Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Diges&ve System University of Pavia • The Alimentary Canal is approximately 9m long and it’s divided for descrip&ve purposes into: 1. Oral Cavity 2. Pharynx 3. Oesophagus 4. Stomach 5. Small Intes&ne (Duodenum, Jejunum and Ileum) 6. Large Intes&ne (Caecum, Ascending Colon, Transverse Colon, descending Colon, Sigmoid Colon and Rectum) 7. Anal Canal 8. MALT 9. Diges&ve glands (liver, gallbladder, biliary tree, pancreas and paro&d, submandibular and sublingual glands). The Oral Cavity -‐It extends from the lips and ceecks externally to the Anterior Pillar of the fauces internally, where it con&nues with the oropharynx. -‐The Palate forms the roof of the mouth and separates the oral and nasal cavi&es. -‐The floor is formed by the mylohyoid muscle and mainly occupied by the tongue. -‐Lateral walls are defined by the cheecks and retromolar space. • The Oral Ves)bule is a slit like space between the lips and cheecks. Where the mucosa of the alveolus of the jaw is reflected onto the lips and cheecks, a solcus is formed, which is called fornix ves&buli. In the midline are the upper and Lower labial frenula and the Upper one is normally a[ached well below the alveolar crest. • The Oropharyngeal Isthmus lies between the So\ Palate and the Dorsum of the tongue and is bounded on both sides by the Palatoglossal Arches. Each palatoglossal arch runs downward , laterally and forward. Floor of the mouth It’s mainly formed, when the fauces are closed, by tongue that rest on this surface, which extends obliquely and downward which is know as free por&on of the floor of the mouth. Along the median line of the inferior triangle of the tongue, there is a mucosal fold semilunar shaped, which join the inferior surface of the tongue with the floor of the mouth, and it’s known as Frenulum Linguae. At the side of the frenulum, are present two small orifices, which are the opening of the Canal of Warthon or Submandibular Duct. Laterally and behind the frenulum can be found a group of orifices which rapresent the excretory ducts of the Sublingual Gland. Posterior part of the mouth The so\ palate is a muscular membraneus septum which con&nues dorsally the hard palate and within its inferior margins draws what is defindes as Isthmus of the Faucis. It’s able to contract and when it does so allows the air to freely pass from the nasopharynx to the oropharynx. When it’s pulled up interrupts the comunica&on between the two cavi&es (deglu&&on). Salivary Glands . Three main type of Salivary Glands in our body, the Paro&d Glands, the Submandibular and Sublingual glands. • They are tubuloacinar exocrine glands whose ducts open in the oral cavity. • They secrete mainly: Saliva, diges&ve enzymes, amylase, anµbial agents, immunoglobulin A, Lysozyme (LYZ, it damages bacterial cell walls by catalyzing hydrolysis) and Lactoferrin (LTF, glycoprotein, it provides an&bacterial ac&vity to human infants). • Approximately 0.5l of saliva daily uns&mulated and up to 1,5l if s&mulated. • The Paro&d secre&on is serous, whereas Submandibular Gland is seromucous and Sublingual secre&on is mainly mucous. Paro&d Glands •
•
•
•
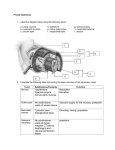
Each weights approximately 25g They are of inverted pyramidal form, yellowish in colour. Each is placed in a specific area known as the “Paro&d Lodge” The concave superior surface is related to the car&laginous part of the external acous&c meatus. • The superficial por&on is covered by the skin and superficial fascia (containing facial branches of great auricular nerve) • The anteromedial surface is embedded in the posterior border of the mandibular ramus • The posteromedial surface lies within the mastoid process, sternocleidomastoid, post belly of digastric and styloid process. • Structures within the Paro&d Glands: Ext Caro&d Artery, Retromandibular Vein (temporomaxillary vein, posterior facial vein), and Facial Nerve traverse and branch within the gland. -‐The paro&d is