Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
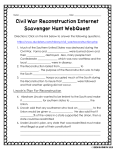
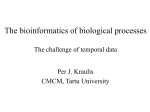
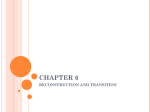
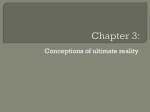
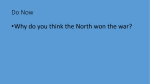
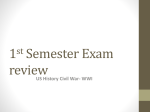
Multithreaded cardiac CT Marc Kachelrieß,a兲 Michael Knaup, and Willi A. Kalender Institute of Medical Physics, University of Erlangen, Nürnberg, Germany 共Received 23 December 2005; revised 29 April 2006; accepted for publication 1 May 2006; published 21 June 2006兲 Phase-correlated CT, as it is used for cardiac imaging, is the most popular and the most important but also the most demanding special CT application in the clinical routine, today. Basically, it fulfills the four-dimensional imaging task of depicting a quasiperiodically moving object at any desired motion phase with significantly reduced motion artifacts. Although image quality with phase-correlated reconstruction is far better than with standard reconstruction, there are motion artifacts remaining and improvements of temporal resolution are required. As a well-known alternative to simply decreasing rotation time, we consider a spiral cone-beam CT scanner that has G x-ray guns and detectors mounted. We call this a multisource or a multithreaded CT scanner. Aiming for improved temporal resolution the relative temporal resolution ˆ , which measures the fraction of a motion period that enters the image, is studied as a function of the motion rate 共heart rate兲 and the degree of scan overlap 共pitch value兲 for various configurations. The parameters to optimize are the number of threads G and the interthread parameters ⌬␣ and ⌬z, which are the angular and the longitudinal separation between adjacent threads, respectively. To demonstrate the improvements approximate image reconstruction of multithreaded raw data is performed by using a generalization of the extended parallel back projection cone-beam reconstruction algorithm 关Med. Phys. 31共6兲, 1623–1641 共2004兲兴 to the case of multithreaded CT. Reconstructions of a simulated cardiac motion phantom and of simulated semi-antropomorphic phantoms are presented for two and three threads and compared to the single-threaded case to demonstrate the potential of multithreaded cardiac CT. Patient data were acquired using a clinical double-threaded CT scanner to validate the theoretical results. The optimum angle ⌬␣ between the tubes is 90° for a doublethreaded system, and for triple-threaded scanners it is 60° or 120°. In all cases, ⌬z = 0 results as an optimum, which means that the threads should be mounted in the same transversal plane. However, the dependency of the temporal resolution on ⌬z is very weak and a longitudinal separation ⌬z ⫽ 0 would not deteriorate image quality. The mean temporal resolution achievable with an optimized multithreaded CT scanner is a factor of G better than the mean temporal resolution obtained with a single-threaded scanner. The standard reconstructions showed decreased cone-beam artifacts with multithreaded CT compared to the single-threaded case. Our phase-correlated reconstructions demonstrate that temporal resolution is significantly improved with multithreaded CT. The clinical patient data confirm our results. © 2006 American Association of Physicists in Medicine. 关DOI: 10.1118/1.2207236兴 Key words: cardiac imaging, multithreaded CT, cone-beam CT, spiral CT, dual source CT I. INTRODUCTION Cardiac computed tomography challenges the problem of imaging moving objects without showing significant motion artifacts. In general, CT requires at least 180° plus fan angle of projection data to perform image reconstruction. This implies that the intrinsic temporal resolution of a standard CT scan is in the order of trot / 2 or worse, where trot is the time needed for a full rotation of the scanner. With modern conebeam CT scanners it is possible to achieve trot / 2 = 165 ms, which is not sufficient to perfectly image the anatomical details of the human heart. Standard CT image reconstruction further makes use of all the data contributing to a given voxel and therefore exhibits a temporal resolution of about trot / p, where p is the spiral pitch value 共typical values lie in the range p 苸 关0.1, 1.5兴兲 and 1 / p quantifies the number of rotations that contribute to a single point in the object. 2435 Med. Phys. 33 „7…, July 2006 Special reconstruction algorithms can be designed to allow reducing the data to a single 180° segment to always come close to trot / 2.1 If the object is moving in a periodic fashion, it is further possible to use dedicated cardiac reconstruction algorithms that divide the required 180° into one, two, or more smaller segments and collect these smaller data segments from adjacent motion periods 共e.g., heart cycles兲. Thereby, the temporal resolution can be improved proportionally to the number of segments used. The alignment of these allowed data intervals 共be it one or several segments兲 to a desired motion phase generates images in which the object’s motion is frozen in the desired state. These basic concepts of phase-correlated CT imaging were first proposed and evaluated in Ref. 2, and since then they have been widely used in clinical CT.3–12 Although the use of multisegment reconstruction combined with very fast rotating scanners appears to provide 0094-2405/2006/33„7…/2435/13/$23.00 © 2006 Am. Assoc. Phys. Med. 2435 2436 Kachelrieß, Knaup, and Kalender: Multithreaded cardiac CT FIG. 1. Relative temporal resolution as a function of f Htrot for singlethreaded CT: analytical results for p = 1 / 4 共adapted from Ref. 2兲. The straight line from the origin to the top right corresponds to a single segment reconstruction. The zig-zag curve lying below is the achievable temporal resolution of multisegment algorithms. The parameter f denotes the fraction of a rotation required to perform image reconstruction 共in our case this is 180° plus fan angle divided by 360° which is close to 0.5兲. The gray bars at the top show the range 关50, 120兴 min−1 of typical heart rates for five different rotation time values. The resoncance peaks are annotated with small red 2 arrows. The two heart rates shown for the peak at f Htrot = 3 and at f Htrot = 1, correspond to a rotation time of 0.33 s; the 120 min−1 peak is considered the most severe resonance case among reasonable heart rates for the given rotation time. very high temporal resolution 共e.g., down to 55 ms if three segments are used and a rotation time of 330 ms is assumed兲, this is rarely the case since the ideal situation wherein the 180° interval can be divided into N intervals of size 180° / N only occurs for selected values of f Htrot where f H denotes the heart rate and trot the scanner rotation time. This complicated dependency of the relative temporal resolution , which is the fraction of a motion cycle that enters the image, as a function of the heart-rate-rotation-time product f Htrot was first derived in Ref. 3 and is demonstrated in Fig. 1 for a pitch value of p = 1 / 4. Obviously, low values of and therefore high temporal resolution can be achieved only for certain values of f Htrot. The average temporal resolution 共averaged over the range of typical heart rates兲 is far from ideal. Increasing rotation speed helps to improve the temporal resolution. However, due to increased centrifugal forces— they currently lie in the order of 20 g already—it appears difficult, but not impossible, to go significantly below the trot = 0.33 s that is available already. Increasing the number of simultaneously acquired slices, as it is today’s trend, will increase z-coverage but will not directly help to increase temporal resolution of phase-correlated CT imaging unless one uses very small pitch values. These, in turn, would yield to increased dose levels that can potentially be compensated to some extend by clever ECG-based tube current modulation. In addition to these concepts, improvements of temporal resolution can also be obtained by equipping a gantry with G x-ray guns and G detectors arrays that rotate together around the patient.13–16 We call such a scanner a multithreaded CT scanner. This avoids using manufacturer-specific terms such as “dual source CT,” for example. The term “thread” itself is Medical Physics, Vol. 33, No. 7, July 2006 2436 much older than CT and describes the spiral winding of a screw. 共There are single-threaded screws, but there are also double- or triple-threaded screws in use. The latter are used when large screw pitch values are required.兲 The term “thread” additionally takes into account the fact that the scanner does not only have multiple sources but also has multiple detector arrays. If these multiple sources are evenly distributed on a halfcircle, one may expect an improvement in temporal resolution by a factor of G since the 180° of data necessary for image reconstruction can be acquired G times faster than with a single-threaded scanner. Considering the complex relationship of temporal resolution, motion rate, and pitch value, as demonstrated in Fig. 1, the exact design parameters of a multithreaded cardiac CT scanner are far from obvious, however. The angle ⌬␣ between the multiple source detector arrays that maximizes the temporal resolution has not yet been determined. Further, it may be of advantage to separate the threads longitudinally by a certain amount ⌬z. Finally, it is not clear whether the improvements obtained are proportional to the number of threads. Regarding the literature, the first multiple-source CT systems that were realized attempted achieving fully fourdimensional imaging by completely sampling large object regions in the spatial and temporal domain with high spatial and temporal resolution.13–15 Cost and image quality issues did not allow commercialization of this system. Reference 16 also proposes a multithreaded CT scanner to improve temporal resolution, but no system was realized. Neither of these systems consider phase-correlated image reconstruction, no design optimizations regarding temporal resolution were carried out, and no reconstructions of clinical cardiac CT data were provided. Recently, a clinical dual-source dual-detector CT system became available that uses two threads, a z- and ␣-flying focal spot 共see one of17–19 for further details regarding the flying focal spot兲, and that reads out 32 detector rows per thread 共Definition, Siemens Medical Solutions, Forchheim, Germany兲.20 Each projection thus consists of 2 · 2 · 32 slices. Although we were not involved in the development of the Definition scanner, the paper intends to analyze the design parameters of such multithreaded CT systems with respect to image quality and temporal resolution and to quantify the improvements in view of multisegment image reconstruction. To do so, a simulation study was conducted that seeks the optimal configuration by varying the interthread parameters of the scanner for a wide range of pitch values p and heart-rate-rotation-time products f Htrot.21 For each point in this high-dimensional parameter space the relative temporal resolution is evaluated to determine the winning configurations for scanners with one, two, and three threads. To assess image quality in terms of noise, spatial resolution, and artifacts, the extended parallel backprojection 共EPBP兲 approximate cone-beam reconstruction algorithm11 was generalized to cope with multithreaded CT raw data. It accounts for the multiple threads by combining them into the weighting function during backprojection.22 Thereby, EPBP allows us to analyze the effects of multithreaded circular, 2437 Kachelrieß, Knaup, and Kalender: Multithreaded cardiac CT sequential 共multiple circles兲, and spiral CT for moderate and wide cone angles. Here, we focus on the spiral trajectory since this is the trajectory used in today’s cardiac CT scanners. It should be noted that adapting the weighting function of this Feldkamp-type algorithm is a rather simple task, and the purpose of this paper is not to propose a new image reconstruction algorithm. We rather intend comparing the performance of single-threaded CT to multithreaded CT for the same type of algorithm. The fact that the reconstruction algorithm used is Feldkamp-type and thus approximate may be considered being not adequate in view of the recent achievements in exact cone-beam image reconstruction. Supershort scan reconstruction algorithms or chord-based image reconstruction algorithms can achieve a temporal resolution that lies in the order of trot / 2.23–25 However these approaches fail as soon as the trajectory is interrupted, as it is particularly the case when one desires phase-correlated images or when one desires achieving a higher temporal resolution by using multiple data segments. The only way to achieve an uninterrupted spiral trajectory is to mechanically align the longitudinal detector offset ⌬z and the angular detector offset ⌬␣ between the threads such that both focal spots actually follow one and the same spiral trajectory. This, however, would fix the pitch value to p = ⌬␣ / ⌬z and would not allow us to adapt the pitch to the heart rate as it is required to achieve full phase selectivity. We consider the possibility to vary either ⌬␣ or ⌬z or both as a function of the patient’s heart rate as being impractical due to technical reasons. Using a rather large number of sources, say G = 10, would allow us to perform cardiac scans with a fixed pitch value, and could potentially overcome this problem of patient-specific scanner alignment. However, this scenario is considered impractical due to very high costs. In all these cases that achieve uninterrupted