Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
informs
Vol. 39, No. 5, September–October 2009, pp. 476–490
issn 0092-2102 eissn 1526-551X 09 3905 0476
®
doi 10.1287/inte.1090.0463
© 2009 INFORMS
Modeling and Optimizing the Public-Health
Infrastructure for Emergency Response
Eva K. Lee, Chien-Hung Chen
Center for Operations Research in Medicine and HealthCare, School of Industrial and Systems Engineering,
Georgia Institute of Technology, and NSF I/UCRC Center for Health Organization Transformation,
Georgia Institute of Technology, Atlanta, Georgia 30332 {[email protected], [email protected]}
Ferdinand Pietz, Bernard Benecke
Strategic National Stockpile, Coordinating Office for Terrorism Preparedness and Emergency Response,
Centers for Disease Control and Prevention, Atlanta, Georgia 30333
Public-health emergencies, such as bioterrorist attacks or pandemics, demand fast, efficient, large-scale dispensing of critical medical countermeasures. By combining mathematical modeling, large-scale simulation, and
powerful optimization engines, and coupling them with automatic graph-drawing tools and a user-friendly
interface, we designed and implemented RealOpt© , a fast and practical emergency-response decision-support
tool. RealOpt allows public-health emergency coordinators to (1) determine locations for point-of-dispensing
(POD) facility setup; (2) design customized and efficient floor plans for PODs via an automatic graph-drawing
tool; (3) determine required labor resources and provide efficient placement of staff at individual stations within
a POD; (4) perform disease-propagation analysis, understand and monitor the intra-POD disease dilemma, and
help to derive dynamic response strategies to mitigate casualties; (5) assess resources and determine minimum
needs to prepare for treating their regional populations in emergency situations; (6) carry out large-scale virtual
drills and performance analyses, and investigate alternative strategies; and (7) design a variety of dispensing
scenarios that include emergency-event exercises to train personnel. These advanced and powerful computational strategies allow emergency coordinators to quickly analyze design decisions, generate feasible regional
dispensing plans based on best estimates and analyses available, and reconfigure PODs as an event unfolds.
The ability to analyze planning strategies, compare the various options, and determine the most cost-effective
combination of dispensing strategies is critical to the ultimate success of any mass dispensing effort.
Key words: public health; emergency response; mass dispensing; resource allocation; facility location; disease
propagation; medical countermeasures; bioterrorism; pandemic; infectious disease; anthrax; disaster
medicine; all-hazard emergency response; public-health informatics; integer programming; simulation;
decision-support system.
P
ublic-health emergencies, such as bioterrorist
attacks or pandemics, demand fast, efficient,
large-scale dispensing of critical medical countermeasures (i.e., vaccines, drugs, and therapeutics). Such
dispensing is complex and requires careful planning and coordination from multiple federal, state,
and local agencies, as well as the potential involvement of the private sector. Dispensing medications
quickly (within 48 hours for anthrax prophylactic)
to large population centers (with tens of thousands
or even millions of people) is urgent; moreover,
the multifaceted nature of dispensing (e.g., sending federal stockpiles to local points of dispensing
(PODs), coordination at the local level to manage the
transportation of citizens to PODs, and the POD operations) makes the process highly unpredictable. Thus,
emergency managers and public-health administrators must be able to quickly investigate alternative
response strategies as an emergency unfolds.
The focus of this paper is on mass dispensing of
medical countermeasures for protection of the general
population; however, large-scale public-health emergencies may involve thousands of sick or injured people who will require various levels of medical care,
ranging from patient evacuation, hospital care, and
sustainable and potentially long-term health-recovery
procedures. Thus, such emergencies present a daunting set of challenges, including the surge capability
476
Lee et al.: Modeling and Optimizing the Public-Health Infrastructure for Emergency Response
Interfaces 39(5), pp. 476–490, © 2009 INFORMS
and flexibility of our existing medical systems, federal
and state emergency capacity for rapid medical dispatching, and the resolve and resilience of health-care
workers and emergency responders to perform under
critical timelines and exceedingly stressful conditions.
In the wake of the 2001 anthrax attacks, the Department of Health and Human Services (HHS) increased
its order for smallpox vaccine, accelerated production,
and began working to develop a detailed plan for
the public-health response to an outbreak of smallpox. By January 2003, the United States had sufficient quantities of the vaccine for every person in
the country in an emergency situation (Gerberding
2003). HHS subsequently required each state to submit a mass-vaccination plan for administering smallpox vaccine. Furthermore, states are charged with
developing city-readiness programs that deal with
establishing regional treatment and dispensing centers, and developing procedures, policies, and a planning framework for efficient allocation of staff and
resources in response to these events.
The importance of such population protection has
been carefully studied for human, social, and economic benefits. Kaplan et al. (2002) argued that immediate mass vaccination after a smallpox bioterrorist
attack would result in fewer deaths and faster eradication of the potential epidemic; Wein et al. (2003) concluded that immediate and aggressive dispersion of
oral antibiotics and the full use of available resources
(local nonemergency care workers, federal and military resources, and nationwide medical volunteers)
are extremely important.
Mass Dispensing: Challenges
Mass dispensing requires the rapid establishment of
a network of dispensing sites and health facilities
that are flexible, scalable, and sustainable for medical
prophylaxis and treatment of the general population. Moreover, each POD must be capable of serving the affected local population within a specified
short time frame. Clearly, for very large-scale dispensing, the sophisticated logistical expertise needed to
deal with the complexities of selecting an adequate
number of strategically well-placed POD locations,
and of designing and staffing each POD, is beyond
the capability of any human planner or public-health
477
administrator. The limited availability of trained critical staff, such as public-health professionals, further
compounds the inherent complexities.
Rapid distribution of medical countermeasures
to a large population requires significant resources
within individual communities. Few, if any, cities are
presently able to meet the objective of dispensing
countermeasures to their entire population within 48
hours (the mortality rate is very steep after 48 hours
for anthrax exposure). The Strategic National Stockpile (SNS) is available to help agencies respond to
public-health threats that can be mitigated or eliminated by treating the affected population with the
antibiotics or vaccines that it contains. Although distribution of countermeasures by the federal government can leverage the distribution infrastructure of
couriers, such as FedEx, UPS, and USPS, the last mile
of dispensing to the broad regional population requires
strategic and operational planning of a network of
POD sites, including the determination of appropriate
staffing at each POD, to ensure that a practical plan is
in place to accomplish the task within the given time
constraint. These last-mile issues form the crux of the
discussion and advances we present in this paper.
Since 2003, exercise drills have been conducted
regularly throughout the nation to better prepare
public-health personnel to realistically plan for mass
dispensing. Beaton et al. (2003) reported an exit
survey of a drill held in the state of Washington.