enclosed within a capsule, the Paro&d Capsule, deriving from the inves&ng layer of Deep Cervical Fascia. The Paro&d Duct is averagely 5 cm long. It passes horizontally across the Masseter, traverses the buccal fat pad and Buccinator and it opens in the oral cavity opposite to the upper second molar crown. The Submandibular Glands • Irregularly walnut shaped • Situated in the digastric triangle and it’s enclosed between two layers of cervical fascia • The submandibular duct (Wharton's duct, submaxillary duct), one of the salivary ducts, is usually 5 cm long, its wall is much thinner than that of the paro&d duct. It emerges behind the post border of mylohyoid and lies between the lingual and hypoglossal nerve before entering in the oral cavity Sublingual Glands • It weights approximately 4g and lies on the mylohyoid. • It has 8-‐20 excretory ducts • Obstruc&on of one of these ducts may result in a condi&on known as “ranula” a mucous cyst • Ducts of Rivinus and a larger sublingual duct, known as duct of Bartholin Sublingual Ducts The excretory ducts of the sublingual gland are from eight to twenty in number. Of the smaller sublingual ducts (ducts of Rivinus), some join the submandibular duct; others open separately into the mouth, on the elevated crest of mucous membrane (plica sublingualis), caused by the projec&on of the gland, on either side of the frenulum linguae. One or more join to form the major sublingual duct (larger sublingual duct, duct of Bartholin), which opens into the submandibular duct. Submandibular Duct The Wharton's duct begins by numerous branches from the deep surface of the gland, and runs forward between the mylohyoideus, hyoglossus, and genioglossus, then between the sublingual gland and the genioglossus, and opens by a narrow orifice on the summit of a small papilla at the side of the frenulum linguæ. It drains saliva from the submandibular glands and sublingual glands to the sublingual caruncle at the base of the tongue. Paro&d Duct The paro&d duct, also known as Stensen's duct passes through the buccal fat, buccopharyngeal fascia, and buccinator muscle then opens into the ves&bule of the mouth next to the maxillary second molar tooth. The buccinator acts as a valve that prevents infla&on of the duct during blowing. Running along with the duct superiorly is the transverse facial artery and upper buccal nerve; inferiorly is the lower buccal nerve. Pharynx • It’s a muscular half cylinder that links the oral and nasal cavi&es in the neck and to the larynx and oesophagus (at CVII) in the neck. • It’s subdivided into three region: Nasopharynx, Oropharynx and Laryngopharynx • Rela&ons: Anteriorly: posterior one/third of the tongue. Posteriorly: Retropharyngeal space. • Pharyngeal walls are formed by skeletal muscle (the Constrictor muscles) and fascia • They are divided in Superior, Middle and Inferior Constrictor muscle. Pharynx Salivary Glands • Superior Constrictors: They form the upper part of the pharyngeal cavity. Each is a[ached anteriorly to the pterygoid hamulus and pterygomandibular raphe. • They run out posteriorly and joins with its partner muscle from the other side at Pharyngeal Raphe. -‐ Middle Constrictor: A[ached to the lower aspect of the stylohyoid ligament and the lesser horn of the Hyoid bone. They fun out posteriorly and a[ach to the Pharyngeal raphe. The posterior part overlaps the middle constrictor. Inferior constrictor: A[ach to the oblique line of the Thyroid car&lage. Spread out posteriorly to a[ach to the pharyngeal raphe. The inferior fibers blend with and a[ach to the wall of the oesophagus • Longitudinal muscles: Named according to their origin. • Stylopharingeus: originates from the styloid process of the temporal bone and fan out on the deep surface of pharyngeal wall. (innervated by CN IX) • Salpingopharingeus: From the Inferior aspect of Pharyngotympanic tube and blends on the deep surface of Pharyngeal walls (innerva&on by vagus) • Palatopharyngeous: a[ached to the upper surface