trajectories, even if they appear impractical today, exact image reconstruction is rather easy: the multithreaded data can be reduced by simple projection weighting to a single spiral data set and existing exact reconstruction algorithms would do the rest. For these reasons, neither multisegment phase-correlated image reconstruction nor multithreaded single- or multisegment image reconstruction is possible in practice with today’s exact algorithms and today’s scanners. A trivial exception is given by two-dimensional image reconstructions of circular scans. Here, one simply collects the interrupted data segments—this may be realized by appropriately weighting the raw data—until the data are sufficient to perform image reconstruction.26 Since our paper deals with threedimensional spiral cone-beam data the choice of a state-ofthe-art approximate cone-beam algorithm such as the EPBP algorithm is well justified. Other interesting applications of G-threaded CT besides cardiac imaging are not part of this paper. Nevertheless, some potential applications that are highly promising and that may be of significant interest in the near future are listed below. • Motion detection and kymogram processing:27 The siMedical Physics, Vol. 33, No. 7, July 2006 2437 multaneous acquisition of two or more projections of an object allows one to determine the object’s position. This can be used to support phase-correlated imaging with the synchronization information.28 • Dual energy CT:29–32 Using different tube voltages Ug for each thread’s tube allows one to decompose the raw data into two base functions, e.g., into the materials water and bone or into the contributions stemming from a photo effect or Compton effect. • Scatter estimation: One thread may be used to measure scatter information. This may be done by using beamstops. Prior to image reconstruction the missing data can be replaced by another thread’s data. • High resolution imaging:12 One thread may have a high resolution detector at the expense of a reduced field of measurement. The high resolution data are truncated but can be easily extended using another thread’s data that runs a low-dose acquisition. Needless to say, the reconstructions themselves are of high resolution only in the reduced field of measurement. II. MATERIALS AND METHODS A. Geometry We assume the scanner to have G tubes mounted on one pivot bearing that rotates with constant angular velocity, and we assume to have a table that is translated through the rotating gantry with constant velocity parallel to the gantry’s rotation axis. The source positions as a function of time t are defined as 冢 Rg sin共t + ␣g兲 sg共t兲 = − Rg cos共t + ␣g兲 pt + zg 冣 with g = 1 , . . . , G. To simplify our further considerations we rescaled the temporal axis 共t axis兲 to obtain a rotation time of trot = 2, and we rescaled the longitudinal axis 共z axis兲 such that the detector’s longitudinal extend is L = 2. The table increment per rotation is given as d = 2 p, from which we see that p = d / L is the spiral pitch value. Rg is the distance of source g to the isocenter. The possibility of chosing different values of Rg for each thread will not play a role for us since we assume the temporal information to be associated with the central ray. Thus, we may safely assume Rg = 1. Rescaling of the temporal and longitudinal axes and of the distance of the focal spot to the isocenter to physically meaningful units is implicitly done during image reconstruction. B. Data sufficiency During our considerations regarding temporal resolution, we will neglect the cone and fan angle of the rays, for convenience. This approximation helps to obtain manageable equations and relations and to carry out analytic manipulations. Our implementation of the generalized multithreaded EPBP reconstruction algorithm, that handles all data suffi- 2438 Kachelrieß, Knaup, and Kalender: Multithreaded cardiac CT ciency considerations and weighting manipulations in a numerical way, finally accounts for the correct ray geometry, which in turn implies that the allowed data ranges and the applied weight functions are actually voxel dependent 共see Ref. 11兲. A z-position zR is illuminated during t 苸 T = 艛 Tg with Tg = 共关− , 兴 + zR − zg兲/p. g The projection angles ␣ = t + ␣g that are covered during that illumination are Std ␣ 苸 AStd = 艛 AStd g with Ag = Tg + ␣g . s Standard image reconstruction at zR can be performed 共with an approximate cone-beam algorithm兲 when AStd covers an angular range of 180° or more. Here, we are interested in phase-correlated image reconstruction and have a set of synchronization points ts available, with ts ⬍ ts+1. These synchronization points may correspond to the R-peaks of the patient’s ECG signal, to the K-peaks of a patient’s kymogram, to any other suitable motion synchronization signal or they may correspond to shifted versions of these signals. Attached to these sync peaks are the allowed data ranges or data segments that are required for reconstruction. The union of all these segments 冉 冉冉 冊 S共兲 = 艛 ts + 关ts−1 − ts,ts+1 − ts兴 s = 艛 ts 1 − s 2 冊 冊 + 关ts−1,ts+1兴 2 2 is the set of time stamps that may enter the reconstruction. The variable 苸 关0 , 1兴 is the relative temporal resolution parameter. It is relative since it measures the width of each interval relative to the distance of adjacent sync peaks. Thereby, is the fraction of the motion cycle that enters the image. Consequently, the relative temporal resolution parameter is a better measure for image quality than an absolute temporal resolution measure where image quality would further depend on the motion rate of the object. Note that for = 1, the intervals touch at the midpoints 1 共t 2 s + ts+1兲 and we obtain S共1兲 = R. Thus, = 1 allows us to mimic a standard image reconstruction situation where in all data are allowed to enter reconstruction. Given a sufficiently large , the angular contribution of thread g to the desired z position is Tg 艚 S共兲 + ␣g, and combining the view angles of all G threads then results in CI ACI = 艛 ACI g with Ag = Tg 艚 S共兲 + ␣g . 