Giovachino et al. (2005) presented postdrill analysis
of an exercise conducted in the District of Columbia.
Aaby et al. (2006) explained how Montgomery County
(Maryland) Public Health Services used operations
research techniques to improve its clinic planning. Lee
et al. (2005; 2006a, b; Lee 2008) described RealOpt’s
development for POD design, resource allocation,
and real-time dynamic response. Gebbie et al. (2006)
defined criteria for the performance evaluation of
drills. Some researchers, such as Lien et al. (2006),
examined the role that the private sector (e.g., retail
chains, such as grocery stores and wholesale clubs)
can play as community centers in partnership with
public-health authorities for the mass distribution of
vaccines or antibiotics. Retail grocery and wholesale
stores already have experience with dispensing annual
influenza vaccinations and could be an excellent
resource in a public-health emergency. Nelson et al.
478
Lee et al.: Modeling and Optimizing the Public-Health Infrastructure for Emergency Response
(2007) addressed the definition, measurement, and
determination of sufficiency of public-health emergency preparedness, and they reviewed the current
approaches. Lee et al. (2009c) offered a multimodality
strategy for planning a realistic mass-dispensing event
in a region with over five million people. The work
includes discussion of cost-effective operations analyses and of public and private sector involvement.
SNS stockpiles sufficient anthrax antibiotics and
smallpox vaccine for the entire population; however, a key mass-dispensing challenge is the need
to dispense to the entire regional population under
scarce staffing resources and within a very tight
time line. Mason and Washington (2003) used operations research techniques to assist in staffing a
smallpox POD site when limited staffing is available. The discrete-event simulation model they developed, Maxi-Vac, offers insight on the practicality of
a simulation system in emergencies. However, its
implementation revealed the severe bottlenecks of
commercial simulation and optimization software.
Each scenario involved about 30 staff and had an
objective of maximizing throughput; however, each
required more than 10 hours to generate a usable, feasible solution. Furthermore, the resulting cycle time
tended to be too long for practical purposes. A subsequent field exercise and study highlighted the importance of a real-time system in which users can develop
operational plans based on their regional needs, analyze trade-offs, and perform dynamic changes on
staffing assignment and (or) floor-plan reconfiguration in response to patient flow as an event unfolds.
Since 2003, we have worked with the Centers
for Disease Control and Prevention (CDC) and state
public-health agencies to design and implement
RealOpt to aid users in determining large-scale, realtime resource allocation. The system enables publichealth administrators to enter values of their choosing
and obtain results that best reflect their emergencyresponse operating environment. Through the design
and integration of efficient optimization technology
and large-scale simulation, RealOpt allows users to
investigate (1) locations for dispensing-facility setup,
(2) clinic and POD layout design, (3) staff allocation,
and (4) disease-propagation analysis. Optimal or nearoptimal solutions of instances of staff allocation models for regions with populations in the hundreds of
Interfaces 39(5), pp. 476–490, © 2009 INFORMS
thousands or millions can be achieved within two
to four CPU minutes, with queue lengths, wait time,
cycle time, and staff utilization rates that are acceptable and practical for actual operations.
Medical Countermeasures Dispensing:
Modeling and Computation
Depending on the type of medical countermeasures
that are to be dispensed, PODs can have various layouts. Lee et al. (2006a, b; 2009c) give detailed descriptions and contrast trade-offs for various POD layout
designs of drive-through and walk-through models for prophylaxis medical dispensing in response
to anthrax, smallpox, and flu pandemic scenarios.
Briefly, within a POD facility, the tasks include
(1) assessing client health status; (2) assessing client
eligibility to receive service; (3) assessing implications
of each case and referring case for further investigation, if necessary; (4) counseling clients regarding
services and associated risks; (5) administering services; (6) educating clients regarding adverse events;
(7) documenting services; (8) monitoring vaccine
and medical prophylaxis take rates; (9) monitoring adverse reactions; and (10) monitoring disease
development.
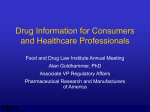
Figure 1 shows a POD for anthrax antibiotics dispensing that was set up in one of the national drill
exercises. Citizens must either drive to the POD site or
Arrival
Triage
decision
Triage
Normal
Registration
Special
Special
medical
care
Medical
screening
Drug
dispensing
Exit
Figure 1: The flowchart shows a POD that was set up in a national drill
exercise to dispense anthrax antibiotics.
Lee et al.: Modeling and Optimizing the Public-Health Infrastructure for Emergency Response
Interfaces 39(5), pp. 476–490, © 2009 INFORMS
to a central location from which a bus transports them
to the POD. This POD consists of five main blocks:
triage, registration, medical screening, drug dispensing, and special medical care. At triage, staff members
greet clients, ask if they have questions, and assess
how to direct clients. They direct most clients to registration. However, they might direct some (e.g., clients
with preexisting conditions who are taking medications that require extra medical advice or assistance)
to special medical care. At the special medical care
stations, staff members assist clients with registration, attend to their special medical concerns, and dispense drugs (when appropriate). Staff members might
also direct families with children to special medical
care because the drug dispensed will depend on a
child’s age and weight. At registration, clients fill out
forms about their health. At medical screening, the
staff members review the forms and determine which
antibiotics should be given. At the drug dispensing
station, clients receive the drug and final consultation
from the staff, and then they exit the system.
Mathematical and Computational Advances
Maxi-Vac and drill exercises have demonstrated that
a simulation system that captures the stochasticity of
the emergency operations within a POD—and seeks
to optimize the resource allocation and throughput—
is essential. However, the CDC benchmark using
commercial systems proved that these systems are
computationally not feasible for solving even a small
scenario (e.g., one that involves 30 staff members and
service to approximately 1,000 households). A closedform solution of a system assumed to be in steady
state is not helpful because in the short time window in which dispensing must be completed, the
system will not achieve a steady state. Moreover,
a deterministic, analytic resource calculation often
underestimates resource needs and is inefficient and
impractical for drill planning and actual usage. The
challenge herein involves the integration of simulation and optimization into a seamless decisionsupport system that can perform rapid optimization
over each simulation iteration.
The coupling of the simulation and optimization
processes is useful because a simulation is typically
a much more realistic evaluator of system performance (objective function), and a good optimization strategy helps in speedy convergence toward the
479
desired set of parameters that produce the best system
performance. However, this approach has considerable difficulties. First, a realistic simulation is typically
computationally intensive, thereby limiting the number of times it can be used to evaluate the objective
function for optimization. Second, most optimization
algorithms work best with convex objective functions.
A realistic simulation will seldom meet this condition. Therefore, the coupling of simulation and optimization remains a big challenge for the research
community.