of the Pala&ne Aponeurosis, passes posteriorly and inferiorly to blend with the deep surface of the pharyngeal walls. (important landmark in finding Pala&ne tonsils) So\ palate muscle Musculus Uvulae: Arises from the post nasal spine of pala&ne bone and lies between the two laminae of the aponeurosis and inserts beneath the mucosa of the uvula. -‐Levator Veli pala&ne: it arises by a small tendon from a quadrilateral roughned space on the medial end of the inferior surface of the petrous part of the temporal bone. It crosses the medial end of the Pharyngotympanic tube. It elevates the posterior part of the so\ palate and pull it sliglthly backward. -‐Tensor Veli Pala&ni: It arises from the scaphoid fossa of the pterygoid process. It turns medially around the Pterygoid hamulus. Ac&ng togheter they &ght the So\ Palate. Ac&ng unilaterally, it pulls the so\ palate to one side. So\ palate pharynx PHARYNX : Nasopharynx,Oropharynx, Laringopharynx • Nasopharynx ranges from the posterior choanae &ll to the so\ palate and it’s con&nuous below with the oropharynx at the pharyngeal isthmus. • -‐ Presence of MALT with the adenoids • Pharyngotympanic Tube: It connects the Tympanic cavity to the nasopharynx and allows the passage of air between the two spaces to equalize the pressure. It’s 36mm long and descends anteromedially at an angle of approximately 45’. Oropharynx • It’s placed posterior to the oral cavity, inferior to the level of the so\ palate. • The palatoglossal muscles mark the boundary with the oral cavity. • The anterior wall presents the lingual and pala&ne tonsils • When holding a liquid or a solid in the oral cavity, the oropharyngeal isthmus is closed by a depression of the so\ palate togheter with the eleva&on of the back of the tongue. This allows to breath while chewing or manipula&ng material in the oral cavity. Laringopharynx • Laryngopharynx extends from the superior margin of the epiglops to the top of the oesophagus at CVII level. • Par&culari&es of innerva&on: Nasopharynx-‐sensory V2 • Oropharynx-‐sensory IX • Laryngopharynx-‐sensory X Oesophagus • It’s a muscular tube, typically 25cm long, which connects the pharynx with the stomach. • It begins in the neck at CVI • Descends slightly anterior to the Vertebral Coloumn trough the Superior and Posterior Medias&num and ends at the gastric orifice at T10. Cervical Oesophagus: It lies posteriorly to the trachea. It lies anteriorly to the vertebral coloumn. It lies medially in respect to the Common Caro&d Artery. Thoracic Oesophagus: It lies posteriorly to the trachea, right pulmonary artery, le\ subclavian artery, le\ main bronchus, diaphragm. It lies anteriorly to the vertebral column, azygos vein and thoracic duct. Abdominal Oesophagus: It’s 2 to 2,5 cm long. It lies le\ of the midline and enters the abdomen trough the oesophageal aperture at T10. -‐It lies posterior to the le\ lobe of the liver and it’s a[ached to the diaphragm by means of the Phreno-‐oesophageal ligament Sites of Constric&on 1) At the esophageal inlet, where the pharynx joins the esophagus, behind the cricoid car&lage (14–
16 cm from the incisor teeth). 2) Where its anterior surface is crossed by the aor&c arch and the le\ bronchus (25–27 cm from the incisor teeth). 3) Where it pierces the diaphragm (36–38 cm from the incisor teeth). Development of the Foregut In order to properly understand the dispositon of the abdominal organs within the cavity in which they are contained, we have to consider their embriological origin. In Abdominal region, the Foregut gives rise to the distal end of the oesophagus, the stomach, and the proximal duodenum. In addi&on it’s the only part of the gut tube which is suspended by both ventral and dorsal mesentery. A diver&culum from the anterior aspect of the foregut grows in the ventral mesentery and forms the Liver, gallbladder and Ventral part of the Pancreas. The dorsal part of the Pancreas develops from an outgrowth of foregut into the dorsal mesentery. Development