2438 艛 共ACI + k兲 = R k is demanded Our implementation of cardiac image reconstruction iteratively determines the minimal possible that still ensures 180°-complete data. For each z position, the code goes through all the interval calculus and determines whether the resulting set is 180°-complete or not. This is done for all in the range from zero to one and the minimum possible is chosen. To speed up the procedure, the are selected using a binary search divide and conquer strategy. Basically, our code corresponds to a function min = f共兵␣g其 , 兵zg其 , 兵ts其 , zR兲. An analytic solution to determining min is not known, to the best of our knowledge. C. Projection weighting Multithreaded image reconstruction requires to generalize the projection weighting to account for contributions from multiple threads. To derive those thread- and projectiondependent normalized weights ŵg共␣兲 let be fixed and large enough such that ACI共兲 is 180°-complete. Thread g contributes the angles ACI g = Tg 艚 S共兲 + ␣g, which is a finite union of disjunct intervals ACI g 共兲 = 艛 共ag + bg关− 1,1兴兲. We now define multitriangular weight functions w g共 ␣ 兲 = 兺 ⌳ 冉 冊 ␣ − ␣ g , b g where ⌳共·兲 is a triangle function of area and height 1. In general, ⌳ can be replaced by any kind of weight function such as a Gaussian function, for example, as long as the support of the weight function covers ACI g , i.e., as long as . supp wg 傶 ACI g We further define the normalization ŵg共␣兲 = w g共 ␣ 兲 w ␥共 ␣ + k 兲 兺 k␥ , which exists since the denominator cannot become zero 共remember that ACI is 180°-complete兲. We achieved ŵg共␣ + k兲 = 1 and 兺 兺 kg g 冕 d␣ŵg共␣兲 = , g Here, CI stands for cardiac interpolation which is also known as multiphase or multisegment image reconstruction and includes single-segment or partial scan algorithms as a special case. We use the superscript CI to distinguish from standard image reconstruction. The value of must be chosen large enough to ensure ACI to be 180°-complete; i.e., Medical Physics, Vol. 33, No. 7, July 2006 which implies proper normalization for approximate conebeam image reconstruction of Feldkamp type. This means that each thread must be weighted by its normalized weight function ŵg共␣兲 before a slice at zR can be reconstructed. Weighting can also be done in temporal domain using w̃g共t兲 = ŵg共␣ − ␣g兲. 2439 Kachelrieß, Knaup, and Kalender: Multithreaded cardiac CT D. Relative temporal resolution To determine the relative temporal resolution ˆ that will, in general, differ from the relative temporal resolution parameter , one must compute the full width at half maximum of the phase sensitivity profile 共PSP兲. The PSP, that was proposed in Ref. 3, quantifies the contribution of each motion phase to the final image. It is defined as the histogram of cardiac phases c共t兲 weighted by the normalized projection weights w̃g共t兲 as follows: PSP共c兲 = 冕 • From the projection weights obtained so far, compute the PSP and therefrom the relative temporal resolution ˆ according to Sec. II D. The optimal interthread parameters ⌬␣ and ⌬z are found by averaging ˆ 共p , f Htrot , G , ⌬␣ , ⌬z兲 over the region 0 ⬍ p 艋 f Htrot ⬍ 1.2 and numerically seeking for those interthread parameters that minimize this mean temporal resolution value. dt ␦关c共t兲 − c兴 兺 w̃g共t兲, g where the cardiac phase c共t兲 苸 关0 , 1兲 is given as c共t兲 = 2439 t − ts , ts+1 − ts and s is chosen such that ts 艋 t ⬍ ts+1. The full width at halfmaximum ˆ of the PSP is our measure of temporal resolution: PSP共0兲 / 2 = PSP共ˆ / 2兲. III. STUDIES A. Geometry optimization Our aim is to find a configuration that optimizes temporal resolution over a wide range of heart rates as a function of the multithreaded scanner geometry. For this we fix G, vary ␣g, and zg, and regard the achievable temporal resolution over a wide range of pitch values p and heart-rate–rotationtime product values f Htrot. Note that the latter must obey p 艋 f Htrot to ensure full phase selectivity throughout the complete volume.3 To reduce the dimensionality of the parameter space, equidistant sync points ts = s⌬t are assumed. Note that ⌬t / 2 is the ratio of the duration 1 / f H of one heart beat to the duration trot of one gantry rotation. Thereby, f Htrot = 2 / ⌬t. We will further restrict our considerations to the cases G = 1, G = 2, and G = 3, which correspond to a standard, a double-threaded, and a triple-treaded spiral cone-beam CT scan, respectively. Equidistant interthread parameter sampling is assumed: ␣g = g⌬␣ and zg = g⌬z. Now, ˆ = ˆ 共p , f Htrot , G , ⌬␣ , ⌬z兲. Note that the computation of ˆ must be done numerically since neither the normalization of the weighting functions nor the determination of the full width at half-maximum of the phase sensitivity profile can be analytically handled in a convenient way. The steps carried out numerically to determine ˆ as a function of the configuration parameters are itemized in the following: • For a given parameter set 共heart rate rotation time product, interthread angle, interthread shift, pitch, etc.兲 find the minimum relative temporal resolution parameter that still allows for data completeness according to Sec. II B. • Use this value to generate the projection weights according to Sec. II C. Medical Physics, Vol. 33, No. 7, July 2006 B. Raw data simulation, acquisition, and reconstruction Spiral cone-beam CT raw data were simulated using a dedicated x-ray simulation tool 共ImpactSIM, VAMP GmbH, Erlangen, Germany兲. The software simulates the raw data by analytically computing line integrals through mathematically defined constructive solid geometry objects. The possibility to add scatter, to account for beam polychromacity and for other physical effects was not used. The scanner geometry was chosen corresponding to a medical state-of-the-art double-threaded spiral cone-beam CT scanner 共Definition, Siemens Medical Solutions, Forchheim, Germany兲: 1160 projections per rotation, 672 channels per slice, RF = 570 mm distance focal spot to isocenter and RFD = 1040 distance focal spot to detector. The collimated slice thickness at isocenter was chosen as S = 0.6 mm. The rotation time was set to trot = 0.33 s. Except for the first thorax phantom case, we simulated wide cone angle spiral CT scanners with M = 256 slices per thread. The use of such a wide cone angle helps provoking cone-beam artifacts far better than with today’s 64-slice scanners. Up to three threads are considered where the interthread parameters are set to ⌬z = 0 and to ⌬␣ = 0, ⌬␣ = / 2 and ⌬␣ = 2 / 3 for G = 1, G = 2 and G = 3, respectively. Thereby, the total number of simultaneously acquired slices ranges up to 3 · 256. Our simulations of spiral raw data include the pitch values p = 0.25, p = 1.5, p = 2, and p = 3. For phase-correlated reconstructions the only pitch suitable is p = 0.25, larger values would violate p 艋 f Htrot. Phantom definitions were taken from the phantom data base at www.imp.uni-erlangen.de/phantoms except for the cardiac motion phantom, which is defined in Ref. 3. A 2 ⫻ 2 subsampling was simulated for the focal spot and for the detector; integration time was simulated by subsampling the angular direction with two samples. Simulations were restricted to monochromatic beams and scatter was switched off to avoid introducing nonlinearities. Heart rates ranging from 60 to 120 beats per minute were simulated and evaluated. For convenience, we present images corresponding to the two heart rates 80 and 120 min−1. These were found to be representative with respect to their artifact behavior. The 120 min−1 has the further advantage of corresponding to a resonance case 共cf. Fig. 1兲 and