Resource-Allocation Model and
Solution Strategies
Given a staff assignment (obtained from an initial
optimization step) and input of service distributions
at each station, we model and simulate the movement
of individuals inside a POD. The simulation output
is a set of parameters (including statistics of average
flow time, queue length, wait time, utilization rate,
etc.) that enables evaluation of the objective function
being optimized (e.g., the resulting throughput).
The optimization of labor resources involves placement of staff at various stations in the POD to maximize throughput or minimize the staffing needs to
satisfy a preset throughput. The cost at each station
depends on the type and number of workers who
are assigned to that station and have the required
skills, and on the average wait time, queue length,
and utilization rate of the station. The total system
cost depends on the cost at each station and on system parameters, such as cycle time and throughput.
These cost functions are not necessarily expressible in
closed form.
Constraints in the model include maximum limits
on average wait time and queue length, range of utilization desired at each station, and upper and lower
bounds on the number of workers with the required
skills who are needed to perform various tasks at
the POD. Constraining the average cycle time to be
less than a prespecified upper bound is critical for
emergency response because individuals must move
through the system as quickly as possible to facilitate crowd control, reduce sources of human frustration and potential disorderly outbursts, and reduce
the potential spread of disease or contamination. Our
CDC collaborator indicated that an acceptable upper
480
Lee et al.: Modeling and Optimizing the Public-Health Infrastructure for Emergency Response
bound is 90 minutes. The resulting nonlinear mixedinteger program (NLMIP) poses a challenge for existing optimization engines (see the appendix).
Mason and Washington (2003) illustrated the difficulty of a simplified version of this resource-allocation
problem for a smallpox POD scenario running on
a popular commercial simulator and optimization
solver. Their input included the distribution of service
times at various stations in the clinic and the availability of 30 public-health staff members to work during
a 12-hour shift. The objective was to determine the
staffing assignments that result in the best throughput. We confirmed CDC’s benchmarking results by
testing several commercial simulation and optimization systems; many exhibited similar computational
bottlenecks: After running for roughly 10 hours, the
staff assignment returned did not satisfy the desired
requirements related to flow and queue and wait
time; in addition, the throughput achieved was fewer
than 800 households.
Working closely with public-health emergency
directors, our team developed a simulation and optimization system from scratch using the Java programming language. Our crude implementation in winter
2003 solved the instance described in the previous
paragraph in 1.09 seconds and returned a feasible
assignment with a throughput of 1,117 households.
For the 2007 benchmark of 100 workers running
the simulation over a 36-hour period, our system
returned a feasible assignment within 30 seconds with
a throughput of 12,013 households.
At each simulation, the NLMIP is solved using a
fast, adaptive local search heuristic. The algorithm
uses a fluid model to approximate system dynamics and estimate performance; it estimates the average delay and service time associated with the current
staff assignment. Then it performs a greedy adaptive step to increase staffing for those stations with a
total wait time exceeding the constraint limit until it
reaches the desired cycle time. Similarly, it increases
staffing at those stations with the longest average
wait time until it reaches a desirable level. It repeats
this greedy adaptive process until it achieves feasibility. When the objective is to minimize resources, the
heuristic terminates. When the objective is to maximize throughput, it repeatedly performs the greedy
adaptive step until it assigns all available workers. It
Interfaces 39(5), pp. 476–490, © 2009 INFORMS
then matches up the resulting staff assignment and
optimizes over the types of available (prioritized)
workers via a minimum-cost network flow algorithm.
When optimization completes, it performs the next
simulation iteration, which feeds the service information resulting from the simulation run into the
heuristic algorithm. The process of simulation and
optimization repeats and, upon termination, returns
a feasible, near-optimal staffing assignment.
Emergency planners can maximize the throughput
under limited staffing availability, or minimize the
staffing needs to satisfy a prespecified throughput.
They can also manually input their staff assignment
and allow our simulator to return the service statistics
for evaluation of performance. We have fine-tuned
the search step such that the heuristic seeks to simultaneously optimize the staffing assignment, equalize
worker utilization rate, and minimize the average
cycle time. It achieves this by varying the different
greedy criteria within the adaptive heuristic procedure to achieve the desirable service statistics upon
termination.
The adaptive heuristic returns a good staffing
assignment within two CPU minutes when the
desired throughput ranges from tens of thousands
to millions. Moreover, the resulting utilization rates,
wait times, and cycle times appear to be superior
to other solutions. Because individuals should move
through the system as quickly as possible, short cycle
and wait times are critical; a balanced utilization rate
is desirable for both the morale and physical wellbeing of workers.
To measure performance, we have also benchmarked the quality of this heuristic against the
solution from our in-house nonlinear mixed-integer
program (MIP) solver. Although the solver can solve
to optimality instances of approximately hundreds
of thousands of households, its computational time
is over 10,000 CPU seconds. The heuristic algorithm
consistently returns solutions that are within 5 percent of optimality in less than two minutes.
POD-Location Model and Computational
Challenges
To best use public-health resources to maximize
region-wide throughput of emergency treatment, our
team works with local emergency-preparedness directors to investigate POD locations that best serve the
Lee et al.: Modeling and Optimizing the Public-Health Infrastructure for Emergency Response
481
Interfaces 39(5), pp. 476–490, © 2009 INFORMS
10,000,000
1,300,000
1,200,000
1,100,000
1,000,000
900,000
800,000
700,000
600,000
500,000
400,000
300,000
200,000
100,000
10 – 0
05 – 2
04 – 0
03 – 5
03 – 4
03 – 3
03 – 2
03 – 1
02 – 0
01 – 2
0
01 – 1
regional population. For a given regional population,
we determine the number of POD locations needed
for cost-effective operations and determine the assignments of households to the various PODs. We solve
this via a two-stage approach by first solving for the
minimum number (and operating cost) of PODs and
then minimizing the travel distance and time for each
household to reach its assigned POD.
To model the POD-location problem and population needs, we first discretize the targeted region into
subregions called grids. To each grid, we associate its
population based on known US Census population
densities. Each grid has a selection of potential POD
locations (these locations could include large warehouses, community centers, or churches) depending
on the mode of dispensing.
Given the total number of jurisdictions in the
region, we formulate the capacitated POD-location
problem COVER-CAP (see the appendix) to ensure
that at least two PODs are opened for each jurisdiction. If a catastrophic event at one site necessitates
shutting down a POD, the remaining location can
continue to carry out the emergency dispensing. The
model also ensures that each household will travel
at most dmax miles (the maximum allowed travel distance), that every household is served, and that the
capacity of the facility is not violated (e.g., POD parking capacity is limited and fire codes limit the number
of individuals who can be inside a facility simultaneously).
COVER-CAP returns the minimum total number of PODs needed for each jurisdiction. Next, the
MINAVG-CAP problem (see the appendix) is formulated. This formulation seeks to minimize the travel
distance and time over all households while keeping
the number of PODs in each jurisdiction fixed to the
optimal value that the COVER-CAP problem determined. When there is no sharing of staff resources,
these two problems can be solved independently for
each jurisdiction.
