Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
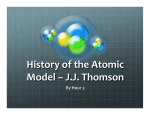
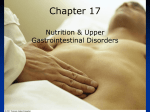
Chapter 15 Enteral & Parenteral Nutrition Support © 2007 Thomson - Wadsworth Nutrition Support • Enteral • Parenteral • Means “within or by means of the gastrointestinal tract.” Oral Known as tube feedings Preferred route if have adequate GI function Uses the veins Persons with inadequate GI function © 2007 Thomson - Wadsworth © 2007 Thomson - Wadsworth If you choose enteral nutrition support… • Must have • Types functional GI tract Standard (1.0-1.2cal/ml) • Tolerated by most patients Bowel sounds • Can be used alone or as a supplement • Variety of kinds of formulas Hydrolyzed • Partially or fully broken down • Persons with compromised GI functioning High calorie Disease-specific Modular • contain 1-2 macronutrients © 2007 Thomson - Wadsworth Enteral Nutrition Support • Provide Pro, CHO and Fat • Nutrient Density Protein = 8-29% of total kcalories Standard formulas • Carbohydrates = 4050% total kcalories • Fat = 30-45% total kcalories • Energy Density 0.5-2.0 kcalories per mL Standard formulas • 1.0-1.2 kcalories per mL • Patients with average fluid requirements Formulas with higher energy density • Smaller amount of fluid • Good for fluid restrictions © 2007 Thomson - Wadsworth Feeding Routes • Tube feeding less than 4 weeks • Tube feeding more than 4 weeks • Enterostomy Nasogastric • Postplorically Gastrostomy Jejunostomy Nasoduodenal Nasojejunal These tubes are weighted or non-weighted with stylets to guide placement • Orogastric Mouth to stomach Good for vent patients • Gastric feedings are the preferred route Easily tolerated & less complicated Not good for patients at risk for aspiration © 2007 Thomson - Wadsworth © 2007 Thomson - Wadsworth © 2007 Thomson - Wadsworth Osmolality • A solution’s tendency to shift from one fluid compartment to another across a semipermeable membrane • Range: 300-700 milliosmoles per kilogram • Isotonic: osmolality similar to blood • Hypertonic: osmolality greater than blood © 2007 Thomson - Wadsworth Enteral Nutrition in Medical Care • Preferred over parenteral • Can fully meet nutrient needs Helps maintain gut • Good for weak & Fewer complications debilitated patients Less costly • Oral preferred over • Nurses help patients find tube feedings appealing flavors Less stress Less complications Less costly © 2007 Thomson - Wadsworth Candidates for Tube Feedings • Severe swallowing problems • Little or no appetite • GI obstructions, impaired GI motility • Intestinal resections • Mentally incapacitated • Coma • Extremely high nutrient requirements • Mechanical ventilators © 2007 Thomson - Wadsworth Feeding Tubes • Soft & flexible • Variety of lengths & diameters • Outer diameter measured in French units © 2007 Thomson - Wadsworth Formula Selection • Need to assess Age Medical problems Nutritional status Ability to digest & absorb nutrients • Choose the one With the lowest risk of complications Lowest cost • Nutrition-related factors Energy, protein, & fluid requirements Need for fiber modification Individual tolerances (food allergies & sensitivities) © 2007 Thomson - Wadsworth © 2007 Thomson - Wadsworth What Formula? • Factors to consider GI function Calorie and protein density Ability to meet needs Type of • Protein, fat, CHO • Fiber © 2007 Thomson - Wadsworth Electrolytes Fluid Viscosity Osmolality Administration of Tube Feedings • Safe handling • Safety guidelines Clean equipment Clean hands • Open system Formula needs to be transferred from original packaging to feeding container • Closed system Formula is prepackaged Clean can opener & lid Refrigerate unused portions in clean, closed containers Discard unlabeled or unused within 24 hours Open system; hang no longer than 8-12 hour supply Closed system; hang no longer than 24-48 hour supply © 2007 Thomson - Wadsworth Tube Feeding • Formula delivery • Initiating tube feeding Intermittent Discuss with patient & family Check initial placement with X-ray Monitor its position throughout the day: can check fluid pH • Gastric, 2500-400 mL over 2040 minutes • Risk of aspiration Bolus • Gastric • Delivery of <500mL every 3-4 hours Continuous • Slowly at constant rate • 8-24 hours • Noctural © 2007 Thomson - Wadsworth Administering the Feeding • Formula volume & strength Varies among institutions Hypertonic fluids usually started slowly & volume gradually increased Assess patient tolerance • Checking gastric residuals Withdraw contents through feeding tube with syringe Intermittent before each feeding Continuous every 46 hrs © 2007 Thomson - Wadsworth Tube Feedings • Supplemental water Formulas are 6985% water More water comes from flushes via feeding tubes • Flush before & after each bolus or intermittent feeding • Flush every 4 hours for continuous • Count as intake • Transition to table foods Gradually shift to oral diet Oral needs to be 2/3 of nutrient intake before discontinuing the tube © 2007 Thomson - Wadsworth Tube Feedings • Delivering medications • Complications Nausea & diarrhea Mechanical problems Metabolic problems Need to consider diet-drug interactions Medications can clog tubes • Monitor patient’s Continuous: stop Weight feeding 15 minutes Hydration status before & after Lab test results medication administration © 2007 Thomson - Wadsworth Parenteral Nutrition Support © 2007 Thomson - Wadsworth Indications for Parenteral Nutrition • Short bowel syndrome • Severe pancreatitis • Malabsorption disorders • Intestinal obstructions or fistulas • Severe burns or trauma • Critical illnesses or wasting disorders • Bone marrow transplants • Malnourished & high risk for aspiration © 2007 Thomson - Wadsworth Venous Access • Peripheral Parenteral Nutrition (PPN) Peripheral veins Short-term support Patients with average nutrient needs & no fluid restrictions Veins can be damaged • Total Parental Nutrition (TPN) Larger, central veins Long-term support Patients with high nutrient needs or fluid restrictions • Need solutions under 800-900 mOsm © 2007 Thomson - Wadsworth © 2007 Thomson - Wadsworth Parenteral Solutions • Contain amino acids • Contain lipids All essential plus combinations of nonessential • Contain carbohydrates Dextrose, 3.4 kcalories/gram 2.5-70% concentrations >10% only for TPN Significant source of energy 10, 20% solutions Often provided daily & = 20-30% total kcalories Decreases risk of hyperglycemia from dextrose © 2007 Thomson - Wadsworth © 2007 Thomson - Wadsworth Parenteral Solutions • Fluid • Contain vitamins Need 1500-2500 mL/day for adults • Contain electrolytes All water-soluble plus A, D, & E K must be added separately Sodium, potassium, • Contain trace minerals chloride, calcium, magnesium, & Zinc, copper, chromium, phosphorus selenium, & manganese Expressed in Iron is excluded milliequivalents (mEq) © 2007 Thomson - Wadsworth Types of Parenteral Solutions • Total Nutrient Admixture (TNA) 3-in-1 solution Also called “all-in-one” solution Contains dextrose, amino acids, & lipids • 2-in-1 solution Dextrose & amino acids Lipids administered separately to provide essential fatty acids © 2007 Thomson - Wadsworth Administering Parenteral Nutrition • Team effort Physicians Dietitians Pharmacists Nurses: provide direct care • IV catheters Nurse can place in peripheral veins Physician must place in central veins • Problems Dislodging Air embolism Clotting Phlebitis Infection • Must use aseptic technique © 2007 Thomson - Wadsworth Parenteral Nutrition Complications • Mechanical complications • Infection and sepsis • Metabolic Complications • Gastrointestinal Complications © 2007 Thomson - Wadsworth Parenteral Solutions • Administering • Discontinuing Continuous • Critically ill • Malnourished Cyclic • 10-16 hours • Often provided at night Check tubing & solution daily for contamination When 2/3-3/4 of nutrient needs are provided by enteral feedings, IV can be discontinued Clear liquids Small enteral feedings to determine tolerance © 2007 Thomson - Wadsworth Managing Metabolic Complications • Hyperglycemia • Hypertriglyceridemia Patients who are glucose intolerant or in severe metabolic stress Provide insulin with feedings or decrease dextrose • Hypoglycemia When feedings are interrupted or discontinued Taper slowly Critically ill can’t tolerate lipid infusions Impaired lipid clearance • Refeeding syndrome Re-feed slowly Life-threatening • Abnormal liver function Long-term, can lead to liver failure Cause unclear © 2007 Thomson - Wadsworth Managing Metabolic Problems • Gallbladder disease Parenteral for more than 4 weeks Sludge builds up, leading to gallstones Cholecystokinin injections or remove gallbladder • Metabolic bone disease Long-term parenteral lowers bone density Alterations in calcium, phosphorus, & vitamin D metabolism © 2007 Thomson - Wadsworth Nutrition Support at Home • Candidates • Planning Enteral Enteral • Head & neck cancers • Neurological impairments affecting swallowing Parenteral • Portion of small intestine removed • Intestinal obstructions • Malabsorption conditions Nasal tubes or enterostomies Investigate cost & availability • Planning Parenteral Sterile & aseptically prepared Cyclic best © 2007 Thomson - Wadsworth Quality of Life Issues • • • • • Economic impact Time-consuming Inconvenient Disturbed sleep Activities & work must be planned around feedings • Social issues Inability to consume meals with friends & family Inability to go to restaurants & social events Fear, anxiety & depression © 2007 Thomson - Wadsworth Nutrition in Practice Ethical Issues in Nutrition Care © 2007 Thomson - Wadsworth Ethical Principles & Health Care • Patient autonomy The right to make own health care decisions • Disclosure Fully informed of treatment’s risks & benefits • Decision-making capacity • Treatment benefits (beneficence) should outweigh harm (maleficence) • Distributive justice Would care given to one patient unfairly limit the care of other patients? Mental capacity to make appropriate health care decisions © 2007 Thomson - Wadsworth Life-Sustaining Treatments • Nutrition support & hydration • Cardiopulmonary resuscitation (CPR) • Defibrillation • Mechanical ventilation • Dialysis © 2007 Thomson - Wadsworth Legal Documents for End of Life Care • Living will, medical directive • Durable power of attorney Written statement specifying medical procedures desired or not desired • Advanced directive Written or oral instruction regarding one’s preferences for medical treatment Another person is appointed to make health care decisions in the event of incapacitation • Do-not-resuscitate (DNR) Order to withhold CPR in the event of a cardiac arrest © 2007 Thomson - Wadsworth