therefore corresponds to a rather difficult imaging situation. The simu- 2440 Kachelrieß, Knaup, and Kalender: Multithreaded cardiac CT 2440 FIG. 2. The dual-source CT scanner available to us provides one detector that covers the full 50 cm FOM and one detector that only covers a 25 cm FOM. The data of the first thread are used to fill in the truncated regions of the second thread. FIG. 3. Winning configurations for G = 1, 2, and 3. lated motion function 共required for the cardiac motion phantom兲 consists of a 20% rest period followed by an 80% period of sinusoidal motion with an amplitude of ±5 mm.3 The use of multiple threads requires to generalize the definition of the effective mAs value 共effective tube current time product兲 as follows: 共I0t兲eff = I0trot , p/G where I0 stands for the tube current and trot is the rotation time. All our simulations were performed with the same effective mAs value to decouple patient dose from the parameters p and G. The effective tube current was empirically chosen to obtain about 10 HU pixel noise in a 20 cm water phantom. For a standard reconstruction we then expect constant image noise regardless of the pitch value and regardless of the number of threads used. Note that scatter effects, that are not objective of this paper and that are not switched on during our simulations, may slightly impair this expectation. Quantum noise was simulated by taking the simulated line integrals, undoing the log, adding Poisson noise, and taking the log again. The number of primary quanta required to simulate Poisson noise was set proportional to I0. To assess image noise, reconstructions of a simulated 20 cm cylindrical water phantom were done with the same parameters as the thorax phantom and the cardiac motion phantom. The reconstruction was modified to carry out an error propagation of the variances of the raw data values into the image. The square root of the images obtained are socalled sigma images whose pixel content quantifies the standard deviation of the image pixel noise. Image noise was computed as the mean of the pixel values in a cuboid region of interest that extends over all reconstructed slices and over an transaxial area of 1 cm by 1 cm centered at x = 30 mm and y = 0 of these sigma images. The pixel noise measured in these reconstructions of the water phantom is displayed in the fourth quadrant of the thorax phantom images. Spatial in-plane and z-resolution values ⌬ and ⌬z are assessed by determining the full width at half-maximum of the point spread function and of the slice sensitivity profile, respectively. These profiles are given by reconstructions of a delta object. Thereby, image noise and spatial resolution are measured in the same way as we did for the single-thread version of EPBP.11 The quality factor FIG. 4. Plots of temporal resolution ˆ for single-, double-, and triplethreaded scanners as a function of f Htrot and p. Images are windowed to the range 关0, 1兴. The ROI is defined by p 艋 f Htrot and is located in the lower right triangle of each plot 共indicated by the dashed line兲. ROI results are given in the form 共Min, Mean± StdDeV, Max兲. All temporal resolution values are given in %. Medical Physics, Vol. 33, No. 7, July 2006 2441 Kachelrieß, Knaup, and Kalender: Multithreaded cardiac CT TABLE I. The mean relative temporal resolution 共in %兲 measured in the ROI p 艋 f Htrot for various values of ⌬␣ and ⌬z. ⌬z / L = 0% ⌬z / L = 20% ⌬z / L = 40% ⌬z / L = 60% ⌬z / L = 80% ⌬z / L = 100% Q2 ⬀ ⌬␣ = 30° ⌬␣ = 60° ⌬␣ = 90° ⌬␣ = 120° ⌬␣ = 150° 25 26 26 25 25 25 20 20 21 21 21 21 16 16 17 17 18 18 20 20 21 21 21 21 25 25 25 25 25 25 1 ⌬ ⌬z2 3 is used as the figure of merit to quantitatively compare the reconstructions. In contrast to Ref. 11, the pitch value does not explicitly appear in the definition of Q. Here, we rather use the concept of the effective mAs value to compensate for the scan overlap parameter p. The constant of proportionality is chosen to normalize the single-threaded 256-slice reconstructions with p = 0.25 to Q = 1. We further present patient data that have been acquired with the dual-source spiral cone-beam CT scanner Definition 2441 共Siemens Medical Solutions, Forchheim, Germany兲 that simultaneously acquires 2 · 32 slices per thread. The number of projections per rotation was N360 = 1536. To accommodate both detectors 共90° interthread angle兲 in the gantry housing one of the detector arrays is of smaller size 共352 channels per detector row兲 and covers only a 25 cm field of measurement 共FOM兲 as shown in Fig. 2. Thereby, this so-called B-detector suffers from data truncation. The missing data, however, can be easily filled in using the values acquired by the large A-detector. These extrapolated portions of the B-detector are used for data filtering only. Backprojection itself respects the small FOM and the final clinical CT image is a weighted combination of a large A-image and a small B-image. Obviously, improvements in temporal resolution due to the use of two source-detector systems can be obtained only within the small 25 cm FOM and, consequently, care must be taken to position the patient’s heart close to the center of rotation. The simulated and measured raw data were reconstructed using the generalized EPBP algorithm22 that is closely related to the single-thread version of EPBP.11 The standard reconstruction EPBPSTD and the phase-correlated algorithm EPBPCI 共“cardio interpolation”兲 were implemented on a standard PC. FIG. 5. Data of scanners with one, two and three threads using an 共approximately兲 constant number of simultaneously acquired slices and constant scan speed. The left column further demonstrates the decomposition of the G = 3 image, whereby the window level and width had to be adjusted to −666 HU and about 700 HU, respectively, to show all effects. Ticks indicate the location of the axial slices and the MPRs 共0 HU/ 300 HU兲. Medical Physics, Vol. 33, No. 7, July 2006 2442 Kachelrieß, Knaup, and Kalender: Multithreaded cardiac CT 2442 FIG. 6. Spiral scan of the thorax phantom with M = 256 slices per thread. Two selected pitch values and one to three threads are shown. Ticks indicate the location of the axial slices and the MPRs 共0 HU/ 300 HU兲. IV. RESULTS A. Geometry optimization The optimum scanner configurations that were found by minimizing ˆ as a function of ⌬␣ and ⌬z for a wide range of heart rates and pitch values are illustrated in Fig. 3. As expected, ⌬␣ = / G and ⌬z = 0 should be chosen to gain the optimal temporal resolution. Of course, symmetry allows us to choose ⌬␣ = 2 / 3 in place of / 3 for G = 3. Plots that show ˆ as a function of f Htrot and p for the three winning configurations are given in Fig. 4. Here, the ROI p 艋 f Htrot is indicated as well. The figure nicely illustrates the well-known resonance phenomenon that occurs when the value of f Htrot