The metro Atlanta area, with a population of 5.2
million people, has 11 districts (jurisdictions), each
of which has multiple counties. Using a grid size of
one mile by one mile, the number of grid squares
per district ranges between 36 and 3,275, and the
number of households within grid squares ranges
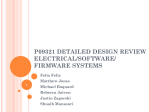
Figure 2: The graph shows the number of 0/1 variables in each PODlocation MIP instance for the 11 districts. Only two instances have fewer
than 100,000 0/1 variables.
between 140 and 3,074. Figure 2 graphically compares the number of 0/1 variables for COVER-CAP
for each of the 11 districts; problem sizes range
from 20880 × 21025 constraints and variables in
the smallest instance to 9452550 × 9455625 in the
largest instance. Although there have been many computational advances in facility location, the general
problem remains NP-hard. We performed benchmark
tests on these instances using CPLEX V11. CPLEX
returned an optimal number of facilities for the smallest instance within 30 CPU minutes when the POD
capacity was set to 2,000 people per hour; however,
for this same instance, it cannot solve the problem
within a week of CPU time when the facility capacity
is 500 per hour. CPLEX was not able to solve any of
the other instances after running for several months
of CPU time.
Our challenge was to find optimal or near-optimal
solutions rapidly so as to be practical for emergency directors. Using recent computational advances
for solving intractable facility-like instances (Lee and
Zaider 2008), we were able to solve all except one
instance to optimality within 300,000 CPU seconds.
Specifically, we ran COVER-CAP and MINAVG-CAP
for dmax ranges from 2 to 34 for the 11 districts. Of
the total 2,904 MIP instances, we were able to solve
all except 5 to proven optimality within 40,000 CPU
seconds. Uniformly, the capacity-500 instances were
482
Lee et al.: Modeling and Optimizing the Public-Health Infrastructure for Emergency Response
the most difficult to solve. Four of the remaining
instances required approximately 300,000 CPU seconds to solve to proven optimality, and one remains
unsolved. More importantly, in all solved instances,
we obtained a feasible solution that is within 5 percent of optimality within 5,000 CPU seconds.
To reduce the computational time further for
scenario-based analyses, we designed a specialized
heuristic approach that couples features of a genetic
algorithm and an adaptive greedy search. When using
the permutation representation of a chromosome, the
challenge is to find feasible opened facilities that
satisfy both capacity and distance constraints. In addition, maintaining solution feasibility during the evolutionary process can require extra computational
effort and reduce solution quality. To overcome this,
for each location we introduced the concept of potential served set (i.e., a subset of the population) that
the location can serve feasibly. Instead of using the
indexes on a chromosome as the sequence of open
facilities and attempting to assign population grids to
their closest facility in a feasible manner, we generate a potential served set for each candidate facility.
This is analogous to Aickelin’s set-covering approach
(Aickelin 2002). By doing so, we can consider indexes
on a chromosome as the sequence of potential served
sets. Using potential served sets in the decoding procedure ensures the solution feasibility is independent
of the evolutionary process of the genetic algorithm
and also provides better opportunities to eliminate
redundant open facilities. Our heuristic routine also
implements and embeds some features of adaptive
greedy search procedures to further improve the solution quality. The initial population is partly randomly
generated and partly generated via a k-mean clustering algorithm to ensure better initial and finalsolution quality. Furthermore, we apply kick-move
and local search to maintain the balance between
search diversification and intensification. Specifically,
kick-move search is implemented by replacing a fraction of chromosomes that carry the current best objective values with randomly generated chromosomes.
The rapid solution engine and quality of returned
solutions facilitate the study of efficient frontiers to
analyze the trade-offs in determining the most suitable number of strategically placed POD sites to best
serve the regional population. For the metro Atlanta
Interfaces 39(5), pp. 476–490, © 2009 INFORMS
area, our POD-location solver allows us to obtain
good feasible solutions that are within 8 percent of
optimality in less than 15 minutes. (The hardest two
instances with 500-capacity constraints ran for about
15 minutes; most other instances required less than 3
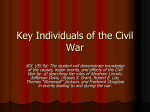
minutes.) Figure 3 shows the efficient frontier (tradeoff) between the number of facilities needed to serve
the regional population and the maximum distance
traveled by each household. This required solving
2,904 very challenging MIPs. Figure 4 shows the distribution of distances traveled by households for a
solution with a capacity limit of 1,500 per hour and a
maximum travel distance set to 10 miles.
The Decision-Support System:
RealOpt
To provide a framework for modeling and optimizing the public-health infrastructure for all hazard
emergency responses, we have designed and implemented a software suite of decision-support systems,
RealOpt (RealOpt 2003–2009). The enterprise system
consists of stand-alone software and decision-support
systems, including RealOpt-Regional© , RealOpt-POD© ,
RealOpt-RSS© , and RealOpt-CRC© . It has been used in
the areas of biological or radiological terrorism preparedness, infectious-disease outbreak planning, and
natural-disaster response planning.
RealOpt-Regional is an interactive online software
enterprise system for large-scale regional medical
dispensing and emergency preparedness. It features
interactive visualization tools to assist users with spatial understanding of important landmarks in the
region, assess the population densities and demographic makeup of the region, and identify potential
facility locations. It features the backend mathematical models for large-scale facility-location problems
and the novel and rapid solution engine, as described
here in the POD-location section, for strategic and
operational planning and real-time dynamic optimization. The rapid computational engine for solving large-scale instances in the POD-location module
is critical for regional planning, in which emergency
managers must map out facility locations that offer
the most effective dispensing strategies, and analyze
the economic and potential benefits of resource sharing across counties.
Lee et al.: Modeling and Optimizing the Public-Health Infrastructure for Emergency Response
483
Interfaces 39(5), pp. 476–490, © 2009 INFORMS
300
Cap = 2,000
Cap = 1,000
Number of facilities required
250
Cap = 1,500
Cap = 500
200
150
100
50
0
5
6
7
8
9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
Maximum allowed travel distance (mile)
Figure 3: The graph shows the efficient frontier (PODs versus distance traveled) under various hourly capacity
(Cap) restrictions. The solid lines represent the proven optimal solutions, and the dotted lines represent the
heuristic solutions.
RealOpt-POD is a stand-alone computerized decision-support system for facility layout and resource
allocation. It consists of three core components: the
Simulation Manager, the Optimization Manager, and
the User Interface and Linker Manager. The Simulation
Manager is responsible for running the simulations
and extracting the various statistics (e.g., average wait
time, average queue length, average utilization rate,
etc.) from the POD (service facility). The Optimization
Manager contains the various exact algorithms and
Capacity = 1,500, dmax = 10
0.16
Fractional frequency of occurence
0.14
0.12
0.10
0.08
0.06
0.04
0.02
0
0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
5.5
6.0
6.5
7.0
7.5
8.0
8.5
9.0
9.5
Distance traveled (miles)
Figure 4: The graph shows the actual distance that each household travels to its assigned POD when the facility
capacity is 1,500.
