (IHC/FISH) HER2 negative HER2 positive missing Tumor type Luminal/HER2Luminal/HER2+ HER2+/non-luminal Triple-negative missing Clinical tumor stage cT1-cT2 cT3-cT4 missing Clinical nodal status cN0 cN+ missing Ki67 0-15% 15·1-35% 35·1-100% Pathological response no pCR pCR n 1082 % 100% 170 912 15.7 84.3 855 144 83 79 13.3 7.7 649 378 55 60 34.9 5.1 353 729 32.6 67.4 779 238 65 72 22 6 547 143 95 232 65 50.6 13.2 8.8 21.4 6 723 355 4 66.8 32.8 0.4 492 579 11 45.5 53.5 1 328 383 371 30.3 35.4 34.3 911 171 84.2 15.8 Klauschen et al. Computer assisted Ki67 scoring in the GeparTrio breast cancer study cohort References 1. Ruifrok AC, Johnston DA. Quantification of histochemical staining by color deconvolution. Anal Quant Cytol Histol. 2001;23:291-9. 2. Huober J, von Minckwitz G, Denkert C, Tesch H, Weiss E, Zahm DM, et al. Effect of neoadjuvant anthracycline-taxane-based chemotherapy in different biological breast cancer phenotypes: overall results from the GeparTrio study. Breast Cancer Res Treat. 2010;124:133-40. 3. von Minckwitz G, Blohmer JU, Raab G, Lohr A, Gerber B, Heinrich G, et al. In vivo chemosensitivity-adapted preoperative chemotherapy in patients with early-stage breast cancer: the GEPARTRIO pilot study. Ann Oncol. 2005;16:56-63. 4. von Minckwitz G, Kummel S, Vogel P, Hanusch C, Eidtmann H, Hilfrich J, et al. Neoadjuvant vinorelbine-capecitabine versus docetaxel-doxorubicin-cyclophosphamide in early nonresponsive breast cancer: phase III randomized GeparTrio trial. J Natl Cancer Inst. 2008;100:542-51. 5. von Minckwitz G, Kummel S, Vogel P, Hanusch C, Eidtmann H, Hilfrich J, et al. Intensified neoadjuvant chemotherapy in early-responding breast cancer: phase III randomized GeparTrio study. J Natl Cancer Inst. 2008;100:552-62.