is close to a fraction consisting of small integers 共e.g., 1 / 2 or 2 / 3兲.3 A very intuitive resonance case is given at f Htrot = 1, when the patient’s heart rate is equal to the scanner’s rotation frequency. Then, the angular range captured remains the same from heart beat to heart beat and the multiphase strategy cannot benefit from using data of several heart cycles. Note that the plot of Fig. 1 corresponds to a horizontal profile at p = 1 / 4 through the G = 1 subimage of Fig. 4. In view of the resonance phenomenon, it is interesting to realize that the minimum, the maximum, the mean and the Medical Physics, Vol. 33, No. 7, July 2006 standard deviation of the ROI 共see Fig. 4兲 are approximately proportional to 1 / G. This implies that having a scanner with G threads will have a G-fold performance compared to a single-threaded CT. Note that this finding also includes the variation, which is the ROI’s standard deviation, of the temporal resolution as a function of the heart rate, this variation is also reduced proportional to G, and imaging becomes less dependent on the heart rate for multithreaded scanners. For completeness, Table I gives the temporal resolution also for some nonwinning configurations for the case G = 2. The interthread angle ⌬␣ is shown ranging from 30° to 150° in 30° steps. The longitudinal distance between ⌬z the source-detector systems ranges from 0% to 100% of the longitudinal detector extend L in steps of 20%. Looking for the lowest possible temporal resolution values we find that it is important to choose ⌬␣ correctly, but it is less important to set ⌬z correctly. B. Raw data simulation, acquisition, and reconstruction In the following thorax phantom figures, we will display the planes x = 0 mm 共sagittal兲, y = 0 mm 共coronal兲, and z = 144 mm 共axial兲 with cubic voxels of 1 mm size. The re- 2443 Kachelrieß, Knaup, and Kalender: Multithreaded cardiac CT 2443 FIG. 7. Phase-correlated EPBPCI reconstructions of the thorax phantom scanned with 256 slices at p = 0.25 for G = 1, 2, and 3. Two different heart rates are assumed during reconstruction. Ticks indicate the location of the axial slices and the MPRs 共0 HU/ 300 HU兲. maining fourth quadrant is used to display the image noise 共standard deviation in HU兲. The gray scale window center and width lie at 0 and 300 HU, respectively. For the reconstructed cardio motion phantom, we display the cross sections x = 50 mm, y = 10 mm, and z = 0 mm with cubic 0.5 mm voxels at a window center of 0 HU and a window width of 500 HU. Our first series of thorax phantom reconstructions keeps the number of simultaneously acquired slices G · M constant 共at about 128兲, while the number of threads G varies from 1 to 3. The table increment per rotation d is also kept constant to allow for a fair comparison of single-, double-, and triplethreaded scanners. To achieve this constant scan speed the pitch value has to increase from p = 1.0 for the singlethreaded scanner up to p = 3.0 for the triple-threaded scanner. Note that such large pitch values are possible only with multithreaded scanners. The right column of Fig. 5 shows the corresponding reconstructed images. Apparently, high image quality is achieved in all three cases. However, although the cone angle decreases with in creasing G, we find that the artifacts emerging from the spine—these are visible in the coronal and sagittal reformations only—slightly increase with inMedical Physics, Vol. 33, No. 7, July 2006 creasing G. This is due to the increased pitch value and is confirmed by comparing the small and large pitch images shown in Fig. 6. To demonstrate the decomposition of the G = 3 image into contributions of each thread, the left colum of Fig. 5 shows the images produced by g = 1, g = 2, and g = 3. The sum of these three volumes equals the G = 3 volume with M = 42 slices per thread and a pitch value of 3.0 on the bottom right of the same figure. Figure 6 shows standard reconstructions of the thorax phantom scanned with a single-threaded 256-slice scanner, a double-threaded 2 · 256-slice scanner, and a triple-threaded 3 · 256-slice scanner 共256 slices per thread always兲. The pitch values were chosen as p = 0.25 to correspond to a typical pitch value for cardiac CT at 0.33 s rotation time and as p = 1.5 which is the maximum pitch for single-threaded scanners. The sagittal and coronal reformations show streak-like cone-beam artifacts emerging from the spine. These artifacts decrease with decreasing pitch—there are fewer artifacts for p = 0.25 than there are for p = 1.5—and the artifacts decrease with an increasing number of threads. Both observations can be understood as some kind of averaging effect. For smaller 2444 Kachelrieß, Knaup, and Kalender: Multithreaded cardiac CT 2444 FIG. 8. Cardiac motion phantom at 80 min−1 with up to three threads. Reconstructions were conducted with EPBPSTD and EPBPCI at the slow, medium, and high motion phase of the motion phantom 共0 HU/ 500 HU兲. pitch values, there are more source positions contributing to each voxel and hence the artifacts average away. For more threads, the focus position of the second and third thread differ from the first thread and hence the direction of the cone-beam artifact does differ as well 共c.f. Fig. 5兲. Note that the thorax phantom is a mathematical phantom whose structures are designed to provoke artifacts; measured data of phantoms or patients would show far fewer artifacts, if any. Although the thorax phantom is not a motion phantom, it is interesting to regard phase-correlated reconstructions thereof. Therefore, we simply feed simulated ECG signals to the phase-correlated reconstruction algorithm EPBPCI. The reconstructions for two representative heart rates are given in Fig. 7. The phase-correlated reconstruction uses only a subset of the available raw data. Hence, noise increases and the cone-beam artifacts are slightly increased compared to the standard reconstructions of Fig. 6. Note that the low values of the quality index Q of Fig. 7 indicate a higher temporal resolution rather than low image quality; Q is influenced mainly by the large increase in image noise. Predominantly in the 120 min−1 reconstructions, one also finds artifacts emerging from the lungs 共small black ellipsoids in the axial images兲. In contrast to the EPBPSTD reMedical Physics, Vol. 33, No. 7, July 2006 constructions, we do not necessarily observe a reduction of cone-beam artifacts with increasing G with EPBPCI. Especially for the high heart rate, cone-beam artifacts seem not to decrease in the axial images. Since image noise also increases with G, we can conclude that the additional threads are used to improve temporal resolution instead of reducing cone-beam artifacts. However, the temporal resolution improvement with increasing G is less for the 80 min−1 case than for the 120 min−1 