of the Foregut The spleen develops in a region between the the body wall and the stomach. The developing stomach rotate clockwise and the associated mesentery (containing the spleen), moves to the le\ and greatly expands. At the same &me the duodenum and an appreciable part of the pancreas swing to the right and fuses with the body wall. The secondary fusion of duodenum, togheter with the massive growth of Liver’s Ventral Mesentery and the fusion of Superior Liver Surface with diaphragm, leads to the crea&on of a restricted opening (Omental Foramen) to the space enclosed by ballooned dorsal mesentery. The part of abdominal cavity enclosed by the expanded dorsal mesentery and posterior to the stomach is the Omental Bursa (lesser sac). Part of the dorsal mesentery that ini&ally form part of the Lesser Sac greatly enlarges in an inferior direc&on and fuse to form an apron like structure, the Greater Omentum. Development of Midgut • A small yolk sac projects anteriorly from the developing midgut into the umbilicus. • The two limbs of the midgut loop rotate counterclockwise around their combined central axis (Superior Mesenteric artery), and the part of the loop that becomes Caecum descends into the Inf Right aspect of the cavity. The Caecum remains intraperitoneal and the Ascending Colon fuses with the Body wall becoming secondary retroperitoneal. Development of Hindgut The distal 1/3 of the Transverse Colon, Descending Colon, Sigmoid Colon and Superior Part of the Rectum develop from the hindgut and swing to the le\ during embriological development. Topographically, the abdomen can be divided into right and le\ upper and right and le\ lower quadrants by ver&cal and horizontal lines through the umbilicus. Abdomen may also be divided into nine regions by two longitudinal lines (right and le\ midclavicular lines) and two transverse planes (subcostal and intertubercular planes). The regions are: right and le\ hypochondriac, right and le\ lumbar, right and le\ inguinal (or iliac), epigastric, umbilical and hypogastric. Surface Topography of the Abdomen Organs found in the epigastric region Diges6ve: Esophagus Stomach Liver Pancreas Small IntesCne Transverse Colon Endocrine: Right & LeH Adrenal Glands Pancreas Right & LeH Kidneys Excretory: Right & LeH Kidneys Right & LeH Ureters Lympha6c: Spleen Stomach • It’s the wider part of the alimentary canal and lies between the oesophagus and duodenum. • It’s placed in the upper abdomen, lying in the le\ hypocondric, epigastric and umbilical areas. • For descrip&ve porpouses, it’s divided into a fundus, body, pyloric antrum and pyloric canal. Stomach • The Fundus is dome shaped and projects above of the cardiac orifice to lie in contact with the dome of the diaphragm. It lies above the Cardiac Incisura to the Greater Curvature. The Body extends from the fundus to the Incisura angularis and the Pyloric Antrum, where it narrows to finish in the Pyloric Canal. Gastric Curvatures • Lesser Curvature: It extends between the Cardiac and Pyloric Orifices and forms the medial and posterosuperior border of the stomach. It descends from the medial side of the oesophagus, in front of the decussa&ng fibers of the right crus, curves downward and lies anteriorly to the Superior Border of the Pancreas. (the Lesser Omentum is a[ached to it). • Greater Curvature: It’s 4 to 5 &mes longer than the Lesser. It starts from Incisura Cardiaca and arches upward and posterolaterally and to the le\. Laterally, it gives a[achment to the Gastrosplenic Ligament and Splenorenal ligament and beyond this the Greater Omentum (containing gastrosplenic vessels). Gastric Surfaces • Anterior (superior) surface: It’s posterior to the costal margins and in contact with the diaphragm. The upper le\ part curves posterolaterally and is in contact with the gastric surface of the spleen. The right half of the anterior surface is related to the le\ Quadrate Lobe of the liver and the anterior abdominal wall. It’s en&rely covered by peritoneum.