10
484
Lee et al.: Modeling and Optimizing the Public-Health Infrastructure for Emergency Response
fast heuristics for resource allocation. In the resourceallocation module, the Simulation Manager is called
repeatedly to resolve and update resource-allocation
statistics. The User Interface and Linker Manager is
responsible for all functions related to input of data
and displaying of results. These three components
and a graph-drawing tool with drag-and-drop features are integrated seamlessly into RealOpt-POD.
This latter tool allows users to design specific floor
plans to enable lay users to easily build simulation
models. The system allows input of raw data and
goodness-of-fit parameters to capture the service time
into the model in real time. Moreover, we developed
the entire system using Java for easy portability across
different computer platforms and PDAs, eliminating
the need for administrators of cash-strapped publichealth agencies to purchase proprietary licenses for
compilers.
RealOpt-POD takes only a few minutes to determine the staffing allocation for instances with
required throughput in the order of hundreds of thousands or millions. This allows regions to develop
operational plans for mass dispensing, analyze facility design and study labor trade-offs, and estimate
resources needed for protection of the general population. It also allows state emergency managers to
assess their current regional labor resources and to
sufficiently and objectively allocate resources to various jurisdictions to ensure the most cost-effective
POD operations.
RealOpt-RSS is a tool for the efficient management
of the logistics of receipt, stage, and storage (RSS)
facilities and regional distribution nodes for medical
countermeasures (RealOpt 2003–2009), and RealOptCRC relates to population health monitoring for radiological emergency planning and response. It shares
some key components of RealOpt-POD, with added
components to deal with radiological screening and
decontamination logistics (Lee et al. 2009a).
The real-time capability of RealOpt means that
users can enter different parameters into the system
and obtain results very quickly. It facilitates analysis
of “what-if” scenarios; thus, it serves as an invaluable
tool for planning and reconfigurations.
Interfaces 39(5), pp. 476–490, © 2009 INFORMS
Disease-Propagation Analysis: Mitigation
Strategies and Choice of Dispensing Modalities
Large-scale dispensing clinics could facilitate the
spread of disease because of their high-volume population flow. The field of dynamical systems (mostly
differential equation systems) provides the principle methods of modeling in classical mathematical epidemiology (Anderson et al. 1992, Diekmann
and Heesterbeek 2000). Despite their simplicity when
compared to recent complex simulation studies
(Ferguson et al. 2005, 2006; Longini et al. 2005;
Germann et al. 2006), these methods have helped
generate functional insights, such as the transmission
threshold for the start of an epidemic and the vaccination threshold for containment of an outbreak.
As modelers attempt to incorporate more realistic
dynamics into their models (such as stochasticity,
nonexponential waiting times, sample-path dependent events, demographical and geographical data,
etc.), more flexible tools, such as individual-based
stochastic simulations, are preferable. Although simulation is a powerful approach, it is less mathematically tractable (i.e., it requires intensive computing
time) than the classical methods.
The rapid simulation and optimization modeling
and computational ability of RealOpt opens up an
opportunity to explore disease-propagation studies
in which stochasticity of systems can be incorporated readily. RealOpt includes a disease-propagation
module that aids users in understanding facility
design and flow strategies that mitigate the spread
of disease. The module incorporates the standard
four-stage SEIR (susceptible, exposed, infectious, and
recovered) model (Kermack and McKendrick 1991)
and a novel six-stage SEPAIR model (Figure 5) to
capture the disease development (i.e., asymptomatic
or symptomatic). By distinguishing the symptomatic
stage from the asymptomatic stage, this model allows
one to examine the effect of triage accuracy in facility
design. We can show that improving triage accuracy
is critical when a disease has a higher probability of
explicitly showing symptoms in patients.
Lee et al. (2009b) give a detailed theoretical and
computational analysis of disease propagation and
strategies for mitigation during biological or pandemic outbreaks and mass dispensing. In addition to
Lee et al.: Modeling and Optimizing the Public-Health Infrastructure for Emergency Response
485
Interfaces 39(5), pp. 476–490, © 2009 INFORMS
S
E
R
P
I
D
Figure 5: The flowchart shows an epidemiology model in which the infectious disease develops in six stages: susceptible (S), exposed (E), infectious (P), asymptomatic (A), symptomatic (I), and recovered (R). A small
percentage of patients might not recover from the asymptomatic or symptomatic stage and therefore die (D).
the stochasticity of client arrival and service distribution that RealOpt can accept, it also accommodates
the following factors.
• The clinic model can be represented as an
n-server system with queuing; transmission can occur
between clients or between clients and staff. In a real
emergency, staff members will be given medical countermeasures to protect them from the disease prior to
their assignment to POD services. However, a medical
countermeasure does not provide 100 percent protection; each staff member still has a small probability of
being infected by clients.
• The intraclinic infectivity between clients and
staff can vary.
• If symptomatic individuals are not triaged out
properly during the initial screening, they could infect
other people inside the POD. The system allows users
to observe the effect of triage and screening errors,
determine improved strategies for triage and screening, and establish guidelines for mitigating the spread
of disease because of such errors.
• Inhomogeneous mixing within the community is
possible.
• The infectious, asymptomatic, and symptomatic
individuals can infect at various rates.
RealOpt offers very flexible and realistic clinicdesign and modeling features that facilitate diseasepropagation analysis. For example, it allows one to
investigate and contrast the effect of standard incidence versus simple mass-action incidence infection.
Likewise, we can investigate the effect of centralized versus decentralized POD design. We can also
model batch processing in areas such as orientation or
bus transportation, situations in which relatively large
numbers of patients are in contact with one another
30
No. of intra-POD infection
A
25
Triangular
Exponetial
ODE
20
15
10
5
0
0
5
10
15
20
25
30
35
40
Time (hr.)
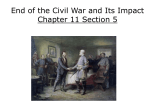
Figure 6: The graph contrasts the number of intra-POD infections over a
36-hour period (with a total throughput of 36,000) when various stochasticity is incorporated into the RealOpt simulation run using the sixstage epidemiology model. Triangular and exponential correspond to the
service-distributions input to RealOpt. The symptomatic proportion is 67
percent, contact number is 193 (for outer-POD disease propagation), and
−5
transmission coefficient = 018E /min for intra-POD disease propagation. The incoming percentage for susceptible is 95 percent, and infectious is 5 percent. The mean dwell time is one day for both exposed and
infectious and three days for asymptomatic and symptomatic.
for extended periods, and thus can be areas of high
infectivity.