case. This is due to the fact that the high heart rate corresponds to a resonance case 共cf. Fig. 1兲 whose temporal resolution can only be improved by increasing the number of sources. The lower heart rate is offresonance and therefore also profits from multisegment reconstruction. Obviously, the value of multiple x-ray guns is shared among cone-beam artifact reduction and increased temporal resolution in a complex, heart rate-dependent and reconstruction phase-dependent way. To directly visualize the achievable temporal resolution one has to regard reconstructions of the cardiac motion phantom. Figures 8 and 9 show cases for 80 and 120 min−1 reconstructed with EPBPSTD 共not phase correlated兲 and with the cardio reconstruction EPBPCI. The reconstruction window was centered at the slow, the medium and the high 2445 Kachelrieß, Knaup, and Kalender: Multithreaded cardiac CT 2445 FIG. 9. Cardiac motion phantom at 120 min−1 with up to three threads. The allowed data ranges were aligned with the slow, medium, and high motion phase of the motion phantom for the phase-correlated reconstructions 共0 HU/ 500 HU兲. motion phase of the cardiac motion phantom. These motion phases correspond to 0%, 30% and 50% of S-S 共simulated synchronization points兲.3 The standard reconstructions show the expected significant blurring of the moving cylinders 共second left column of calcifications兲 and of the moving spheres 共rightmost two columns of calcifications兲. This blurring is nicely visible in the multiplanar reformations as well. Regarding the reconstructions of the slow motion phase we find optimal image quality in all cases except for the G = 1 reconstruction of the 120 min−1 patient. The calcifications of the high heart rate patients, however, cannot always be perfectly captured in the medium motion phase. Only the double-and the triple-threaded scanner have a temporal resolution high enough to freeze the medium motion phase at 120 beats per minute. Regarding the high motion phase where the sinusoidal motion function runs through its zero point 共at 50% of S-S兲 we find motion artifacts for G = 1 and G = 2 in the 80 min−1 reconstruction, whereas the G = 3 scanner behaves almost ideally. The high motion phase images of the 120 min−1 data show motion artifacts in all cases. Nevertheless, these are nearly removed with increased G. Medical Physics, Vol. 33, No. 7, July 2006 Figure 10 shows reconstructions of patient data acquired with the Definition scanner. As already detailed in Sec. III B, the data of the small detector 共B-detector兲 had to be extended to the full FOM by using data of the large detector 共Adetector兲, and these extended values were used for convolution only but not for backprojection. While the standard reconstruction, which is not phase-correlated, shows significant blurring due to the heart motion the two cardiac reconstructions with G = 1 and G = 2 clearly depict the anatomy. Apart from the noise reduction—which simply comes from artificially switching on and off the second thread and is no property of dual source CT—the differences between one and two threads are subtle for this patient 共arrows兲. For example, the blurring artifacts of the left ventricle that is filled with contrast agent are greatly reduced when switching from the single source reconstruction to the dual source reconstruction. V. DISCUSSION AND CONCLUSIONS To optimize the temporal resolution of phase-correlated cardiac CT, we analyzed the theoretical performance of G-threaded spiral cardiac CT and determined the optimal 2446 Kachelrieß, Knaup, and Kalender: Multithreaded cardiac CT 2446 FIG. 10. Patient data acquired with pitch p = 0.4 and a rotation time of trot = 0.33 s. The heart rate was f H = 90 min−1. The left image is a standard reconstruction using both threads, the middle and right images are phasecorrelated cardio reconstructions centered at 50% of R-R using one and two threads, respectively. The temporal resolutions are 165 and 83 ms, respectively. The three rows show axial, coronal, and sagittal displays of the volume 共100 HU/ 800 HU兲. geometric design parameters of respective scanners. The results turned out to correspond to the natural choice: 180° / G interthread angle and zero longitudinal interthread distance are optimal. Whereas the correct interthread and angle ⌬␣ is crucial for temporal resolution we found negligible effects for the longitudinal distance ⌬z. Temporal resolution and thus image quality improves proportional to the number of available threads for all combinations of heart rate, reconstruction phase, rotation time, and pitch value. The improvements in temporal resolution do not only refer to the temporal resolution averaged over a range of typical heart rates, but they also apply to the variation of the temporal resolution as a function of f Htrot. Especially resonance cases that cannot be improved with single-threaded scanners are significantly reduced with multithreaded CT. Standard and phase-correlated EPBP reconstructions of the simulated thorax and the simulated cardiac motion phantom and reconstructions of patient data prove that image quality becomes better with increasing G. Less motion artifacts and fewer cone-beam artifacts are observed with double- or triple-threaded scanners given that they are compared at the same pitch value. The improved temporal resolution and the reduction of motion artifacts can be directly attributed to the G-fold temporal sampling. Since the rotation angle required to obtain complete data is 180° / G 共neglecting the fan angle兲, it is worth noting that a temporal resolution of trot / 2G can be achieved also in those cases where no phase correlation is possible or desired, given that the image reconstruction algorithm uses only the minimal data necessary. When increasing the pitch proportionally to the number of threads, it was shown that the cone-beam artifacts slightly increase 共Fig. 5兲. However, we observed a potential reduction of cone-beam artifacts with multiple threads and apMedical Physics, Vol. 33, No. 7, July 2006 proximate Feldkamp-type image reconstruction at constant pitch 共Fig. 6兲. This improvement, that is apparent for stationary objects and for standard reconstructions, can be understood regarding the fact that we used an approximate conebeam algorithm, where the artifacts are simply averaged over the multiple threads and thus appear less pronounced. The fact that the maximum pitch 共for standard reconstruction兲 increases with increasing G implies that it may pay to portion a given number of slices onto multiple threads even if one is not interested in cardiac CT. The spiral overscan 共the scan start lies one collimation before the first a desired image and the scan end lies one collimation after the last desired image兲 is smaller for multithreaded scanners than for single-threaded scanners, and hence the dose usage is improved. The pitch limit for phase-correlated reconstruction remains at p 艋 f Htrot regardless of the number of threads. G-threaded CT seems a promising technique to further enhance CT imaging. This is yet to be shown for most applications, but the benefit of multithreaded cardiac CT, i.e., its robustness against resonance cases and its improved temporal resolution, is evident and has been shown in this paper. a兲 Author to whom correspondence should be addressed. Electronic mail: [email protected] 1 D.