Posterior (Inferior) Surface: It lies anteriorly to the le\ crus of the diaphragm, the le\ Phrenic vessels, le\ Suprarenal Gland, Superior Pole of the Le\ Kidney, Anterior Pancrea&c surface, splenic artery. The Greater Omentum and Transverse Mesocolon separates the stomach from duodeno-‐
jejunal flexure and Ileum. The proper posterior surface is covered by peritoneum, except at cardiac orifice. Cardiac Orifices • Cardiac Orifice and Gastro-‐Oesophageal junc)on: It’s typically situated to the le\ of the midline behind the 7th costal car&lage and it’s con&nuos with the abdominal oesophagus. • At rest there is a gastro-‐oesophageal pressure gradient due to the presensce of a nega&ve intrathoracic pressure and a posi&ve intrabdominal pressure. The major an&-‐oesophageal reflux mechanism is the tonic contrac&on of specialized smooth muscles of the wall of the lower oesophagus and the encircling fibers of the right diaphragma&c crus, which, togheter, exert a radial pressure. • Anyway, if a persisent laxity of the the cardias is present, several complica&ons may arise, including a condi&on known as Barret’s Oesophagus, which is a metaplasia of the distal oesophagus epithelium. • The cell lining the distal oesophagus, in reac&on to the presence of the of the gastric acids, modify themselves in order to protect from the acidic pH. • The Pylorus cons&tutes the communica&on sphincter with the proximal duodenum and the pyloric antrum of the stomach MICROSTRUCTURES LIPS TOOTH TONGUE OESOPHAGUS STOMACH, CARDIAC, PYLORIC FUNDIC GLANDS HUMAN ANATOMY: MICROSTRUCTURES CLASSIFICATION: LOCATION AND BOUNDARIES, FORM, FUNCTION, MICROSCOPIC STRUCTURE: A hollow organ is a visceral organ that is a hollow tube or pouch (as the stomach or intes&ne) or that includes a cavity (as of the heart or urinary bladder) The parenchyma are the func&onal parts of an organ in the body The stroma refers to the connec&ve, non-‐func&onal suppor&ve framework of an organ You always recognize a stroma (suppor&ng &ssue, formed by capsule and trabeculae) and parenchyma (func&onal &ssue). It is usually covered with a capsule of connec&ve &ssue that penetrates inside the body. We recognize overlapping layers of different &ssue Origin. Usually by the outer layer are: Tunica serosa (tunica adven66a in esophagus and rectum) Tunica muscularis Tunica submucosa Tunica mucosa ORAL CAVITY LIPS S = skin (no visible) SM = striated muscle sg = salivary gland SubM= submucosa bM = buccal mucosa S sg SM SubM bM Tooth anatomy Tooth anatomy The lingual papillae consist of a connec&ve &ssue core covered with a stra&fied squamous epithelium. On the basis of their appearance four types of papillae can be dis&nguished -‐ filiform, fungiform, circumvallate and foliate papillae SKELETAL MUSCLE OF TONGUE Filiform papillae are the smallest and most numerous papillae. By providing the tongue with a rough surface they aid in the manipula&on and processing of foods Fungiform papillae occur singly and are fairly evenly spaced between the filiform papillae. Their connec&ve &ssue core is richly vascularised. The epithelium is slightly thinner than on the remaining surface of the tongue Circumvallate papillae are the largest and least numerous papillae -‐ in humans there are between 8 and 12 of them. They occur in depressions of the surface of the tongue and are surrounded with a trench formed by the infolding of the epithelium. Taste buds are par&cularly numerous on the lateral surfaces of these papillae. The excretory ducts of serous glands open into the trenches surrounding the papillae ("rinsing glands" or glands of von Ebner Foliate papillae The word "foliate" means "leaflike" and in this case the reference is to the "leaves" of a book. The papillae themselves are flat-‐topped and have deep cle\s between them. The cle\s are lined with epithelium, and there are taste buds embedded in them. TASTE BUDS CLEFT submucosa TASTE BUDS