Figure 6 highlights that the ordinary differential
equations (ODEs) model underestimates the number of intra-POD infections. Our disease-propagation
module considers the stochasticity of patient arrival
and service-probability distributions, thereby generating more accurate estimates. Figure 7 contrasts the
triage accuracy with respect to the symptomatic proportion, when simple mass-action incidence infection,
as Lee et al. (2009b) describe in detail, is considered. This analysis assesses errors in triage and
their infection consequences. It provides estimates for
POD planners and epidemiologists to use to help
them determine the level and expertise of triage that
should be in place with respect to the transmission
coefficient.
Such analyses may influence the selection of dispensing modalities. Specifically, over the past few
years, we have observed more use of drive-through
PODs for infectious-disease prophylaxic dispensing
(e.g., seasonal flu vaccination for communities). In
January 2008, a hepatitis A confirmation of a grocery worker triggered the prophylaxic vaccination
of 10,000 residents in Erie County, New York, who
were potentially exposed to the disease, costing the
486
Lee et al.: Modeling and Optimizing the Public-Health Infrastructure for Emergency Response
Interfaces 39(5), pp. 476–490, © 2009 INFORMS
No. of intra-POD infections
and collected data from actual clinical visits. We also
performed role-playing with public-health officials.
In addition, since 2005, the team has been collecting
time-motion study data at various anthrax and smallpox drill exercises as well as actual flu and hepatitis
vaccination events.
The User Interface and Linker Manager includes a
goodness-of-fit panel. The goodness-of-fit test, based
on a chi-square test, allows users to determine the
probability distribution from data collected in real
time; the module includes different probability distributions, significance levels, and numbers of intervals.
Symptomatic proportion (%)
Triaging accuracy
Figure 7: The graph shows the triage accuracy versus symptomatic proportion and the importance of using the SEPAIR six-stage propagation
model, because it allows us to examine the effect of implementing triage
accuracy. The graph shows the number of intra-POD infections under
different triage accuracy and symptomatic proportions. The throughput is 36,000 over a period of 36 hours. The contact number is 193
(for outer-POD disease propagation), and the transmission coefficient is
−5
018E /min. The incoming percentage for susceptible is 95 percent and
infectious is 5 percent. The mean dwell time is one day for both exposed
and infectious and three days for asymptomatic and symptomatic.
county’s public-health agency at least $500,000. The
health department dispensed the first vaccination in
February when it set up a stationary clinic (walkthrough POD). Because of the medical logistics and
infectious nature of the disease, some people had to
wait for hours in frigid temperatures. In September
2008, the health department used a hepatitis A followup drive-through POD to provide a second round
of vaccinations to individuals potentially exposed to
the disease. The POD was also the first test of the
county’s drive-through plan. The drive-through process is quick, efficient, and convenient, and it minimizes the potential of intra-infectivity (Tan 2008).
Input Data: Challenge, Time-Motion Study, and
Real-Time Data Processing
In addition to the computational challenges, an early
difficulty that we encountered was the lack of historical data for mass dispensing services. To perform optimization and resource-allocation analysis, it
is imperative that we enter realistic distributions for
client-service and arrival times. To obtain data for service distribution, we performed a time-motion study
Validation and Successful Usage
of RealOpt
Since 2003, we have distributed RealOpt to more than
1,000 public-health and emergency coordinators from
tribal, local, state, and federal public-health departments, including the CDC.
In 2005, the planning and resource-estimation capability of RealOpt was tested and validated in an
eight-county anthrax emergency drill in Georgia. This
exercise involved between 600 and 700 public-health
workers, hundreds of law-enforcement officers, and
thousands of volunteers. Each county was responsible for its own planning and execution of the drill;
only one county, DeKalb, used RealOpt to determine its POD layout and staffing needs. DeKalb
achieved the highest throughput among all counties that simultaneously conducted the same scale
of anthrax drill at various locations. Moreover, it
was the only county that achieved and exceeded
the targeted throughput; it processed 50 percent
more individuals than the second-place county. Its
labor usage was at or below that of the other
counties. The independent state external evaluators
commented that DeKalb produced the most efficient floor plan (with no path crossing), the most
cost-effective dispensing (lowest labor-to-throughput
ratio), and the smoothest operations (shortest average wait time, average queue length, equalized utilization rate) (Moriarty 2006). This anthrax exercise
suggests that even without historical data, using our
system, one can plan wisely and obtain good estimates of required labor resources. Currently, RealOpt
includes time-motion study data from anthrax and
Lee et al.: Modeling and Optimizing the Public-Health Infrastructure for Emergency Response
Interfaces 39(5), pp. 476–490, © 2009 INFORMS
smallpox exercise drills, seasonal flu-vaccine events
(walk-through and drive-through), and drive-through
hepatitis A booster shoots (Tan 2008).
RAND Corporation employed RealOpt to analyze the most effective POD layout design for drill
exercises. New Orleans emergency-response planners
used it for their October 2007 mass-vaccination drill
in which the community received free flu shots when
the emergency team tested its capabilities of running
a POD. The local team used RealOpt for the clinic
design and for estimating staffing needs. It correctly
predicted bottlenecks for the planners; the throughput
numbers the system returned were fairly close to the
actual numbers (these individuals actually received
flu shots), thus validating the importance of such a
decision-support system.
Strategic and Regional Planning for Effective
Multimodality Mass Dispensing
To illustrate RealOpt’s strategic capability and importance, we have been working with a team of
emergency-response directors in the Georgia City
Readiness Initiative to develop a mass-dispensing
plan for an anthrax event for the metropolitan Atlanta
area (Lee et al. 2009c). Briefly, working together
with public-health directors, and with the aid of
the systems approach and decision tools we present
in this paper, we designed a cost-effective massdispensing network for anthrax prophylaxic dispensing (Figure 8).
This heterogeneous mix of PODs, capable of serving the entire regional population in a 48-hour period,
is selected based on both operational efficiency and
optimal staff utilization. The study reveals that
(1) sharing labor resources across counties and districts within the same jurisdiction is important;
(2) the most cost-effective dispensing plan across
a region consists of a combination of drive-through,
walk-through, and closed PODs, each operating at a
throughput rate that depends on the surrounding population density, facility type, and labor availability;
(3) the optimal combination of POD modalities
changes according to various facility capacity restrictions, and the availability of critical public-health
personnel;
(4) an increase in the number of PODs in operation
does not necessarily increase the total number of core
public-health personnel needed;
487
(5) optimal staffing is nonlinear with respect to
throughput; thus we cannot estimate the optimal
staffing and throughput by simply using an average
estimate; and
(6) depending on the population, an “optimal”
capacity that provides the most effective staffing
exists for each POD location. If a POD is operating
above its optimal capacity, reduction in capacity (and
thus hourly throughput) eases the crowd-control tasks
of law enforcement personnel and helps to minimize
potential operational problems inside the POD.