-A. Sennst, M. Kachelrieß, C. Leidecker, B. Schmidt, O. Watzke, and W. A. Kalender, “Syngo Explorer: An extensible software-based platform for reconstruction and evaluation of CT images,” Radiographics 24, 601– 612 共2004兲. 2 M. Kachelrieß and W. A. Kalender, “Electrocardiogram-correlated image reconstruction from subsecond spiral computed tomography scans of the heart,” Med. Phys. 25共12兲, 2417–2431 共1998兲. 3 M. Kachelrieß, S. Ulzheimer, and W. A. Kalender, “ECG-correlated image reconstruction from subsecond multi-slice spiral CT scans of the heart,” Med. Phys. 27共8兲, 1881–1902 共2000兲. 4 K. Taguchi and H. Anno, “High temporal resolution for multislice helical computed tomography,” Med. Phys. 27共5兲, 861–872 共2000兲. 2447 Kachelrieß, Knaup, and Kalender: Multithreaded cardiac CT 5 M. Kachelrieß, S. Ulzheimer, and W. A. Kalender, “ECG-correlated imaging of the heart with subsecond multislice CT,” IEEE Trans. Med. Imaging 19共9兲, 888–901 共2000兲. 6 T. Flohr and B. Ohnesorge, “Heart rate adaptive optimization of spatial and temporal resolution for electrocardiogram-gated multislice spiral CT of the heart,” J. Comput. Assist. Tomogr. 25共6兲, 907–923 共2001兲. 7 M. Kachelrieß, T. Fuchs, R. Lapp, D.-A. Sennst, S. Schaller, and W. A. Kalender, “Image to volume weighting generalized ASSR for arbitrary pitch 3D and phase-correlated 4D spiral cone-beam CT reconstruction,” Proc. of the 6th Int. Meeting on Fully 3D Image Reconstruction, November 2001, pp. 179–182, www.fully3d.org 8 M. Grass, R. Manzke, T. Nielsen, P. Koken, R. Proksa, M. Natanzon, and G. Shechter, “Helical cardiac cone-beam reconstruction using retrospective ECG grating,” Phys. Med. Biol. 48, 3069–3084 共2003兲. 9 T. Flohr, B. Ohnesorge, H. Bruder, K. Stierstorfer, J. Simon, C. Suess, and S. Schaller, “Image reconstruction and performance evaluation for ECG-gated spiral scanning with a 16-slice CT system,” Med. Phys. 30共10兲, 2650–2662 共2003兲. 10 R. Manzke, M. Grass, T. Nielsen, G. Shechter, and D. Hawkes, “Adaptive temporal resolution optimization in helical cardiac cone beam CT reconstruction,” Med. Phys. 30共12兲, 3072–3080 共2003兲. 11 M. Kachelrieß, M. Knaup, and W. A. Kalender, “Extended parallel backprojection for standard 3D and phase-correlated 4D axial and spiral conebeam CT with arbitrary pitch and 100% dose usage,” Med. Phys. 31共6兲, 1623–1641 共2004兲. 12 W. A. Kalender, Computed Tomography, 2nd ed. 共Wiley & Sons, New York, 2005兲. 13 R. A. Robb, E. L. Ritman, B. K. Gilbert, J. H. Kinsey, L. D. Harris, and E. H. Wood, “The DSR: A high-speed three-dimensional x-ray computed tomography system for dynamic spatial reconstruction of the heart and circulation,” IEEE Trans. Nucl. Sci., NS-26, 2713–2717 共1979兲. 14 D. P. Boyd, “Transmission computed tomography,” In Radiology of the Skull and Brain—Technical Aspects of Computed Tomography 共Mosby, St. Louis, 1981兲, pp. 4357–4371. 15 R. A. Robb, Eric A. Hoffman, Lawrence J. Sinak, Lowell D. Harris, and E. L. Ritman, “High-speed three-dimensional x-ray computed tomography: The dynamic spatial reconstructor,” Proc. IEEE 71共3兲, 308–319 共1983兲. 16 Y. Liu, H. Liu, Y. Wang, and G. Wang, “Half-scan cone-beam CT fluoroscopy with multiple x-ray sources,” Med. Phys. 28共7兲, 1466–1471 共2001兲. 17 M. Kachelrieß, M. Knaup, C. Penßel, and W. A. Kalender, “Flying focal spot 共FFS兲 in cone-beam CT,” 2004 IEEE Medical Imaging Conference Record, April 2005, pp. 3759–3763. 18 T. G. Flohr, K. Stierstorfer, S. Ulzheimer, H. Bruder, A. N. Primak, and C. H. McCollough, “Image reconstruction and image quality evaluation for a 64-slice CT scanner with z-flying focal spot,” Med. Phys. 32共8兲, Medical Physics, Vol. 33, No. 7, July 2006 2447 2536–2547 共2005兲. M. Kachelrieß, M. Knaup, C. Penßel, and W. A. Kalender, “Flying focal spot 共FFS兲 in cone-beam CT,” IEEE Trans. Nucl. Sci. 53 共2006兲. 20 T. G. Flohr, C. H. McCollough, H. Bruder, M. Petersilka, K. Gruber, C. Süß, M. Grasruck, K. Stierstorfer, B. Krauss, R. Raupach, A. N. Primak, A. Küttner, S. Achenbach, C. Becker, A. Kopp, and B. M. Ohnesorge, “First performance evaluation of a dual-source CT 共DSCT兲 system,” Eur. Radiol. 16共2兲, 256–268 共2006兲. 21 M. Kachelrieß, M. Knaup, and W. A. Kalender, “Phase-correlated imaging from multithreaded spiral cone-beam CT scans of the heart,” Proc. of the 8th Int. Meeting on Fully 3D Image Reconstruction, pp. 159–162, July 2005, www.fully3d.org 22 M. Knaup, M. Kachelrieß, and W. A. Kalender, “3D and 4D imaging from multithreaded cone-beam CT,” IEEE Medical Imaging Conference Program, October 2005, pp. M03–373. 23 F. Noo, M. Defrise, R. Clackdoyle, and H. Kudo, “Image reconstruction from fan-beam projections on less than a short scan,” Phys. Med. Biol. 47共14兲, 2525–2546 共2002兲. 24 Y. Zou and X. Pan, “Exact image reconstruction on PI-lines from minimum data in helical cone-beam CT,” Phys. Med. Biol. 49, 941–959 共2004兲. 25 Y. Ye, S. Zhao, H. Yu, and G. Wang, “A general exact reconstruction for cone-beam CT via backprojection-filtration,” IEEE Trans. Med. Imaging 24共9兲, 1190–1198 共2005兲. 26 Y. Chen, H. Kudo, F. Noo, and M. Defrise, “Accurate and efficient image reconstruction for spatio-temporal CT,” IEEE Medical Imaging Conference Record, October 2004. 27 M. Kachelrieß, D.-A. Sennst, W. Maxlmoser, and W. A. Kalender, “Kymogram detection and kymogram-correlated image reconstruction from subsecond spiral computed tomography scans of the heart,” Med. Phys. 29共7兲, 1489–1503 共2002兲. 28 D. Ertel, M. Kachelrieß, and W. A. Kalender, “raw data-based generation of a heart motion function 共kymogram兲 using multithreaded CT scans of the heart,” Radiology 237共P兲, 697 共2005兲. 29 R. E. Alvarez and A. Macovski, “Energy-selective reconstructions in x-ray CT,” Phys. Med. Biol. 21共5兲, 733–744 共1976兲. 30 W. A. Kalender, W. H. Perman, J. R. Vetter, and Ernst Klotz, “Evaluation of a prototype dual-energy computed tomographic apparatus. I. Phantom studies,” Med. Phys. 13共3兲, 334–339 共1986兲. 31 J. R. Vetter, W. H. Perman, W. A. Kalender, R. B. Mazess, and J. E. Holden, “Evaluation of a prototype dual-energy computed tomographic apparatus. II. Determination of vertebral bone mineral content,” Med. Phys. 13共3兲, 340–343 共1986兲. 32 W. A. Kalender, E. Klotz, and L. Kostaridou, “An algorithm for noise suppression in dual energy CT material density images,” IEEE Trans. Med. Imaging 7共3兲, 218–224 共1988兲. 19