RealOpt has been used successfully in planning for
biodefense drills (e.g., anthrax, smallpox) and pandemic response events in various locations in the
United States since 2005. Users have tested various
POD layouts, both drive-through and walk-through.
Because of the system’s rapid speed, it facilitates
analysis of what-if scenarios and serves not only
as a decision tool for operational planning, actual
drill preparation, and personnel training, but also
allows dynamic reconfigurations as an emergency
event unfolds. In addition, it supports performing
“virtual field exercises,” offering insight into operation flows and bottlenecks when mass dispensing is
required.
Appendix. Resource-Allocation Model
The optimization of labor resources involves placement of staff at various stations in a POD to maximize
throughput or minimize staffing needs to satisfy a
predetermined throughput. Constraints in the model
include maximum limits on wait time and queue
length; range of utilization desired at each station,
type, and number of skilled workers, respectively,
who can perform various tasks in the POD; and a
maximum limit on the cycle time of the individual.
The model parameters are as follows:
S: the set of stations in the POD;
T : the set of available types of workers;
kij : the cost of assigning a worker of type i to station j, i ∈ T , j ∈ S;
ij and mij : the maximum and minimum numm
ber of workers, respectively, of type i that may be
assigned to station j, for i ∈ T , j ∈ S;
T ⊆ T : for K ∈ T, nK is the number of available
workers who can assume the role of the worker types
represented by K;
Lee et al.: Modeling and Optimizing the Public-Health Infrastructure for Emergency Response
488
Interfaces 39(5), pp. 476–490, © 2009 INFORMS
Drive-through PODs
throughput rate:
0 < 500
500 < 1,000
1,000 < 1,500
Walk-through PODs
0 < 500
500 < 1,000
1,000 < 1,500
Closed PODs
Airport
Prisons/jails
Assisted living
Colleges
/universities
Large corporate
offices
Homeless
shelters
Mobile PODs
Figure 8: The map shows an effective dispensing strategy that involves a network of public and private dispensing
sites of various throughput sizes and dispensing modalities. Blue (red) represents walk-through (drive-through)
dispensing sites, with various hourly throughput rates. In addition to these public PODs, closed PODs are set up
in large corporate offices, university and college campuses, assisted living facilities, prisons and jails, homeless
shelters, and at the airport. The map does not show the mobile PODs.
wj qj , and uj : the average wait time, average
queue length, and average utilization rate, respectively, at station j, j ∈ S;
C: the average cycle time (i.e., length of time a
patient spends in the system); and
: the average throughput (number of patients serviced in a specified period).
Let the decision variable
xij ∈ Z+ = the number of workers of type i ∈ T
assigned to station j ∈ S.
We can represent the cost at each station j as
gj i∈T kij xij wj qj uj , j ∈ S. The total system cost
depends on the cost at each station, and on system
parameters, such as cycle time and throughput. Thus,
we may represent the total cost as f j∈S gj c .
Here, gj and f are functions that are not necessarily expressible in closed form. We can formulate
a general representation of the resource-allocation
problem as
min z = f
gj c j∈S
ij
st mij ≤ xij ≤ m
xij ≤ nK
∀ i ∈ T j ∈ S
(1)
∀ K ∈ T
(2)
i∈K j∈S
wxj ≤ wmax qxj ≤ qmax umin ≤ uxj ≤ umax
(3)
Lee et al.: Modeling and Optimizing the Public-Health Infrastructure for Emergency Response
Interfaces 39(5), pp. 476–490, © 2009 INFORMS
x ≥ max xij ∈ Z+
cx ≤ cmax ∀ i ∈ T j ∈ S
(4)
(5)
POD-Location Model
To model the POD-location problem and population
needs, we first discretize the targeted region into grids
(e.g., one mile by one mile), where each grid has
a specified population according to census information. A selection of potential POD locations lies within
these grids. Let k be the total number of jurisdictions
in the region. The parameters in the model include
Gi =
dr l =
dmax =
cl =
pr =
set of grids in jurisdiction i;
distance between grids r and l;
maximum allowed travel distance;
the capacity of the facility at grid l; and
population of grid r.
Let the decision variable
yl = 1 if facility site at grid l is selected for setting
up a dispensing facility, 0 otherwise;
xrl = 1 if the population in grid r is served by the
facility at grid l, 0 otherwise.
We can formulate the capacitated POD-location problem as follows:
(COVER-CAP)
min
k yl
i=1 l∈Gi
s.t.
yl ≥ 2
∀ i = 1 k
(6)
l∈Gi
dr lxrl ≤ dmax yl
∀ r l ∈ Gi i = 1 k
(7)
xrl = 1 ∀ r ∈ Gi i = 1 k
(8)
xrl pr ≤ cl
(9)
l∈Gi
∀l ∈ Gi i = 1k
r∈Gi
xrl yl ∈ 0 1
∀ r l ∈ Gi i = 1 k
(10)
Constraint (6) ensures that at least two PODs are
opened. This is required if a catastrophic event at
one site necessitates shutting down a POD; in such
a case, emergency dispensing can still be carried out
in the remaining location. Constraint (7) ensures that
489
each household will travel at most dmax miles, constraint (8) ensures that each household is served, and
constraint (9) represents the capacity of the facility.
Let
ni = number of facilities in jurisdiction i as determined by COVER-CAP.
MINAVG-CAP minimizes the distance traveled by all
households, ki=1 r∈Gi l∈Gi xrl dr lpr , while satisfying the constraint sets (7)–(10). Constraint (6) for
MINAVG-CAP is given by l∈Gi yl = ni ∀i = 1 k,
where ni is the number of PODs required for jurisdiction i as returned by COVER-CAP. When there
is no sharing of staff resources, these two problems can be solved independently for each jurisdiction. For each jurisdiction, COVER-CAP and
MINAVG-CAP have identical problem sizes, with k +
k
k
2
2
i=1 Gi + 2Gi constraints and
i=1 Gi + Gi 0/1
variables. Although there have been many computational advances in facility location, the general problem remains NP-hard.
Acknowledgments
The material and results reported herein are based on
our work in this area and interaction with public-health
agencies. We are grateful to have had the opportunity
to participate in exercise drills and time-motion studies,
and to have had discussions with many state and federal
public-health and emergency-response experts. Although
we would like to thank many people who took part in
this multiagency and multidisciplinary collaboration, we
would like to particularly thank Jacquelyn Mason of the
CDC and Tom Tubesing, formerly of the CDC; Dr. Duane
Caneva, Dr. James Lawler, and Dr. Carter Mecher at the
White House Homeland Security Council; William Glisson at ESi; Bernard Hicks at the DeKalb Emergency Preparedness Department; and the many public-health and
emergency managers throughout the nation who have used
RealOpt. We thank the Wagner judges for their comments
that helped to improve this paper. We acknowledge funding from CDC to conduct the time-motion study and postevent operations analysis, and from the National Institutes
of Health for translational biomedical informatics advances.
This research was funded by the National Institutes of
Health, and the author will add the Web-published pdf file
of the article to the National Library of Medicine’s PubMed
Central database no later than 12 months after publication.
The findings and conclusions in this report are those of
the authors and do not necessarily represent the official
position of the CDC.
490
Lee et al.: Modeling and Optimizing the Public-Health Infrastructure for Emergency Response
References
Aaby, K., J. W. Herrmann, C. S. Jordan, M. Treadwell, K. Wein. 2006.
Montgomery County’s public health service uses operations
research to plan emergency mass dispensing and vaccination
clinics. Interfaces 36(6) 569–579.
Aickelin, U. 2002. An indirect genetic algorithm for set covering
problems. J. Oper. Res. Soc. 53(10) 1118–1126.
Anderson, R. M., R. M. May, E. Anderson. 1992. Infectious Disease of Human: Dynamics and Control. Oxford University Press,
Oxford, UK.
Beaton, R. D., M. W. Oberle, J. Wicklund, A. Stevermer, J. Boase,
D. Owens. 2003. Evaluation of the Washington State National
Pharmaceutical Stockpile dispensing exercise: Part I—Patient
volunteer findings. J. Public Health Management Practice 9(5)
368–376.
Diekmann, O., J. A. P. Heesterbeek. 2000. Mathematical Epidemiology
of Infectious Disease: Model Building, Analysis and Interpretation.
John Wiley & Sons, New York.
Ferguson, N., D. A. T. Cummings, C. Fraser, J. C. Cajka, P. C.
Cooley, D. S. Burke. 2006. Strategies for mitigating an influenza
pandemic. Nature 442(7101) 448–452.
Ferguson, N. M., D. A. Cummings, S. Cauchemez, C. Fraser,
S. Riley, A. Meeyai, S. Lamsirthaworn, D. S. Burke. 2005. Strategies for containing an emerging influenza pandemic in Southeast Asia. Nature 437(7056) 209–214.
Gebbie, K. M., J. Valas, J. Merrill, S. Morse. 2006. Role of exercises and drills in the evaluation of public health in emergency
response. Prehospital Disaster Medicine 21(3) 173–182.
Gerberding, J. L. 2003. The smallpox vaccination plan: Challenges and next steps. Testimony, US Senate Hearing 108-146
(January 30), Committee on Health, Education, Labor, and
Pensions, United States Department of Health and Human
Services, Washington, DC.
Germann, T. C., K. Kadau, I. M. Longini Jr., C. A. Macken. 2006.
Mitigation strategies for pandemic influenza in the United
States. Proc. National Acad. Sci. 103(15) 5935–5940.
Giovachino, M., T. Calhoun, N. Carey, B. Coleman, G. Gonzalez,
B. Hardeman, B. McCue. 2005. Optimizing a District of
Columbia strategic national stockpile dispensing center.
J. Public-Health Management Practice 11(4) 282–290.
Kaplan, E. H., D. L. Craft, L. M. Wein. 2002. Emergency response to
a smallpox attack: The case for mass vaccination. Proc. National
Acad. Sci. 99(16) 10935–10940.
Kermack, W. O., A. G. McKendrick. 1991. Contributions to the
mathematical theory epidemics–I. Bull. Math. Biology 53(1–2)
33–55. [Reprinted from Proc. Roy. Soc. 115A 700–121, 1927.]
Lee, E. K. 2008. In case of emergency. OR/MS Today 35(1) 28–34.
Lee, E. K., M. Zaider. 2008. Operations research advances cancer
therapeutics. Interfaces 38(1) 5–25.
Interfaces 39(5), pp. 476–490, © 2009 INFORMS
Lee, E. K., A. Ansari, K. Caspary. 2009a. A decision tool for efficient
design of community reception centers for radiation emergencies. Working paper, Georgia Institute of Technology, Atlanta.
Lee, E. K., S. Maheshwary, J. Mason. 2005. Real-time staff allocation for emergency treatment response of biologic threats and
infectious disease outbreak. INFORMS William Pierskalla Best
Paper Award in Healthcare Management Science, November,
INFORMS, Hanover, MD.
Lee, E. K., S. Maheshwary, J. Mason, W. Glisson. 2006a. Decision
support system for mass dispensing of medications for infectious disease outbreaks and bioterrorist attacks. Ann. Oper. Res.
148(1) 25–53.
Lee, E. K., S. Maheshwary, J. Mason, W. Glisson. 2006b. Large-scale
dispensing for emergency response to bioterrorism and infectious disease outbreak. Interfaces 36(6) 591–607.
Lee, E. K., C. H. Chen, F. Pietz, B. Benecke. 2009b. Disease propagation analysis and mitigation strategies for effective mass
dispensing. Working paper, Georgia Institute of Technology,
Atlanta.
Lee, E. K., H. K. Smalley, Y. Zhang, F. Pietz, B. Benecke. 2009c. Facility location and multi-modality mass dispensing strategies and
emergency response for biodefense and infectious disease outbreaks. Internat. J. Risk Assessment Management 12(2–4) 311–351.
Lien, O., B. Maldin, C. Franco, G. K. Gronvall. 2006. Getting
medicine to millions: New strategies for mass distribution.
Biosecurity Bioterrorism: Biodefense Strategy Practice Sci. 4(2)
176–182.
Longini, I. M., Jr., A. Nizam, S. Xu, K. Ungchusak, W. Hanshaoworakul, D. A. Cummings, M. E. Halloran. 2005. Containing pandemic influenza at the source. Science 309(5737)
1083–1087.
Mason, J., M. Washington. 2003. Optimizing staff allocation in largescale dispensing centers. Report, Centers for Disease Control
and Prevention, Atlanta.
Moriarty, E. 2006. Software helps to deal with disaster. Atlanta Business Chronicle (April 28).
Nelson, C., N. Lurie, J. Wasserman. 2007. Assessing public health
emergency preparedness: Concepts, tools, and challenges.
Annual Rev. Public Health 28(April) 1–18.
RealOpt. 2003–2009. RealOpt© user manual—Software for public
health and medical preparedness, version 5. Atlanta. http://
www2.isye.gatech.edu/medicalor/research.htm#realopt.
Tan, S. 2008. Drive-through vaccination effort a success in
Amherst: 1,385 people receive hepatitis A booster. Buffalo News
(September 22).
Wein, L. M., D. L. Craft, E. H. Kaplan. 2003. Emergency
response to an anthrax attack. Proc. National Acad. Sci. 100(7)
4346–4351.